Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
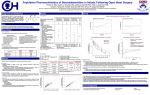
ANTIARRÍTMICOS -Sebastián Cárdenas V -Jaime Mella R.. DEFINICION TRATAMIENTO FRECUENCIA Extracelular Intracelular Na+ Ca2+ K+ Cl- +20 mV Ca2+ K+ Na+ K+ Na+ -90 mV Tiempo ECG R T P Q S ESTRATEGIA -50 mV -65 mV -75 mV Pot. Umbral -85 mV Pot. Diastólico máx. Clasificación de los Fármacos Antiarrítmicos Grupo I Grupo II Grupo III Grupo IV QUINIDINA -ADME -CONC. TERAPÉUTICAS Y TÓXICAS -CINCONISMO -RIESGO DE MUERTE. -CATEGORÍA C TRATAMIENTO A) EMESIS - Not recommended because of the risk of significant dysrhythmias, seizures, and coma. B) ACTIVATED CHARCOAL: Administer charcoal as a slurry (240 mL water/30 g charcoal). Usual dose: 25 to 100 g in adults/adolescents, 25 to 50 g in children (1 to 12 years), and 1 g/kg in infants less than 1 year old. C) GASTRIC LAVAGE: Consider after ingestion of a potentially life-threatening amount of poison if it can be performed soon after ingestion (generally within 1 hour). Protect airway by placement in Trendelenburg and left lateral decubitus position or by endotracheal intubation. Control any seizures first. CONTRAINDICATIONS: Loss of airway protective reflexes or decreased level of consciousness in unintubated patients; following ingestion of corrosives; hydrocarbons (high aspiration potential); patients at risk of hemorrhage or gastrointestinal perforation; and trivial or non-toxic ingestion. D) Monitor plasma and serum potassium levels. If refractory dysrhythmia develops, assess Ca and Mg. E) Administration of SODIUM BICARBONATE (1 to 2 mEq/kg IV in an adult, or 1/2 to 1 mEq/kg in a child) may decrease toxicity. F) TORSADES DE POINTES: Hemodynamically unstable patients require electrical cardioversion. Treat stable patients with magnesium, isoproterenol, and/or atrial overdrive pacing. Correct electrolyte abnormalities (hypomagnesemia, hypokalemia, hypocalcemia). 1) MAGNESIUM SULFATE/DOSE: ADULTS: 2 g IV over 1 to 2 min, repeat 2 g bolus and begin infusion of 0.5 to 1 g/hr if dysrhythmias recur. CHILDREN: 25 to 50 mg/kg diluted to 10 mg/mL; infuse IV over 5 to 15 min. 2) ISOPROTERENOL/DOSE: Correct hypovolemia first. ADULT: 2 to 10 mcg/minute (CHILD: 0.1 to 1 mcg/kg/minute) IV infusion; titrate to heart rate and rhythm response. Mix 1 mg isoproterenol HCl in 500 mL D5W for a 2 mcg/mL solution. 3) Avoid class Ia (quinidine, disopyramide, procainamide, aprindine) and most class III antidysrhythmics (N-acetylprocainamide, sotalol). G) PHENYTOIN OR LIDOCAINE (type I antiarrhythmics) may be used to control some types of dysrhythmias. Phenytoin theoretically is preferred as it increases AV conduction velocity. DO NOT use procainamide or disopyramide. 1) LIDOCAINE: ADULT: LOADING DOSE: 1 to 1.5 mg/kg IV push; for refractory VT/VF may give an additional bolus of 0.5 to 0.75 mg/kg over 3 to 5 min. Do not exceed 3 mg/kg or 200 to 300 mg over one hour. INFUSION: Once circulation restored begin infusion of 1 to 4 mg/min. PEDIATRIC: LOADING DOSE: 1 mg/kg; INFUSION: 20 to 50 mcg/kg/min. Monitor ECG continuously. H) Initial treatment of bradycardia or heart block should include the use of atropine and isoproterenol. 1) Consider temporary pacemaker insertion in patients with refractory bradycardia, Mobitz II block, or third degree heart block. I) 1) HYPOTENSION - Theoretically, pure or predominant alpha agonists such as norepinephrine or metaraminol may be more effective. HYPOTENSION: Infuse 10 to 20 mL/kg isotonic fluid. If hypotension persists, administer dopamine (5 to 20 mcg/kg/min) or norepinephrine (ADULT: begin infusion at 0.5 to 1 mcg/min; CHILD: begin infusion at 0.1 mcg/kg/min); titrate to desired response. J) SEIZURES: Administer a benzodiazepine IV; DIAZEPAM (ADULT: 5 to 10 mg, repeat every 10 to 15 min as needed. CHILD: 0.2 to 0.5 mg/kg, repeat every 5 min as needed) or LORAZEPAM (ADULT: 2 to 4 mg; CHILD: 0.05 to 0.1 mg/kg). • 1) Consider phenobarbital if seizures