Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
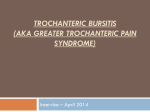
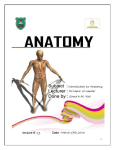
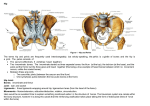
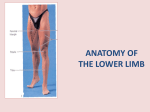
GLUTEAL FUNCTION, TRAINING AND HIP MECHANICS Ed Harper MSc, BSc, ASCC Session Aims: • Define Gluteal function and relate to hip mechanics and general movement patterns. • Compare methods of Gluteal Assessment. • Evaluate proposed ‘3 Stage’ Training progressions. • Myths and Misconceptions – Squatting Where to start • Bipedal Locomotion only in humans! • 4 Considerations: • Stability in upright posture • Ability to raise & control trunk over hind limbs • Ability to balance on one leg • Walk with feet underneath body The most misunderstood, undertrained and important muscle in the body! • In order to enhance performance we need to understand what underpins movement. • The muscles of the gluteal region are primarily responsible for extension, abduction, lateral rotation and slight medial rotation of the hip joint. Gluteal Function • Therefore walking, running, jumping, standing, throwing, sitting in every direction! Gluteal Strength: • Encourages good lifting/movement mechanics and less lumbar rounding. This also spares the knee joint by allowing the hips to share the load when lifting rather than overloading the knees. • Stabilises the knee preventing valgus which decreases the likelihood of patellofemoral pain and ACL tears. • Enhances overall structural health, reducing the risk of postural weakness (e.g. lower- and upper-cross syndrome, groin/hamstring/quad strains, shoulder issues, spinal issues, Sciatica, and hip pain). Injury Prevention Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA (2000) ’Hip abductor weakness in distance runners with iliotibial band syndrome’ Clin J Sport Med Jul;10(3):16975. Robert Griffin III • Washington Redskins officially signed him to a four-year, $21.1 million contract with a $13.8 million signing bonus in 2012. • 2012 ACL tear. Gluteal Region Obturator Internus ORIGIN Inner surface of obturator membrane and rim of pubis and ischium bordering membrane INSERTION Middle part of medial aspect of greater trochanter of femur ACTION laterally rotates and stabilizes hip NERVE Nerve to obturator internus (L5, S1,2) Gemellus Superior ORIGIN Spine of ischium INSERTION Middle part of medial aspect of greater trochanter of femur ACTION laterally rotates and stabilizes hip NERVE Nerve to obturator internus (L5, S1, 2) Gemellus Inferior ORIGIN Upper border of ischial tuberosity INSERTION Middle part of medial aspect of greater trochanter of femur ACTION laterally rotates and stabilizes hip NERVE Nerve to quadratus femoris (L4, 5, S1) Sacrotuberous Ligament Sacrospinous Ligament Piriformis ORIGIN 2, 3, 4 costotransverse bars of anterior sacrum, few fibers from superior border of greater sciatic notch INSERTION Anterior part of medial aspect of greater trochanter of femur ACTION laterally rotates and stabilizes hip NERVE Anterior primary rami of S1, 2 Gluteus Minimus ORIGIN Outer surface of ilium between middle and inferior gluteal lines INSERTION Anterior surface of greater trochanter of femur ACTION Abducts and medially rotates hip. Tilts pelvis on walking. NERVE Superior gluteal nerve (L4, 5, S1) Gluteus Medius ORIGIN Outer surface of ilium between posterior and middle gluteal lines INSERTION Posterolateral surface of greater trocanter of femur ACTION Abducts and medially rotates hip. Tilts pelvis on walking NERVE Superior gluteal nerve (L4,5,S1) Quadratus Femoris ORIGIN Lateral border of ischial tuberosity INSERTION Quadrate tubercle of femur and a vertical line below this to the level of lesser trocanter ACTION laterally rotates and stabilizes hip NERVE Nerve to quadratus femoris (and obturator internus) (L4, 5, S1) Gluteus Maximus ORIGIN Outer surface of illium, sacrum, coccyx, sarotuberous ligamens INSERTION Illiotibial tract, gluteal tuberosity of femur ACTION Extends and laterally rotates thigh at hip, through illiotibial tract extends knee NERVE Inferior gluteal nerve Tensor Fascia Lata ORIGIN Outer surface of anterior iliac crest between tubercle of the iliac crest and anterior superior iliac spine INSERTION Iliotibial tract (anterior surface of lateral condyle of tibia) ACTION Maintains knee extended (assists gluteus maximus) and abducts hip NERVE Superior gluteal nerve (L4, 5, S1) Sciatic Nerve Whole Picture Glute (Max) Squeeze - The vast majority of glute fibers insert into fascia, with only a small percentage insert onto the gluteal tuberosity of the femur. Research suggests 70-85% but it might be even higher. Largest muscle of the 21 hip muslce’s, accounting for approx. 