Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Chagas disease wikipedia , lookup
Oesophagostomum wikipedia , lookup
Gastroenteritis wikipedia , lookup
Orthohantavirus wikipedia , lookup
Typhoid fever wikipedia , lookup
Lyme disease wikipedia , lookup
Marburg virus disease wikipedia , lookup
Meningococcal disease wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Leptospirosis wikipedia , lookup
Infectious mononucleosis wikipedia , lookup
Schistosomiasis wikipedia , lookup
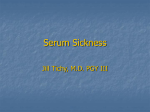
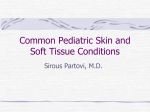
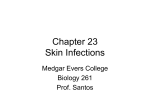
CASE 5: “RASH JUDGMENT” Questions to be answered 1. 2. 3. 4. 5. 6. 7. How are rashes classified? What infectious conditions are to be entertained in Michelle’s case? Are there non-infectious conditions that may present with rashes? In view of the general presentation, what is the most likely diagnosis of Michelle’s case? Discuss the possible complications of her condition Discuss the treatment of Michelle’s case Discuss the measure/s necessary to prevent infection with the viral exanthems that present with maculopapular rash “RASH JUDGMENT” • Michelle is a 10-year old girl with fever for the last five days. Associated symptoms include brassy cough and coryza, watery diarrhea and decreased appetite. Two days later, she was noted to have “sore eyes” and irritability. • The mother could not recall the child’s immunizations except that she was given the last vaccines at the health center at age 4 months “RASH JUDGMENT” • On examination, she looked tired and ill, and had a temperature of 390C; CR 88/min. and RR 26/min.. She had a rash that started 8 – 12 hrs. earlier behind the ears and on the face then spread down the body. The rash was erythematous with fine macules and papules. Conjunctivitis was prominent. On examination of the buccal mucosa, small 1-mm.white papules were seen opposite the 2nd molars. “RASH JUDGMENT” • 2 days later, the white spots disappeared and the palms and soles were involved in the erythematous rash which later became brownish. This was later followed by a fine branny desquamation first occurring in the face later involving the body. Q1: How are rashes classified ? (judged) RASH JUDGMENT • A exanthem is a skin eruption occurring as an integral part of an infectious disease. The corresponding changes in the mucous membranes is an enanthem • Accurate diagnosis not always possible on preliminary examination- judgment should be deferred until rash develops Morphologic types or Components of a rash • Macule is a circumscribed discoloration of the skin. Often evolve into papules. Papules are small nodular elevations of the skin • Vesicles are small blisters containing clear fluid. Pustules are small elevations of the skin containing pus Maculopapular rash Vesiculopustular rash Morphologic types or Components of a rash • Petechiae are small hemorrhages beneath the epidermis. Ecchymoses are larger areas of hemorrhage Color Atlas of Infectious Diseases, Emond & Rowland Other components • Crust/scab – congealed exudate on the skin • Wheal – localised effusion of fluid into the skin causing a raised, white or pinkishwhite zone with a halo of erythema • Erythema – a diffuse or localised red ness of the skin Vital information necessary in the diagnosis of exanthematous illnesses Exposure Season Incubation period Age Previous exanthem Relation of rash to fever Adenopathy Type of rash Distribution of rash Progression of rash Exanthems Other associated symptoms or Prodrome Laboratory tests Feigin and Cherry Textbook of Pediatric Infectious Diseases Basis for Rash Judgment: 1. Prodromal period 2. Rash 3. Presence of pathognomonic or other diagnostic signs 4. Laboratory diagnostic tests Q2: What infectious conditions are to be entertained in Michelle’s case? Conditions that present with Maculopapular rash 1. Measles • Prodromal period: – The rash is preceded by a 3 or 4 day period of fever, conjunctivitis, coryza and cough • Rash: – reddish brown, appears on the face first and progresses downward to involve the trunk and extremities in sequence Measles • Rash (cont.): The eruption fades by the 5th or 6th day with brownish staining first