Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Human microbiota wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
West Nile fever wikipedia , lookup
Urinary tract infection wikipedia , lookup
Anaerobic infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Hepatitis C wikipedia , lookup
Hepatitis B wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Neonatal infection wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
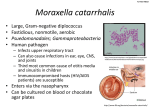
Branhamella catarrhalis Made by :Huda M. N. Hanyia Presented to:Dr Abdelraouf A. Elmanama Introduction Branhamella catarrhalis is classified with genera Neisseria, Moraxella and Acinetobacter in the family Neisseria. The taxonomic position of B. catarrhalis be assigned to the genus Moraxella (M. catarrhalis) in the family Moraxella, or to its own genus Moraxellae are closely related to the Neisseriae. Like Neisseriae, they synthesize the unusual type 4 pili that are involved in both adherence and motility. Some of the other organisms that synthesize type 4 pili also synthesize a variety of hydrolytic enzymes that may be involved in pathogenesis, but these have yet to be identified in Moraxella. In the clinical laboratory , isolates of B . Catarrhalis must be distinguished from Neisseria The Branhamella catarrhalis was consider as a saprophyte of the upper respiratory tarct with no siginficant pathogenic. Although the commensal status of Branhamella catarrhalis in the nasopharynx is still accepected , the organism is common cause of Otitis media and sinusitis , laryngitis. The Branhamella catarrhalis Bacteremia especially in patients who are immunocompromised. Bacteremia can be complicated by local infection such as osteomyelitis or septic arthritis. Branhamella catarrhalis is also associated with nosocomial infections. Normal human habitat: It is a part of the normal in human cavity and mucosa and nasopharynx Sources/specimens: nasopharyngeal specimen, blood, cerebrospinal fluid Reservoir : human Zoonosis: none vector: none Mode of Transmission: By direct contact with droplets and discharges from nose and throat of infected persons ; nosocomial transmission is being increasingly documented 1. 2. 3. o o Lab studies: CBC count : increased WBC count with netrophilia may be present in branhallema catarrhalis. Gram stain: Gram-negative diplococcus culture result are found ;strict adherence to the staining is required Confirmation of diagnosis of branhallema catarrhalis is based on isolation of the organism in culture. culture can be taken from middle ear effusion, the nasopharynx, sputum, blood ,wound, urine . colonies are 0.2 cm in diameter, opaque, and no hemolytic after incubation on C.A,or B.A for 48hrs characteristically , colonies can be pushed along the surface of the agar like hockey puck with standard methods of identification , branhallema catarrhalis can be difference from Neisseria species by not using sucrose ,glucose. Because Neisseria cineria has the same reaction pattern, the superoxol test must be added. for definitive identification Dnase and nitrate reduction are performed ; branhallema catarrhalis Dnase and nitrate and nitrite levels several rapid confirmy tests are available to identify branhallema catarrhalis , and they are all based on the ability of branhallema catarrhalis to hydrolyze tributyrin. This provides immediate identification and separation from human Neisseria species Neisseria species, which do not hydrolyze tributyrin serological tes for branhallema catarrhalis are not widely used : cross-reactively with Neisseria species in the detection of complent fixation Ab by immunoelectrophoresis has been demonstrated. 1. Serum Ab to whole cell protein, to lipooligosaccharides, and to outer membrane Ag have proved useful in the diagnosis of branhallema catarrhalis infection. Other lab studies may be needed , depending on the site of the infection and underlying condition Imaging studies: Imaging studies may be needed, depending of the site of infection: Paranasal sinus radiographs or CT scans. 2- chest radiographs 3- abdominal radiographs: obtain a 3-way peritonitis is a possibility. Pathogenicity; Infection in adult: A-The M. catarrhalis is manifest itself as a pathogen in the nosocomial setting .a rare but very serous and frequently lethal infection with M. catarrhalis appear to be endocarditic B- laryngitis C- bronchitis and pneumonia 1. Infection in the children: 1. Meningitis Media Otitis Pneumonia Bronchitis Bacteremia complication: recurrence, Bacteremia, meningitis, mastoidotis, hearing loss, pleural effusion, shock, death 2. 3. 4. 5. Nosocomial infection: outbreaks of infection with branhallema catarrhalis have reported, mostly involving pulmonary units or pediatric intensive care units. Increased length of hospitalized has been correlated with the presence of branhallema catarrhalis Bacteremia : no primary site infection was found in 46% of patient with branhallema catarrhalis bacterima . Deterrence/prevention: universal precaution, good hand hashing and sterilization of instruments and tubes used intubations , aspiration, or invasive produced may reduce or prevent the nosocomial infection caused by branhallema catarrhalis prognosis :prognosis is poor for hospitalized patients with underlying conditions, especially the following; Patients hospitalized for prolonged periods 1. 