Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
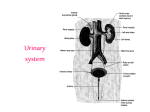
HEMATURIA AND EXAMINATION OF THE URINE 汇报提纲 1 Hematuria 2 Proteinuria 3 Appearance of urine 4 Volume of urine 5 Specific gravity and osmolality 6 PH (potential of hydrogen) Hematuria Type microscopic hematuria defined as 4 erythrocytes per high-powered field on a spun urine specimen gross hematuria bloody urine ,indicates sufficient red blood cells to discolor the urine Clinical occurrence 1.systemic disease blood disease, congenital hemophilia, sickle cell disease, leukaemia, thrombocytopenia, bleeding disorders, including anticoagulant drugs; scurvy. vitamin K deficiency 2.Infective disease epidemic hemorrhagic fever, ichorrhemia, epidemic meningitis; 3.Cardiovascular disease: infective endocarditis, Malignant hypertension, congestive heart failure; 4.Urinary system disease diastrophic erythrocyturia: glomerular hematuria glomerular disease: acute glomerulonephritis, nephrotic syndrome, orthomorphic erythrocyturia: non-glomerular hematuria non-renal source: infarct/papillary necrosis, trauma , pyelitis, stones, renal tumours/ infection/tuberculosis, kidney injury of drugs (e.g.,sulfonsmides, nonsteroidal, antiinflammatory drug or mannitol), renal infarction. post renal: Ureteric/bladder stone; ureteric /bladder/ prostate cancers; bladder tuberculosis, infectious urethritis, prostatitis, interstitial/bacterial cystitis ; urethral stricture , Urethral neoplasma 5 others Radiation nephritis or cystitis, metabolic/toxic hemorrhagic cystit is( e.g. cyclophosphamide or ifosfamide) ,analgesic Nephropathy, anticoagulants 6 functional heavy exercise, fever, post surgical. Clinical feature 1Change of color: • Microscopic hematuria: normal • Gross hematuria: color change according to the amount of bleeding. • Renal bleeding---dark red • Bladder/prostate bleeding---Bright red • Red color urine is not all hematuria: haemoglobinuria or myoglobinuria Normal chyluria hematuria haemoglobinuria 2.Source of blood: initial hematuria: urethra terminal hematuria : the trigone region of the bladder or prostate total hematuria : the kidney or ureter. erythrocyte casts :proves a renal source 3.Microscopic hematuria found only on chemical testing, judge renal source or not renal source diastrophic erythrocyturia ----glomerular hematuria Red cells size differ, shape multiplicity orthomorphic erythrocyturia---- non- glomerular hematuria renal pelvis calices, Ureteric, bladder , prostate Red cells shape unity 4.symptomatic hematuria renal region dull pain or colicky pain – renal disease frequent micturition, urgent micturition, Dysuria—bladder, urethra 5.asymptomatic hematuria the early stage of some disease tuberculosis of kidney, renal carcinoma or bladder carcinoma, hiding nephritis Test • Stix test followed by microscopy fresh urine, exception of menstruating confirm the presence of red cells , exclude haemoglobinuria or myoglobinuria. . detect red-cell casts, which are diagnostic of glomerulonephritis. • In the absence of red-cell casts, further investigations, such as urine cytology, renal imaging and cystoscopy, are required to define the site of bleeding. • Renal biopsy may be required Proteinuria • Proteinuria is one of the most common signs of renal disease. Detection is primarily by Stix testing. • Most reagent strips can detect protein if albuminuria exceeds 300 mg/d. • Most reagent strips react primarily with albumin and are relatively insensitive to globulin and Bence Jones proteins. • Excretion in 24 hour urine collections should be measured. • Healthy adults excrete up to 30 mg daily of albumin. • fever, exercise and adoption of the upright posture (postural proteinuria) all increase urinary protein output but are benign. Appearance Little value except diagnosis of hematuria Very concentrated urine appear dark . Discoloration of urine: cholestatic jaundice, haemoglobinuria, drugs such as rifampicin, use of fluorescein or methylene blue, and ingestion of beetroot. after standing for some time occurs in porphyria, ingesting the drug L-dopa. Volume Determined by diet and fluid intake. Normal 1000–2000 ml/d The minimum amount 650ml/d to stay in fluid balance. oliguria <400ml /d anuria <100ml/d polyuria>2500ml /d Chronic kidney disease or diabetes, insipidus, impairment of concentrating ability requires increased volumes of urine to be passed, given the same daily solute output. An increased solute output, such as in glycosuria or increased protein catabolism following surgery, also demands increased urine volumes. Specific gravity and osmolality • Urine specific gravity is a measure of the weight of dissolved particles in urine, whereas urine osmolality reflects the number of such particles. • Measurement of is required only in the differential diagnosis of oliguric renal failure or the investigation of polyuria or inappropriate ADH secretion. • Specific gravity1.015-1.025 , • Specific gravity is usually fixed at 1.010 in CKD or acute tubular necrosis as compared to prerenal acute kidney injury and inappropriate ADH secretion where specific gravity is very high close to 1.025. Urine PH • Measurement of urinary pH is nnecessary except in the investigation and treatment of renal tubular acidosis. • 6.5 Dysmorphic Rbc Glomerular disease hematuria Hemogeneous Rbc Calculus,tumor, TB,infection • proteinuria>150mg/24hr Proteinuria analysis glomerular >1.5g/24hr Selective Non Selective (albumin) (mixture) tubular overflow secretory or <1.5g/24hr immunoglobulin histic Β2-micro globulin Bence Jones protein Infection toxicity myeloma • 10cm in length • 5cm in width • 4cm in thickness • 134 ~ 148g in weight Renal Cortex • renal cortex – 80~90% of glomerulus – Glomerular capsule • renal medulla – renal tubule