Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
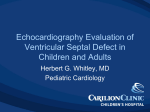
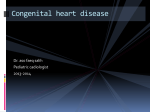
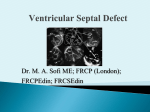
Surgically-Based Device VSD Closure Olaf Wendler Department of Cardiothoracic Surgery King‘s College Hospital NO CONFLICT OF INTEREST TO DECLARE Background Conventional Surgical Treatment Early clinical outcome after surgical repair of acute ischemic VSD is poor (mortality 30-50%) - Cardiogenic shock - Recurrent VSD - Complications from prolonged ITU 1. Jeppsson A et al. Eur J Cardio-thorac Surg. 2005 2. David TE et al. J Thorac Cardiovasc Surg 1995 Interventional VSD-Closure Interventional VSD-Closure • Device closure is established as an option for VSD closure in paediatric patients • Case series of ischaemic VSD’s reported N=18, 5 pts with acute iVSD, early survival 40% Hypothesis Hypothesis for Pilot Trial • Direct surgical closure of an acute iVSD using an Amplatzer® muscular VSD device to • Reduce cardiac trauma – Avoid left ventriculotomy – Reduce CPB time – Avoid cardiac arrest • Achieve full revascularisation • Reduce incidence of recurrent VSD • Simplify device deployment (Ethically approved by the King’s Novel Procedures Committee) Case Report A novel surgical approach to close an acute ventricular septal defect using an occluder device Chanaka Rajakaruna (MRCS), Jonathan Hill (MA, MRCP), Eleanor Jane Holland Turner (BSc, PhD, MRCS), Alex Sirker (MRCP), Bushra S Rana (MRCP), Olaf Wendler (MD, PhD, FRCS) Departments of Cardiothoracic Surgery and Cardiology, Kings College Hospital, London. UK. Case Report Patient Data • 75 y, male • no past medical History • Presentation – Anterior MI – iVSD 4 d pMI – Pulmonary oedema – Cardiogenic shock Case Report ECHO • Anterior VSD (7-9 mm) • L to R shunt (Qp:Qs = 4:1) • LVEF 45% • RV preserved • PAP 50 mmHg Case Report Preoperative Treatment • Insertion of IABP • Coronary angiography – LAD 95%, D1 75% – Cx normal – RCA occluded, Crux 70% • Scheduled for surgery when he deteriorated 10 pMI (24. 03. 2006). Case Report Operation (I) • Midline sternotomy & aorto-bicaval cannulation • On-pump beating heart – Sequential LIMA to LAD & D1 – Sequential SVG to LV branch & PDA • Epicardial 3-D-ECHO – VSD of 18-21 mm in the mid septum Case Report Operation (II) • VF induced • Incision (1.5cm) in the anterior wall of the RV • VSD size 20mm, Device 24mm • Device deployed, direct vision • RV closed after de-airing • The patient weaned off CPB with IABP and Noradrenaline (0.09mcg/kg/hr) Case Report Postoperative Course • • • • • Early extubation (6 hours pOP) IABP for 48 hours Furosemide infusion (5-10mg/hr) Adrenaline and Noradrenaline (0.05- 0.1mcg/kg/hr) Complications – Chest infection – Haemothorax secondary to chest drain (day 20) • Discharged on day 32 Case Report 6 - Months Follow-Up • Asymptomatic • NYHA I • ECHO - Device well seated - Residual shunt through device (Qp:Qs=2:1) • PAP 20 mmHg Summary Summary Potential advantages vs. Conventional surgery - No incision in the LV - Reduced CPB time - No cardiac arrest Interventional treatment - Device deployed under direct vision - Complete revascularization Conclusion Conclusion Limitation - Residual shunt through the device Outlook - Earlier intervention may improve outcome - Improve surgical technique - Modification of the device