recur after diazepam 30 mg (adults) or 10 mg (children > 5 years). • 2) Monitor for hypotension, dysrhythmias, respiratory depression, and need for endotracheal intubation. Evaluate for hypoglycemia, electrolyte disturbances, hypoxia. LIDOCAÍNA CH3 CH3 O N NH CH3 CH3 TRATAMIENTO A) EMESIS - Contraindicated after oral overdose due to rapid development of seizures. B) Ingestion of most of these liquid formulations results in rapid absorption and gastric decontamination is of limited utility. C) ACTIVATED CHARCOAL: Administer charcoal as a slurry (240 mL water/30 g charcoal). Usual dose: 25 to 100 g in adults/adolescents, 25 to 50 g in children (1 to 12 years), and 1 g/kg in infants less than 1 year old. D) SEIZURES - Administer diazepam IV bolus (DOSE: ADULT: 5 to 10 mg initially which may be repeated every 15 minutes PRN up to 30 mg. CHILD: 0.25 to 0.4 mg/kg dose up to 10 mg/dose) or lorazepam IV bolus (DOSE: ADULT: 4 to 8 mg; CHILD: 0.05 to 0.1 mg/kg). 1) If seizures are uncontrollable or recur, give phenobarbital. 2) Phenytoin may worsen or precipitate cardiac arrhythmias from local anesthetics and should be avoided. E) COMA/RESPIRATION DEPRESSION - Protect the airway with an endotracheal tube and assist ventilation as necessary. F) BRADYCARDIA/BRADYARRHYTHMIAS - If symptomatic and heart rate is less than 60, consider administration of atropine 15 mcg/kg (up to 0.4 to 0.6 mg/dose) IV, IM or subcutaneously. G) HYPOTENSION: Infuse 10 to 20 mL/kg isotonic fluid. If hypotension persists, administer dopamine (5 to 20 mcg/kg/min) or norepinephrine (ADULT: begin infusion at 0.5 to 1 mcg/min; CHILD: begin infusion at 0.1 mcg/kg/min); titrate to desired response. H) ACIDOSIS - Severe metabolic acidosis (pH <7.1) should be corrected with IV sodium bicarbonate. Respiratory acidosis should be treated by assisted ventilation. Monitor serum bicarbonate and arterial blood gases to guide therapy. I) METHEMOGLOBINEMIA: Administer 1 to 2 mg/kg of 1% methylene blue slowly IV in symptomatic patients. Additional doses may be required. J) ELIMINATION ENHANCEMENT - Hemodialysis, exchange transfusion, AV hemofiltration and forced diuresis have not been shown to increase clearance substantially. Urinary acidification is NOT recommended. PROPAFENONA O OH O NH CH3 TRATAMIENTO A) In overdose ventricular dysrhythmias and seizures have been reported. Patients should be monitored for ventricular tachydysrhythmias and provided with supportive care. No specific antidote exists. B) EMESIS: Ipecac-induced emesis is not recommended because of the potential for seizures. C) GASTRIC LAVAGE: Consider after ingestion of a potentially life-threatening amount of poison if it can be performed soon after ingestion (generally within 1 hour). Protect airway by placement in Trendelenburg and left lateral decubitus position or by endotracheal intubation. Control any seizures first. 1) CONTRAINDICATIONS: Loss of airway protective reflexes or decreased level of consciousness in unintubated patients; following ingestion of corrosives; hydrocarbons (high aspiration potential); patients at risk of hemorrhage or gastrointestinal perforation; and trivial or non-toxic ingestion. D) ACTIVATED CHARCOAL: Administer charcoal as a slurry (240 mL water/30 g charcoal). Usual dose: 25 to 100 g in adults/adolescents, 25 to 50 g in children (1 to 12 years), and 1 g/kg in infants less than 1 year old. E) VENTRICULAR DYSRHYTHMIAS - Institute continuous cardiac monitoring, obtain an ECG, and administer oxygen. Evaluate for hypoxia, acidosis, and electrolyte disorders. Intravenous bicarbonate may be useful in patients with QRS widening or ventricular dsyrhythmias. Administer 1 to 2 mEq/kg bolus and repeat as needed. Monitor ECG and arterial blood gases; maintain pH 7.45 to 7.55. 