Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
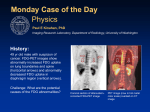
Radiological Category: Thoracic/Nuclear Principal Modality (1): CT with FDG PET overlay Principal Modality (2): CT with and without IV contrast Case Report Submitted by: Matthew Bean MSIV Faculty reviewer: Sandra Oldham M.D Date accepted: August 28, 2014 Case History 64 year old male smoker from Mexico who presents with weight loss and hemoptysis. He had a CT done at a hospital in Mexico which showed a lung mass. Decided to come here instead of being worked up and treated in Mexico. Radiological Presentations CT with IV contrast from hospital in mexico. CT w/FDG PET overlay coronal views taken here. Radiological Presentations Findings and Differentials Findings OSH CT: Right sided, central lung mass with irregular borders. Subsegmental, linear atelectasis right upper lobe. MHH CT with FDG PET overlay: Right sided, central, FDG avid mass with lobulated borders. Multiple, confluent, enlarged, FDG avid para-aortic lymph nodes. Moderate sized, right sided pleural effusion. Differentials •Lung cancer: Primary vs. Metastatic •Sarcoidosis •Infectious: Fungal granuloma, active infection, granuloma secondary to Tuberculosis Discussion: PET/CT Advantages of FDG-PET in Lymph Node Staging ● FDG-PET has the ability to identify positive nodes that are smaller than the standard CT pathologic enlargement criteria of one centimeter as well as identify larger size nodes that are negative. ● PET imaging with anatomically fused images is advantageous in being able to identify the exact location of mediastinal nodes near the midline. Staging - Distant metastases ● One of the most important roles for FDG-PET ● Commons sites a. adrenal glands, liver, bones ● Stage IV - palliative chemotherapy is indicated. ● Direct biopsy site to confirm the highest stage of disease expediting the work up ● FDG-PET scan can reveal a distant site of disease that can be biopsied. This often can obviate the need to biopsy the primary lesion. ● Biopsy based on an FDG-PET scan can make the diagnostic workup more effective. Discussion: PET/CT Sensitivity and Specificity ● FDG-PET is very sensitive though not very specific ● Sensitivity of 96.8 and specificity of 77.8 in accuracy to differentiate malignant and benign lesions3. Negative FDG-PET significantly reduces the chance that a lesion is malignant ● This decreases with smaller lesions in the 5-7 mm range, continue follow up ● May be adequate to obviate further clinical work up or continue non-invasive follow up ● FDG avidity of bronchiolo-aveolar cell cancer is reduced Sources of false positive FDG avid foci ● Granulomatous disease is a common cause of false positive single pulmonary nodule. ● Fungal granulomas due to coccidiomycosis, histoplasmosis, and aspergillosis. ● Granulomas due to tuberculosis. ● Sarcoidosis often has a characteristic pattern, but it can cause false positives. ● Active infections ● Post infectious nodules Radiological Presentations 49 year old man with weight loss, chronic cough, recurrent low grade fever. Radiological Presentations 52 year old man with 3 months of cough. Discussion: Infectious (L)Nocardia infection- Nodules/masses with irregular borders, FDG avid on PET, mimicking malignancy on imaging. Abscess formation and cavitation is common. Can also have associated pleural effusion and thickening. (R)Biopsy proven, cryptogenic organizing pneumonia. Both were suspected to be cancer until biopsy showed otherwise. Authors: P. Diana, S. L. Betancourt; Houston, TX/US Radiological Presentations 50 year old female with cough and cutaneous lesions of the shins. Radiological Presentations Same condition, different patient radiographic presentations. Discussion: Sarcoidosis Can have a variety of imaging presentation patterns in the chest/lungs like bilateral hilar lymphadenopathy, diffuse lymphadenopathy, reticulonodular infiltrative pattern, alveolar ground glass or dense nodular opacities, and bullae and cyst formation. Tissue diagnosis is imperative. Shetty A, Carter JD. Sarcoidosis mimicking lymphoma on FDGPET imaging. Radiology Case Reports. (Online) 2011;6:409. Radiological Presentations CT w/FDG PET overlay coronal views Diagnosis Biopsy showed squamous cell carcinoma. Discussion: Neoplasms Bronchogenic squamous carcinoma- Centrally located lung cancer secondary to smoking, typically not calcified, can have area of central necrosis. At presentation, 25% of patients have spread to regional lymph nodes, 55% have distant metastasis. PET/CT used widely for staging purposes. Radiological Presentations Another complication of smoking, same patient. References Johnson DH, Blot WJ, Carbone DP, et al. Cancer of the lung: non-small cell lung cancer and small cell lung cancer. In: Abeloff MD, Armitage JO, Niederhuber JE, et al., eds. Abeloff’s Clinical Oncology. 4th ed. Philadelphia, Pa: Elsevier Churchill Livingstone; 2008:chap 76. National Cancer Institute: PDQ Non-Small Cell Lung Cancer Treatment. Bethesda, MD: National Cancer Institute. Date last modified 08/08/2013. Available at:http://cancer.gov/cancertopics/pdq/treatment/non-small-cell-lung/Patient. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Non-small cell lung cancer. Version 2.2013. Available at http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. =http://www.med.harvard.edu/jpnm/chetan/lungca/clinical_scroll.html Herring, William, Learning Radiology: Recognizing the Basics Images: Shetty A, Carter JD. Sarcoidosis mimicking lymphoma on FDG-PET imaging. Radiology Case Reports. (Online) 2011;6:409. jjco.oxfordjournals.org radiopaedia.org http://posterng.netkey.at/esr/viewing/index.php?module=viewing_poster&task=viewsection&pi=116860&ti=383079&searchkey= Radiological Presentations Radiological Presentations Discussion: Neoplasms Metastatic disease- many peripheral, rounded nodules of varying sizes scatter through both lungs. Most common sources of lung metastatic disease are breast, colorectal, renal cell, and head/neck squamous carcinomas, and uterine leiomyosarcoma.