followed by branny desquamation. The hands and feet do not desquamate Brownish discoloration Measles • Pathognomonic sign: Koplik’s spots – Detected on the mucosa of the cheeks opposite the molars, where they resemble coarse grains of salt on the surface of the inflamed membrane. • Histologically are small necrotic patches in basal layers of the mucosa with serum exudation and mononuclear cell infiltration Measles course Conditions that present with Maculopapular rash 2. Rubella (Postnatal) • Prodromal period: – In children there are no prodromal period. The appearance of the rash and preceding lymphadenopathy may be the first obvious sign of disease. – Adults and adolescents may have a variable period of malaise and low-grade fever before the rash appears Rubella rash Rubella course Postnatal Rubella • Rash: – Not distinctive; initially discrete, delicate pink macules beginning on face and neck and progresses downward to the trunk & extremities more rapidly than measles. On the third day the face is usually clear – Does not desquamate Postnatal Rubella • Forchheimer spots – red spots are often seen on the palate – Exceptionally profuse in this patient Rubella • Diagnostic sign: – lymphadenopathy (particularly postauricular and occipital) is a common manifestation, but it also occurs in other diseases • Laboratory diagnosis: – positive throat culture for rubella virus and rise in antibody level are helpful diagnostic aids Congenital Rubella Syndrome • “Blueberry muffin” rash: a purpuric rash may present at birth or develop within 48 hrs. • May be accompanied by bleeding from the mucosal surface Conditions that present with Maculopapular rash 3. Roseola infantum • Prodromal period: – a 3 or 4 day period of high fever and irritability precedes the rash which appears as the temperature falls to normal Roseola infantum (HHV 6) • Rash: – typically discrete rose-red maculopapules that frequently appear on the chest and trunk first and then spread to involve the face and extremities. – The eruption usually disappears within 2 days. Occasionally within several hours Roseola infantum • Diagnostic sign: – The coincidental appearance of the rash with defervescence in an infant is distinctive • Laboratory diagnostic test: – none locally commercially available Conditions that present with Maculopapular rash 4. Erythema infectiosum: Rash: erupts in 3 stages 1. Red, flushed cheeks with circumoral pallor (“slapped check” appearance) 2. Maculopapular eruption over upper and lower extremities (the rash assumes a lacelike appearance as it fades) Erythema infectiosum Lacelike pattern of rash Slapped-face appearance Erythema infectiosum • Rash (cont.) 3. An evanescent stage characterized by subsidence of the eruption followed by recurrence precipitated by a variety of skin irritants • Diagnostic sign: – • suggested by the slapped-face appearance in a well child Laboratory diagnosis: – future serologic tests to confirm parvovirus B19 Conditions that present with Maculopapular rash 5. Infectious mononucleosis • Rash – pinkish maculopapular, often mistaken for rubella – Tends to be patchy and heavier on the limbs Infectious mononucleosis • Diagnostic signs: – a triad of membranous tonsillitis, lymphadenopathy and splenomegaly suggests this • Laboratory diagnostic test: – blood smear positive for abnormal lymphocytes. – Monospot test and heterophil agglutination (Paul-Bunnell) test are positive Infectious mononucleosis • Hoagland’s sign: lid edema 6. Enteroviral Infections • Prodrome: – Echovirus 16 (Boston exanthem) prodrome resemble exanthem subitum but fever lower – Fever & constitutional symptoms in Echovirus 4, 6 & 9 may precede but usually coincide with rash appearance ECHOvirus type 19 infection • Rash: – May be maculopapular, petechial and vesicular eruptions with Coxsackie A9, A16,A10, A5,B3 and B5 Cochsackievirus infection 7. Mucocutaneous Lymph Node Syndrome (Kawasaki disease) • Prodrome: – A nonspecific febrile illness with sore throat precedes the rash by 2 – 5 days • Rash: – Generalized, erythematous, maculopapular. The palms and soles are swollen and reddened, eventually peeling after several days or weeks. Mucocutaneous Lymph Node Syndrome (Kawasaki