1) If unresponsive to bicarbonate, lidocaine is generally the first line agent. Consider bretylium and/or phenytoin if dysrhythmias persist. F) HYPOTENSION: Infuse 10 to 20 mL/kg isotonic fluid. If hypotension persists, administer dopamine (5 to 20 mcg/kg/min) or norepinephrine (ADULT: begin infusion at 0.5 to 1 mcg/min; CHILD: begin infusion at 0.1 mcg/kg/min); titrate to desired response. G) SEIZURES - Administer a benzodiazepine IV; DIAZEPAM (ADULT: 5 to 10 mg, repeat every 10 to 15 minutes as needed. CHILD: 0.2 to 0.5 mg/kg, repeat every 5 minutes as needed) or LORAZEPAM (ADULT: 4 to 8 mg; CHILD: 0.05 to 0.1 mg/kg). 1) Consider phenobarbital if seizures are uncontrollable or recur after diazepam 30 mg (adults) or 10 mg (children > 5 years). 2) Monitor for hypotension, dysrhythmias, respiratory depression and the need for endotracheal intubation. 3) Evaluate for hypoglycemia, electrolyte disturbances, and hypoxia. 4) Phenytoin is generally NOT recommended as it may exacerbate cardiotoxicity. H) ATROPINE: ADULT DOSE: BRADYCARDIA: 0.5 to 1 mg IV every 5 min. ASYSTOLE: 1 mg IV every 5 min. Maximum total dose 3 mg or 0.04 mg/kg. Minimum single dose 0.5 mg. PEDIATRIC DOSE: 0.02 mg/kg IV repeat every 5 min, minimum single dose 0.1 mg; maximum single dose child 0.5 mg, adolescent 1 mg; maximum total dose 1 mg child, 2 mg adolescent. AHORA CONTINÚA CÁRDENAS... ANTIARRÍTMICOS CLASE II AMIODARONA LD50=254mg/kg ratones i.p., LD50=885mg/kg ratas i.p. BDoral=29-100%, Vd=65.8L/kg, t1/2=9-44días SOTALOL SOTALOL • Torsades de pointes • Prolongado intervalo QT • Fibrilación ventricular • Asístole ventricular ANTIARRÍTMICOS CLASE III PROPRANOLOL RECEPTORES BETA β1 β2 β3 TOXICOLOGÍA GENERAL • • • • • Liposolubilidad Actividad estabilizante de membrana Actividad simpaticomimética intrínseca Metabolismo Cardioselectividad ANTIARRÍTMICOS CLASE IV ANTIARRÍTMICOS CLASE IV Verapamilo TOXICOLOGÍA GENERAL • • • • Efectos cardiovasculares Efectos respiratorios Efectos sobre SNC Otros Fármacos Exposición letal mínima(g) Amiodarona Propranolol Exposición máxima tolerada(g) 8 2.06-9.6 Atenolol 2-3 1-1.8 Metoprolol 7.5-10 4.84 Verapamilo 4.16 16 EMBARAZO Droga Categoría Amiodarona C Propanolol C Atenolol D Metoprolol C Verapamilo C TRATAMIENTO • Apoyo cardiorespiratorio de funciones afectadas • Tratamiento sintomático • Monitoreo: electrolitos, función renal, glicemia, presión arterial, ECG. • Ingestión oral: lavado gástrico, carbón activado. CONCLUSIÓN PEROGRULLESCA TODOS LOS ANTIARRÍTMICOS PRODUCEN ARRITMIAS RESUMEN BIBLIOGRÁFICO Clin Pharmacol Ther 1976b; 18:30-36. § 93. Ueda CT, Williamson BJ, & Dzindzio BS: Absolute quinidine bioavailability. Clin Pharmacol Ther 1976a; 20:260-263. § 94. Ueda CT: Quinidine In: Evans WE, Schentag JJ & Jusko WJ (eds): Applied Pharmacokinetics, 2nd ed, Applied Therapeutics, Inc, Spokane, WA, 1986, pp 712-734. § 95. Vale JA, Krenzelok EP, & Barceloux GD: Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. J Toxicol Clin Toxicol 1999; 37:731-751. § 96. Vale JA: Position Statement: gastric lavage. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol 1997; 35:711-719. § 97. Valman HB & White DC: Stellate block for quinine blindness in a child. Br Med J 1977; 1:1065. § 98. Vollmer F, Brembilla-Perrot B, & Thiel B: Tachycardies ventriculaires polymorphes survenant trois mois apres une ablation par radiofrequence du faisceau de his. Ann Cardio Angeiol 1998; 47:109-112. § 99. Vozeh S, Uematsu T, & Guentert TW: Kinetics and electrocardiographic changes after oral 3-OH-quinidine in healthy subjects. Clin Pharmacol Ther 1985; 37:575-581. § 100.Wang L, Sheldon RS, & Mitchell B: Amiloride-quinidine interaction: adverse outcomes. Clin Pharmacol Ther 1994; 56:659-667. § 101.Wasserman F, Brodsky L, & Dick MM: Successful treatment of quinidine and procainamide intoxication. Report of three cases. N Engl J Med 1958; 259:797-802. § 102.West SG, McMahon M, & Portanova JP: Quinidine-induced lupus erythematosis. Ann Intern Med 1984; 100:840-842. 103.Woie L & Oyri A: Quinidine intoxication treated with hemodialysis. Acta Med Scand “La realidad tiene limites; la estupidez no”. Napoleón