Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
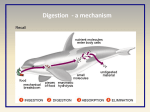
Department of faculty and hospital surgery Tashkent Medical Academy Diseases of the esophagus Diseases of the esophagus Occupies the 6th place In the structure of human diseases On the 3rd place Among diseases of gastro - intestinal tract (after disease Of stomach and rectum) The incidence rates of esophageal population in 2010 year (100 thousand) Incidence of malignant tumors In 2010 year in the Republic of Uzbekistan History of surgical treatment of esophageal-is starting with 1877., When Vincenz Cherny conducted the first successful resection of the cervical esophagus Vincenz Czerny (1842 − 1916) Franz J. A. Torek (1861-1938) Only in 1913, Franz Torek first successfully performed transtorakaling resection of the esophagus (through the left torakotomtion access) cancer middle chest Transthoracic access to the clinic tried to apply Johannes von Mikulicz (1904), Ernst Sauerbruch (1905), but these attempts were unsuccessful Johannes von Mikulicz-Radecki 1850 - 1905 Sergey Yudin (1891-1954) Peter A. Herzen (1871-1947) Ivan Greeks (1867-1934) Mikhail Davydov Vasit Vakhidovich Vahidov Shavkat Ibrahimovic Karimov Sadik Aliyevich Masumov Nikolai Fedorovich Krotov Duties of the general practitioner in diseases of the esophagus - Provision of primary health and social care; - Health education (promoting healthy lifestyles); - Preventive work (timely detection of early and latent forms of the disease, risk groups); - Dynamic monitoring; - Emergency assistance in case of emergency and acute conditions; - Timely consultation and hospitalization in the prescribed manner; - Medical and rehabilitation work in accordance with the qualifying characteristic; - An examination of temporary disability; - The organization of medical and social care and household together with the bodies of social protection and services of mercy alone, the elderly, the disabled, the chronically ill; - Maintaining the approved forms of records and reports. Anatomy of the esophagus Tracheal Aortic Bronchial Aorto-bronchial Epibronhial Retropericardial Supradiaphragmatic Intradiafragmal Abdominal Anatomical region and part of the esophagus 1. The cervical 2. Hilar department a. The upper part of the chest b. The average breast part. c. The lower part of the chest (including abdominal esophagus). Blood circulation and the lymphatic system of the esophagus branches of the lower thyroid artery bronchial artery branches of the thoracic aortic ascending branch left gastric artery Metastasis Methods of study of the esophagus 1. 2. 3. 4. 5. 6. Radiographs Endoscopic examination Radioisotope study (external and intraluminal) Ultrasound examination Intraesophageal pH-meters The study of motor Endoscopic method of investigation of the esophagus X-ray method for studying the esophagus Classification of diseases of the esophagus I. Malformations 1 Congenital esophageal atresia and esophageal-tracheal fistula 2 Congenital stenosis of the esophagus 3 Congenital diaphragm membrane of the esophagus 4 Congenital short esophagus 5 Congenital esophageal cyst 6 Anomalies vessels II. damage 1 Traumatic injuries - interior and exterior 2 Burns of the esophagus and their consequences III. diseases of the esophagus 1 diverticula - pulse and traction 2 Inflammatory diseases - esophagitis IV. Tumors of the esophagus 1 Benign tumors 2 Cancers V. Violation of esophageal motility (cardiospasm) 1 Achalasia 2 esophagism The frequency of lesions of the esophagus Cancer Sarcoma Polyps Cardiospasm Cicatricial stricture Diverticula Esophagitis Tuberculosis Syphilis 60-80 0,04 0,04 5,1 0,7 0,6 0,2 0,02 0,08 Esophageal cancer is 3.4% of all malignant neoplasms Dysphagia Grade I - pass any food, but swallowing solid food there are unpleasant sensations (burning, scratching, sometimes pain) Grade II - solid food stays in the esophagus and passes with difficulty, it is necessary to wash down solid food with water Grade III - solid food does not pass. When you try to swallow it arises regurgitation. Patients are fed liquid and semi-liquid food Grade IV - the esophagus to pass only liquid Grade V - complete obstruction of the esophagus. Patients are unable to swallow a sip of water, does not pass even the saliva Types of congenital esophageal atresia Esophageal corpus alienum Esophagealbronchial fistula Excision of the esophagealbronchial fistula Degree of burns of the esophagus Grade I - redness and swelling of the mucous membrane Grade II - the defeat of the mucosa and submucosa Grade III - the defeat of all the shells of the esophagus Factors determining the degree of damage to the esophagus a burn 1 The nature of the received material 2 Number of received material 3 