disease) • Rash (cont.) – Dryness with erythema of the lips (red strawberry tongue), mouth and tongue accompanies bilateral conjunctival injection Mucocutaneous Lymph Node Syndrome (Kawasaki disease) • Conjunctivitis – Bilateral, bulbar, generally nonpurulent • Cervical lymphadenopathy – Usually unilateral – Not explained by other known disease process Mucocutaneous Lymph Node Syndrome (Kawasaki disease • Periungual desquamation or • Perianal desquamation may follow in the subacute phase Diagnostic Criteria for Kawasaki Disease • • Fever lasting for at least 5 days Presence of at least 4 of the ff. 5 signs: – – – – – Bilateral bulbar conjunctival injection, generally nonpurulent Changes in the mucosa of the oropharynx, including injected pharynx, injected and/or dry fissured lips, strawberry tongue Changes of the peripheral extremities, such as edema and/or erythema of the hands or feet in the acute phase; or periungual desquamation in the subacute phase Rash, primarily truncal; polymorphous or nonvesicular Cervical adenopathy, > 1.5 cm., usually unilateral lymphadenopathy illness not explained by other known disease process 8. Staphylococcal Scalded Skin Syndrome • Prodrome: – None – Fever and irritability occur at the time of onset of the rash • Rash: – Generalized, erythematous, scarlatiniform eruption with sandpaper-like texture Staphylococcal Scalded Skin Syndrome • Rash (cont) – The erythema is accentuated in the skin folds. – The skin is tender and within 1-2 days, bullae appear and the epidermis separate into large sheets, revealing a moist, red, shiny surface underneath (Nikolsky sign) Ritter’s disease Staphylococcal Scalded Skin Syndrome variants + Nikolsky sign Lyell’s disease Lyell’s disease Toxic Epidermal Necrolysis Staphylococcal Scalded Skin Syndrome variants Newborns – Ritters disease or Pemphigus neonatorum Older children and adults – Lyell’s disease or Toxic Epidermal Necrolysis – TEN differentiated from SSS by intraepithelial splitting at the dermoepidermal junction – TEN usually drug-induced from phenytoin, phenobarbital, sulfonamides, penicillin Toxic epidermal Necrolysis Staphylococcal Scalded Skin Syndrome variants • Diagnostic sign: – An associated staphylococcal infection e.g. Impetigo or purulent conjunctivitis may be present • Laboratory diagnostic tests: – Culture of skin positive for phage group II 9. Staphylococcal Toxic Shock Syndrome • Prodrome: – High fever, headache confusion, sore throat, vomiting, diarrhea and shock may precede or may be associated with the rash • Rash – There are no characteristic features of the rash – Occurs most prominently in the trunk & extremities – Associated with edema and desquamation Poor capillary refill in TSS Staphylococcal Toxic Shock Syndrome • Diagnostic signs: – The scarlatiniform eruption is associated with high fever, toxicity and a shock-like state • Laboratory tests: – Cultures of various mucosal surfaces or purulent lesions should be positive for Staphylococcus aureus 10. Typhoid fever • Rash: – Rose spot • Typically appear towards the end of the 1st week • Present in 50% of adults but less common in children • Difficult to detect on dark skin • Districuted over abdomen, chest and back but rarely seen in face, hands or feet – Step-ladder temperature chart Q3: Are there non-infectious conditions that may present with rashes? Noninfectious conditions • Drug eruptions/toxic erythemas • Sunburn • Miliaria – No prodromal periods – Sunburn rashes confined to the areas not protected by clothing – Miliaria: fine punctiform lesions are chiefly confined to the flexor areas. Rash not usually generalized and does not desquamate Drug Eruptions…Others Erythema multiforme from sulphonamide Urticaria caused by Penicillin Malar “butterfly Rash” of Systemic Lupus erythematosus Q4: In view of the general presentation, what is the most likely diagnosis of Michelle’s case? Task 5: Discuss the possible complications of her condition Task 6: Discuss the treatment of Michelle’s case Task 7: Discuss the measure/s necessary to prevent infection with the viral exanthems that present with maculopapular Task 8: Enumerate possible Key Learning points in Michelle’s case CASE 5: “RASH JUDGMENT”