Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
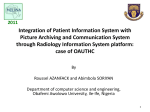
The Virtual Night Hospital Dr Philip Shorvon Central Middlesex Hospital London FACTORS PROFESSIONAL SHORTAGE RADIOLOGISTS INCREASING WORKLOAD HEAVY CONSULTANT ON- ALL COMMITMENT PARTICULARLY IN NON-TEACHING HOSPITALS INCREASING COMPLEXITY OF WORK LESS EXPERIENCE OF JUNIOR CONSULTANTS FACTORS ORGANISATIONAL NETWORKED SERVICES- ORTHOPAEDICS/ NEUROSCIENCES/ VASCULAR /ONCOLOGY EUROPEAN WORKING TIME DIRECTIVE NIGHT HOSPITAL ‘SMALL DGH’ MODEL FACTORS IMAGING AND IT INCREASING USE OF IMAGING OUT OF HOURS FOR TRIAGE NICE GUIDELINES FOR HEAD CT INCREASE USE OF EMERGENCY CT IN ABDOMINAL AND CHEST CONDITIONS RAPID INCREASE IN PACS SYSTEMS IT ADVANCES ( NHS NET/BROADBAND ETC) NIGHT HOSPITAL CONCEPT INCREASING USE OF EXTENDED ROLES REDUCED NUMBER OF MEDICAL PERSONNEL ON SITE MORE CONSULTANT LED SERVICES CENTRAL MIDDLESEX HOSPITAL Innovation to survive 2nd hospital to get trust status Lead patient focussed concept One of first PFI type deals for MRI (1993) First DTC to be built (ACAD in 1999) New build underway (BECaD) Now merged with Northwick Park Hospital (NorthWest London Hospitals NHS Trust) CENTRAL MIDDLESEX HOSPITAL 250K catchment area Highly disadvantaged population ( 40K refugees and > 50% population English not first language) 80K A and E attendances / year 10K emergency admissions / year Bedbase 250 approx CMH- BECAD (Brent Emergency Care and Diagnostic Centre) DOH model of the “small district general hospital- (www.dh.gov.uk/policyand guidance/organisationpolicy/configuringhospitals) Innovations over staffing/hospital at night Filmless environment THE VIRTUAL NIGHT HOSPITAL ? THE SOLUTION • Several hospitals link their PACS systems to a central reporting site • Portable video conferencing to referring hospitals (discussions with radiographers/ referring clinicians/ even patients?) • Consultant opinions at central reporting site - Radiology, A and E , ? Cardiology? others Virtual Night Hospital Work-Flow Hospital A Image Repository & PACS Gateway n Hospital B Hospital A Examinations for Reporting are sent to the VNH Image Repository & PACS Gateway (DICOM “processed” to support multiple PACS Vendors) Hospital B Hospital A Examinations reported directly into the On-Call Worksation and sent back to the Repository On-Call Workstation Hospital B Hospital A Teleconference Facilities make it possible to communicate between sites in real-time. This may also include streaming images such as Ultrasound. Hospital B Hospital A Examinations reported directly into the On-Call Worksation and sent back to the Repository On-Call Workstation Hospital B Hospital A Images and Report made immediately available via Web Based Viewer to referring site. On-Call Workstation Hospital B Report may also be exported into RIS system. Hospital A Fully Reciprocal Arrangement Hospital B Highly Scalable Hospital C Hospital E Hospital A Image Repository & PACS Gateway Hospital B Hospital F Hospital D THE VIRTUAL NIGHT HOSPITAL RADIOLOGY ALL OUT OF HOURS PLAIN FILM AND CT REPORTING PERFORMED AT THE TIME VIDEO CONFERENCING ALLOW CLINICAL DISCUSSIONS/ PROTOCOL MANAGEMENT FOR CT THE VIRTUAL NIGHT HOSPITAL RADIOLOGY PROBLEMS INTERVENTIONAL ?- will require separate ULTRASOUND?- X training nurse practioners interventional rotas. If organised regionally, interventionalists could cover several hospitals (already beginning with vascular networks (gynae), A and E – FAST. Videostreaming and remote robotic ultrasound possible THE VIRTUAL NIGHT HOSPITAL RADIOLOGY INDIRECT ADVANTAGES Radiologist- Much reduced on-call commitment. Busy when on call but following day off A and E films reported on time- less returns/ misses Good acute training opportunities Patients- 24 hour access to consultant opinion THE VIRTUAL NIGHT HOSPITAL WHEN? Need working model by early 2006commissioning of BECaD THE VIRTUAL NIGHT HOSPITAL WHERE ARE WE NOW? 3. Gaining political support Identifying funding Investigating technology 4. Looking for partners 1. 2. THE VIRTUAL NIGHT HOSPITAL WHERE ARE WE NOW? Technology PACS-Workstation which can receive different PACS company data/ PACS to PACS translation (Insignia) WEB based return of reports Portable video conferencing- on 3G networks or via broadband- liaising with Kingston University Robotic Ultrasound - assessment THE VIRTUAL NIGHT HOSPITAL WAY FORWARD IF ANY HOSPITALS WITH PACS ARE INTERESTED IN CONTRIBUTING TO A PILOT STUDY OF THIS CONCEPTPLEASE CONTACT MYSELF OR DAVID POWELL (PROJECT LEADER FOR THE BECaD) [email protected] [email protected] Or Mary McKenna on 02084532270