16% of total cross-sectional area of musculature. Gluteal Assessment • Bilateral – Squat (Bench, OH, BW) • Unilateral – Trendelenburg Test/Hurdle Step • Timing • Activation • Load? • Hermes Scratching the surface Exercise Hierarchy Level 1 •Position of high stability – Stimulus – Position of high stability. •Maintain torque and maximum stability throughout. •Squat, Deadlift, Bench Press. Level 2 •Position of high stability – Complex element – Position of high stability. •Start and finish in same position with implementation of speed. •CMJ, Running, Snatch Balance. Level 3 •Position of transition – Speed/Complex element – Position of high stability •Actions resembling sport/movement, starting and finishing in different positions. •Snatch, Clean, Jerk, Sport Specific Individual Exercise Progression Client Test Level 1 Level 2 Level 3 Rugby Player – Bilateral Max Strength OH Squat, Hurdle Step/SL Squat Rack Pull/American Deadlift Dead Pull Clean Middle Age Man – ACL Rehab OH Squat, Hurdle Step/SL Squat Paloff Press BW Bench Squat BW MB Jump Squat Netball Player – Unilateral Power OH Squat, Hurdle Step/SL Squat Lunge SL Linear Hurdles SL Box Jump* *Q Angle Brett Contreras - Research Myths and Misconceptions - Squatting +++ • Form of Assessment. • Strong correlation to sport/movement. • Fairly easy to teach/learn and progress. • Good for teaching lumbo-pelvic hip complex mechanics. -----• Little focus on fine detail – Crossfit, Insanity, 30 day squat Challenge. • Easy(ish) to hide poor form. Foot Position • Externally rotated feet (for comfort, support or to selectively strengthen individual muscles – quadriceps) is not supported by research (Boyden 2000; Signorile 1995). • Rotation greater than ~20° may increase mobility but reduces gluteal activation. Also commonly causing dropped arches and collapsed ankles. • Inadequate gluteal/hip strength, in addition to overactive hip adductors, prevents proper stabilization of the femur. Forcing the hips to move into adduction and internal rotation. Reducing Gluteal (+ext. Rotator) activity = knee valgus. Mobility Narrow Vs Wide Don’t make excuses for form or depth! Hyperextension Addressing hyperextension shortens hamstrings. (lumbar flexion/posterior pelvic tilt) When you descend into a squat, the hamstrings are being lengthened at the pelvis, but shortened at the knee. So it would seem to me that the net length change is • negligible Femur – Pelvis = Hip ‘pinching’ • Cause? Joint Mobility, Muscle Flexibility, Motor Control/Stability? • Tight anterior hip musculature 9-5ers - Corrective exercises: • ½ Kneeling Stretch/Bucket Stretch (*Hip + Shoulder) • Raised Lunge • Extended horiz./vert. Squat (+ regressions/progressions) • Start as you mean to go on • Hamstring length commonly Research suggested limited ankle dorsiflexion alters squat mechanics (Macrum et al. blamed when... 2012). Tight ankles during a squat will push the body into a backwards weight shift. Leading to either falling backwards, or dropping the chest and rounding the back as a counterbalance. Conclusions • Every case is individual • Vital to include some form of gluteal activation, strengthening and hip mobilisation. • ‘Go to’ Exercises – • Pre-hab/Activation always in warm up • Clams, Bi and Unilateral Squats and Bridges, Linear and Lat Lunges • Main Focus • Hip Thrust/Bridge, SL Thrust/Bridge, Squat, Deadlift, S.S./Lunge • Additional/Assitive • Pallof, DB Bench etc References Holmes et al. (1992). Erector spinae activation and movement dynamics about the lumbar spine in lordotic and kyphotic squat-lifting. Spine.Vol 17 (3). McKean et al. (2010). The lumbar and sacrum movement pattern during the back squat exercise. The Journal of Strength and Conditioning Research. Vol 24 (10). Walsh et al. (2007). Three-dimensional motion analysis of the lumbar spine during “free squat” weight lift training. The American Journal of Sports Medicine. Macrum et al. (2012). Effect of limiting ankle-dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. J Sport Rehabil. 21 (2):144-50. Presswood L, Cronin J, Keogh J, Whatman C (2008). Gluteus Medius: Applied Anatomy, Dysfunction, Assessment, and Progressive Strengthening. Strength and Conditioning Journal, 30 (5), 41-53 http://bretcontreras.com/