Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
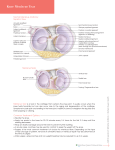
• Youtube video http://www.youtube.com/watch?v=MRGjy6AX69c Warning: You may want to look away at times! SPORTS INJURIES “Injuries may be forgiven, but not forgotten.” -Aesop Most Common Sports Injuries • • • • • • Groin Sprains Shin Splints Neck Stains Lower Back Injury Pulled Muscles Fractured bones • • • • • • Rotator Cuff tendinopathy Tennis Elbow Ankle Sprain Runner’s Knee Achilles Tendiopathy Knee Ligament rupture Most Common Causes of Injury • Failure to Warm UP • Over training • Excessive loading on the body • Not taking safety precautions • An Accident • Inappropriate equipment • • • • Poor Exercise Technique Reoccurring injury Genetic Factors Muscle weakness or imbalance • Lack of flexibility • Joint laxity • SHARP Swelling Heat Altered function Red Painful SIGNS of injuries • P.I.E.R principle Pressure Ice Elevation Restriction/Rest Treatment Sprains • • • • Relate to ligaments Tendons are strained. Pulls are associated with muscles Overuse or successive force- stretches or tears- tissues that connects bone 3 Categories (or Grades) of Injuries: • 1st degree – mild, least severe, a couple days to heal if treated properly *overstretched • 2nd degree- moderate but more severe, physiotherapy may be needed * partial tear • 3rd degree- most severe, surgery, physiotherapy, up to 12 months to recover *complete tear or rupture Ankle Sprain Most Common: Plantar Flexion or Inversion • • • • Anterior talofibular ligament Calcaneofibular ligament Posterior talofibular ligament Tibiofibular ligament (severe injury) Inversion sprain The Ankle Joint – Medial View Eversion sprains Occurs to the deltoid ligament The Ankle Joint – Lateral View Tibia Fibula Lateral malleolus Anterior tibiofibular ligament Posterior tibiofibular ligament Posterior talofibular ligament Calcaneofibular ligament Calcaneus Anterior talofibular ligament Ankle Sprain 1st Degree – inversion stress with foot in mild plantar flexion, stretching the anterior talofibular ligament 2nd Degree – tear anterior talofibular ligament, stretch and tear the calcaneofibular ligament 3rd Degree – grade III injury, varying degrees of injury to anterior talofibular, calcaneofibular, and posterior talofibular ligaments and joint capsule Symptoms and Signs 1st Degree Mild 2nd Degree 3rd Degree pain Partial tearing Complete sensation felt tear/rupture Point tenderness Swelling at Snap/Pop point tenderness sound Localized swelling (anterior at sprain site Severe pain talofibular Tenderness and ligament) swelling over entire lateral area Tearing of three ligaments Treatment 1st Degree 2nd Degree 3rd Degree PIER PIER PIER Limit X-ray X-ray Crutches Walking weightbearing activities Wrap when weight bearing No swelling – circumduction activites Weight bearing – tape Exercises 5-10 days Plantar and dorsiflexion exercises (if pain free) 1-2 weeks weight bearing Taping with walking Motion exercises Cold / heat application cast after swelling After circumduction exercises Progressive program of strengthening Joint Laxity: no end point Anterior Cruciate Ligament (ACL) • • • • Considered to be the most serious ligament injury to the knee Causes: Direct blow to knee Single-plane force –lower leg is rotated while the foot is fixed • Sharp cutting motion • Hyperextension from a force in front of knee • Non-contact Females and ACL Injuries Extrinsic factors • Level of conditioning, skill acquisition, playing style, amount of preparation and practice, environmental considerations, types of equipment used Intrinsic factors • Femoral intercondylar notch size, ACl size, ACL laxity, lower extremity anatomic malalignment (ie. Qangle) ** possible reasons why females are more likely to suffer noncontact ACL injuries Q-angle - Quadriceps angle • Formed in the frontal plane by a linedrawn from: • the centre of the patella to the anterior superior iliac spine, • and from the centre of the tibial tuberosity to the centre of the patella extending up the thigh • If angle created by the intersection of these two lines above the patella is greater than twenty degrees, this puts the individual at greater risk of experiencing knee injury Q-angle and ACL tears • Width of the pelvis determines size of Q-angle • women have a wider pelvis than men, the Q-angle tends to be greater • The forces are concentrated on the ligament each time the knee twists increasing the risk for an ACL tear • Proper stretching and strengthening is important Symptoms and Signs • • • • • • Experience a pop Immediate disability Knee feels like it is “coming apart” Rapid swelling at joint line Positive anterior drawer sign pivot-shift test, jerk test, and flexion-rotation drawer test may be positive • Decreased proprioception Treatment • • • • PIER Weight bearing support Physiotherapy Surgery? • Depends on athlete’s age, type of stress applied to knee, amount of stability present, techniques available to surgeon • May involve joint reconstruction, with transplantation of some external structure Achilles Tendon Rupture • Sports with stop and go action • Usually a result of sudden pushing-off action of the forefoot with the knee being forced into complete extension Symptoms and Signs • • • • • • • Feel a sudden snap (felt like something kicked him/her in lower leg) This will often be accompanied by a loud crack or bang. Immediate pain Point tenderness, swelling, discoloration There may be a gap felt in the tendon. Toe raising impossible Usually occurs 2-6cm proximal to its insertion onto the calcaneus Treatment - Surgical repair Rotator Cuff Tear • Involve one or four muscles • Supraspinatus, infraspinatus, teres minor, and subscapularis • Supraspinatus, infraspinatus, and teres minor share a common tendinous insertion on the greater tubercle of the humerus Shoulder Dislocation • Normal Dislocated Dislocation • Bone displaced from position • Damage to joint (synovial) capsule and ligaments between bones, muscles and tendons could tear • Signs: deformed joints, painful to move or touch, joint is unusable • Humerus “pops out” of the glenoid fossa • Usually a result of a hit or fall resulting in a tear to the glenohumeral ligament and joint capsule • Treatment should be done by a professional • Injury to the brachial plexus (vital nerves) and blood vessels if not