2- Patients in pulmonary units or pediatric intensive care units 3- Patients of advanced age. Patients education: Hand washing, smoking cessation, and good heath habits (e.g, proper rest, diet, exercise) are helpful both the treatment process and in prevention of any infection. Characteristic of B. catarrhalis Gram stain: Gram-negative diplococcus Colony morphology : Pigmentation: Oxidase test: Acid production Production of deoxyribonucleas(DNase): Polysaccharide from sucrose: Superoxol test (reaction with 30% hydrogen peroxide) Catalase test (reaction with 3% hydrogen peroxide); When performed on clear base medium without Hb , the Catalase reaction of B. catarrhalis may vigorously, but very rapid and then become negative , persistent bubbles may not be observed . Thus , the reaction should be watched to observe a positive Catalase reaction Colistin resistance: Nitrate reduction ; positive 1. MEDIA OF CHOICE: Modified oxidation-fermentation medium was developed as a practical medium for highly and specific detection of acid production from carbohydrates by Neisseria spp. and B catarrhalis. Neisseria spp and B. catarrhalis were tested in this medium , in which the protein concentration was reduced relative to the carbohydrate concentration , phenol red was substituted for bromthymol blue at low conc. and the PH is 7.2 . Sugar utilization patterns were consistent with published result and other cultural and biochemical characteristics for these species. The reaction obtained using this medium were qualitative better and more reproducible than those obtained in cystine- Trypticase agar . 1. 2. 3. To study effect of various commonly used media on the growth of Branhamella : New York city medium (MNYC) containing the selective agent trimethoprim lactate Modified Thayer Martin medium containing vancomycin Mac agar 4- crystal violet blood agar , bilayer ;lower contain colum blood agar, the upper blood agar contain crystal violet 5- N.A 6- semiselective media for Branhamella allow all Neisseria ssp and further differentiation is necessary. The plate incubated at 22c and 37c aerobically and 37c anaerobically on NA Cultured were read after overnight and read as light, moderate or heavy growth The result : The Branhamella have no ability to grow on MNYC or MTM media All the strain of Branhamella failed to grow on the MAC agar and blood agar All strain grow on the N.A at 22c and 37c None of the strain of Branhamella grew under the anaerobic condition because the morphological similarities and biochemical variation among Neisseria ssp.and Branhamella may cause confusion and result in error delayed in their recognition Dnase is test high specificity it can be used as confirmatory test and also superoxol test. Risk factor: 1. This bacteria cause more than 70%of patient that have neutropenia, malignancy, respiratory impairment. This bacteria cause infection in most patient older than 65 year and 90%to 95%of patient have underlying cardiopulmonary disease. A large % are smoker Men appear to be greater risk than women 2. 3. 4. Virulence of M. catarrhalis: 1. Adherence: Study M. catarrhalis was show to specifically attach to the mucin molecules from thenasopharynx and middle ear but not to mucin the saliva and trancheobronchial mucin. The interaction such as these represent the first steps in the process of bacterial colonization and infection. The presence or absence of fimbria did not influence the capacity of the bacterium to adhere or to cause haemagglutination . The bacteria and epithelial cell are both negatively charged, interaction between the negatively charged surface of M. catarrhalis cells and positively charge domain s called microplica on pharyngeal epithelial cells was found. 2- Tissue culture adherence and haemagglutination characteristics of M.catarrhalis The haemagglutination and tissue culture adherence properties of 20 isolates of Moraxella catarrhalis obtained from the sputum of elderly patient with lower respiration tract infection were compared with those 20 isolation of Moraxella obtained from the nasopharynx of elderly persons colonized by the organism . Eighty percent of isolate from the infected group as opposed to 5% of isolate from the colonized group hameagglutinin human erythrocyte . The indicating that the hameagglutinin might be a marker of Pathogenicity for catarrhalis. Animal Models: the low virulence of M .catarrhalis in laboratory animals has hampered protection experiment and Pathogenicity studies in rats and mice one study on the model was presented by lee etal, who were able to isolate live M .catarrhalis from specific mouse strain, suspended in BHIB were inoculalated via interaperitoneal route . infection resulted in high mortality and facilitated antibiotic efficacy studies. in another study murine model designed to study phagocyte response and clearance mechanism after endotarcheal challenge with M .catarrhalis , high influx of PMN leukocytes into the lung bacteria were cleared from the lung within 24-48hr, and the animal remained healthy Enhanced clearance of bacteria from the lungs was observed , correlating with higher levels of specific IgA and IgG in serum and bronchoalveolar lavage fluid the clearance of M .catarrhalis from the lungs is rapid within 6-24 h , result of low virulence of M .catarrhalis for animal models. passive and active immunization studies in this animal model documented improved pulmonary. Complement resistance: complement resistance strain appeared to activate complement to the same extent as , or even slightly. the resistance strain do not inhibit classical or alternative complement pathway activation but interfere with complement at the level of attack complex formation Treatment: Amoxicillin-clavulanate,second and third generation oral cephalosporin and trimethoprim-sulfamethoazole are the most recommended agent. Alternatively, azithromycin, diithromycin can be used . All other agents listed below are also effective :