Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
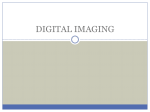
Computed Radiography By Prof. Stelmark Presently, an acceleration in the conversion from screen-film radiography (analog) to digital radiography (DR) is occurring. Digital imaging began with computed tomography (CT) and magnetic resonance imaging (MRI). DR was introduced in 1981 by Fuji with the first commercial computed radiography (CR) imaging system. After many improvements that were made over the next decade, CR became clinically acceptable and today enjoys widespread use. To conduct a screen-film radiographic examination, one should first produce a paper trail of the study, then process the image with wet chemistry, and finally physically file the image after accepting that it is diagnostic. CR imaging eliminates some of these steps and can produce better medical images at lower patient dose. THE COMPUTED RADIOGRAPHY IMAGE RECEPTOR Many similarities have been observed between screen-film imaging and CR imaging. Both modalities use as the image receptor an x-ray sensitive plate that is encased in a protective cassette. The two techniques can be used interchangeably with any x-ray imaging system. Both carry a latent image, albeit in a different form, that must be made visible via processing. Here, however, the similarities stop. In screen-film radiography, the radiographic intensifying screen is a scintillator that emits light in response to an x-ray interaction. In CR, the response to x-ray interaction is seen as trapped electrons in a higher-energy metastable state. Photostimulable Luminescence Some materials such as barium fluorohalide with europium (BaFBr:Eu or BaFI:Eu) emit some light promptly, in the way that a scintillator does following x-ray exposure. However, they also emit light some time later when exposed to a different light source. Such a process is called photostimulable luminescence (PSL). The europium (Eu) is present in only very small amounts. It is an activator and is responsible for the storage property of the PSL. The activator is similar to the sensitivity center of a film emulsion because without it, there would be no latent image. Over time, these metastable electrons return to the ground state on their own. However, this return to the ground state can be accelerated or stimulated by exposing the phosphor to intense infrared light from a laser—hence the term photostimulable luminescence from a photostimulable phosphor (PSP). The PSP, barium fluorohalide is fashioned similarly to a radiographic intensifying screen. Because the latent image occurs in the form of metastable electrons, such screens are called storage phosphor screens (SPSs). SPSs are mechanically stable, electrostatically protected, and fashioned to optimize the intensity of stimulated light. Some SPSs incorporate phosphors grown as linear filaments that enhance the absorption of x-rays and limit the spread of stimulated emission. Cross section of a photostimulable phosphor (PSP) screen Some storage phosphor screens (SPSs) incorporate phosphors grown as linear filaments that increase the absorption of x-rays and limit the spread of stimulated emission. Imaging Plate The PSP screen is housed in a rugged cassette and appears similar to a screen-film cassette . In this form as an image receptor, the PSP screen-film cassette is called an imaging plate (IP). The IP is handled in the same manner as a screen-film cassette; in fact, this is a principal advantage of CR. CR can be substituted for screen-film radiography and used with any x-ray imaging system. The PSP screen of the IP is not loaded and unloaded in a dark room. Rather, it is handled in the manner of a screen-film daylight loader. When an x-ray beam exposes a PSP, the energy transfer results in excitation of electrons into a metastable state. Approximately 50% of these electrons return to their ground state immediately, resulting in prompt emission of light, with wavelength λe. The remaining metastable electrons return to the ground state over time. This causes the latent image to fade and requires that the IP must be read soon after exposure. CR signal loss is objectionable after approximately 8 hours. When the CR cassette is inserted into the CR reader, the IP is removed and is fitted to a precision drive mechanism. This drive mechanism moves the IP constantly, yet slowly (“slow scan”) along the long axis of the IP. Small fluctuations in velocity can result in banding artifacts, so the motor drive must be absolutely constant. While the IP is being transported in the slow scan direction, a deflection device such as a rotating polygon or an oscillating mirror deflects the laser beam back and forth across the IP. This is the fast scan mode. ADC IMAGING CHARACTERISTICS Medical imaging with CR is not much different from that with screen-film imaging. A cassette is exposed with an existing x-ray imaging system to form a latent image. The cassette is inserted into an automatic processor (reader) and the latent image is made manifest. In CR and DR, it is not really a characteristic curve but rather an image receptor response function. However, the screen-film image can display only approximately 30 shades of gray on a viewbox. That is why radiographic technique is so critical in screenfilm imaging. CR imaging is characterized by extremely wide latitude. Four decades of radiation exposure results in 10,000 gray levels, each of which can be evaluated visually by postprocessing. Proper radiographic technique and exposure are essential for screen-film radiography. Overexposure and underexposure result in unacceptable images. With CR, radiographic technique is not so critical because contrast does not change over four decades of radiation exposure. At this time, it should be emphasized that the conventional approach that “kVp controls contrast” and “mAs controls OD” does not hold for CR. Because CR image contrast is constant, regardless of radiation exposure, images can be made at higher kVp and lower mAs, resulting in additional reduction in patient radiation dose. The transition from screen-film radiography to CR brings several significant changes. Fewer repeat examinations should be needed because of the wide exposure latitude. Contrast resolution will be improved and patient dose may be reduced CR should be performed at lower techniques than screen-film radiography