done properly Shoulder Dislocation Shoulder Dislocation Inferior Dislocation Anterior Dislocation Separation • Bones held by ligaments tear or separate from each other • Shoulder separation • Tearing of acromioclavicular ligament union of clavicle to acromion) • Result from falls directly on shoulder (contact from another player or tumble on shoulder) Shoulder Separation Shoulder separations are classified as either 1st (mild), 2nd (moderate), or 3rd (severe) degree sprains. A 3rd degree AC joint sprain is the most severe with the result being what is termed a “stair step” deformity. This is when the end of the clavicle appears elevated because the ligament connecting the bones is completely torn. Torn Cartilage Cartilage is avascular Takes time to heal Often use arthroscopy: surgical procedure where incision made to allow a small fibre optic camera in to assess damage Shin splints • Overuse without adequate recovery • Pain along medial or lateral side of tibia along shaft • Caused by tearing of interosseous membrane (between tibia and fibula) or periosteum (lining of bone) • Causes: change in training regimen (frequency, duration or intensity), training surface (hard), poor shoes • Can develop into stress fractures Biceps Tendinitis • Overuse injury • Adequate rest is not given to the biceps brachii muscle when it has been worked or overloaded • Pain on the proximal end of biceps • Flexion of shoulder and elbow painful Tendinitis • Inflammation of a tendon caused by irritation due to prolonged or abnormal use “itis” means an inflammation to that particular organ or tissue Hematoma • A collection of pooled blood in the thigh within a relatively constricted area. • Example: thigh - probably accompany all serious contusions of the thigh • they are difficult to diagnose because of the large muscle mass in the thigh • may become calcified and form a hard lump in the quadriceps muscle. This lump is called osteomyositis ossificans and may cause stiffness or a bump in the muscle that may be very long lasting. Signs & Symptoms • Swelling at the injury site. • Feeling of tenseness to touch • Tenderness. • Redness that progresses through several colour changes-purple, green-yellow, yellow--before it completely heals. Treatment • PIER • anti-inflammatory medicine prescribed by your healthcare provider. • wearing an elastic thigh wrap when you return to sports • having prescribed physical therapy (including deep tissue treatments - ultrasound or electrical stimulation). • Complications: infection could develop in the wound, • the signs and symptoms might be increasingly severe pain, • a fever of 101 degrees or more, • swelling with surrounding redness, and pus. Groin Strain • Caused by strenuous stretching movements of the legs • Also sometimes with overuse of the adductor muscles • Symptoms: mild discomfort, pain against resistance, swelling and bruising in inner thigh • Usually take 4-6 weeks to heal but could be upwards of 8 weeks Patellofemoral Pain Syndrome • Causes: muscle weakness, muscle imbalance, tight tendons, abnormal movement of the kneecap • Signs and Symptoms: pain at front of knee, pain on pressure on knee, walking up stairs, running, swelling around kneecap, grinding or grating • Should see improvement over the few weeks of treatment, looking at 4-6 months of recovery time completely Patellofemoral Pain Syndrome • Treatment & Rehabilitation: • Rest the joint or cut back on the intensity of activity (exreduce practice or training schedule) • Strengthen the Quadriceps muscles (they support the knee) • Wear a knee brace or sleeve during activity • Wear an arch support or orthotic to prevent overpronation • Replace old shoes, which have been worn down from pronation • Anti-inflammatory drugs can be taken to reduce pain • Rehabilitation can last anywhere from one to eight weeks depending on the severity of the injury. Typically, athletes can continue their regular activities if the level of pain allows them to participate. Osgood Schlatter Disease • Description: condition of the knee where the tibial tuberosity becomes inflamed. The patellar tendon inserts on the tibial tuberosity and through overuse can tug away at the bone, causing pain and inflammation. • Symptoms: Pain around one or both knees , Pain when straightening the leg through the knee joint or full squat , Tibial tuberosity is swollen , Skin over tibial tuberosity is red, painful and inflamed , Pain when jumping or squatting Osgood Schlatter Disease • Causes: • Growth spurt: this condition tends to affect teenage children directly after a growth spurt. In addition, children that are active and engage in sports are at an increased risk. • Treatment and Rehabilitation: • Strengthening the quadriceps and hamstring groups • Avoiding physical activities that require frequent knee bending for two-four months • Wearing a knee brace or knee sleeve to restrict movement • Anti-inflammatory drugs may be taken to control pain and inflammation • Increasing flexibility in the quadriceps and hamstring muscles Sports Injury Facts • More than 3.5 million children ages 14 and under receive medical treatment for sports injuries each year. • Injuries associated with participation in sports and recreational activities account for 21 percent of all traumatic brain injuries among children in the United States. • Overuse injury, which occurs over time from repeated motion, is responsible for nearly half of all sports injuries to middle-and high-school students. Immature bones, insufficient rest after an injury and poor training or conditioning contribute to overuse injuries among children. • Most organized sports related injuries (62 percent) occur during practices rather than games. Despite this fact, a third of parents often do not take the same safety precautions during their child's practices as they would for a game. • A recent survey found that among athletes ages 5 to 14, 15 percent of basketball players, 28 percent of football players, 22 percent of soccer players, 25 percent of baseball players and 12 percent of softball players have been injured while playing their respective sports. • Children ages 5 to 14 account for nearly 40 percent of all sports-related injuries treated in hospital emergency departments. The rate and severity of sports-related injury increases with a child's age.