Concentration of the solution 4 Consistency received substance 5 Individual sensitivity to the received substance The clinical picture of burns of the esophagus Acute stage (5-10 days), pain in the mouth, pharynx, behind Step imaginary well-being (7-30 days) as a result of Stage of formation of the stricture (from 2 to 6 months, sometimes years) on the wall of the esophagus ulcers of the breastbone, in the epigastric region. Hypersalivation. dysphagia, shock in the next few hours after the injury. Burn toxemia after a few hours begins to prevail rejection of the necrotized esophageal webs around the end of the 1st week is somewhat looser. Complications: esophageal bleeding, perforation of the wall of the esophagus, in the presence of extensive wound surfaces develops sepsis different sizes. Wound surface covered with a scab, bleed easily. Dysphagia can reach the degree of complete obstruction of the esophagus. When top strictures: laryngospasm, coughing, choking due to spillage of food into the airway Burns and scar strictures of the esophagus Short burn stricture at pharyngeoesophageal transition Short burn stricture of the middle third of the esophagus Extended burn stricture of the esophagus Burns and scar strictures of the esophagus Complications caused by chemical burns of the esophagus Early shock laryngeal edema hemolysis Older stricture depletion pulmonary Early acute tracheobronchitis pneumonia Esophageal-bronchial fistula Perforation mediastinitis pericarditis empyema bleeding Older pneumonia lung abscess bronchiectasis Esophageal-bronchial fistula Other foreign bodies diverticula Hiatal hernia Cancer of the esophagus Complications of dilatation anemia sepsis Treatment of burns of the esophagus in the acute period 1. 2. 3. 4. 5. 6. 7. 8. 9. Neutralize poison Removal of intoxication and pain Normalization of water-salt metabolism Anti-inflammatory therapy Parenteral nutrition Normalization function of the cardiovascular system Normalization of renal function Prevention of respiratory disorders Oral Care Probing of the esophagus Segmental esophagoplasty colon Esophagoplasty stomach Esophagoplasty with stomach Esophageal diverticula Esophageal diverticula Esophageal diverticula Esophageal diverticula Complications of esophageal diverticula 1 2 3 4 5 Diverticulitis - 85.2% Intestinal obstruction - 6.5% Bleeding - 4.3% Perforation or penetration - 3.2% Tumor development - 0.8% Removal of esophageal diverticulum Classification of reflux esophagitis I. Primary Primary disorders of the nervous and peptide (gastrin, histamine, motilin, etc..) Regulation of motility of the esophagus and the stomach II. Secondary When hiatal hernia, pyloric stenosis, peptic ulcer, cholecystitis, large tumors in the abdomen, ascites, pregnancy, after gastrectomy, scleroderma, and other diseases III. Severity (endoscopic classification of Savary and Miller, 1978) Stages of cardiospasm (B.V. Petrovsky) Stage I - unstable functional spasm of the cardia, the expansion of the esophagus is not observed Stage II - stable spasm of the cardia with soft extension of the esophagus Stage III - scarring the muscle layers of the cardia with a pronounced expansion of the esophagus Stage IV - pronounced stenosis of the cardia with dilation of the esophagus, often Sshaped with esophagitis Cardiospasm stage IV stage II stage III Treatment of the cardiospasm Treatment of the cardiospasm operation of Nissen Achalasia of the esophagus The most characteristic symptoms of achalasia of the esophagus 1. 2. 3. 4. 5. 6. Dysphagia After the passage of food techniques that increase the intraluminal pressure Regurgitation (a few hours after a meal the night immediately after a meal) Pain (pain crises, non-food, pain on swallowing, paresthesias, itching, etc.) Nausea, vomiting, weight loss Complications (esophagitis, the transition to cancer, respiratory disorders) A benign tumor of the esophagus Removal of a benign tumor of the esophagus Cancer of the esophagus The share of esophageal cancer: structure bowel diseases - 5-7%; in the structure of all neoplasms of the body - 1.5-2%. Mortality from cancer of the esophagus, in a number of other malignancies, up - 5-6%. Factors contributing to the development of cancer of the esophagus Alcohol and tobacco; Deficiency of vitamin A, riboflavin, zinc, molybdenum; Dietary carcinogens; Chemical burns or stricture of the esophagus; Tyloses (a disease characterized by hyperkeratosis of the palms and soles); Plummer-Vinson syndrome (iron deficiency anemia + + achlorhydria stricture of the upper esophagus; A long-term untreated achalasia; Prior exposure of the mediastinum; Celiac disease and chronic non refluks esophagitis. Cancer of the middle third of the esophagus Cancer lower third of the esophagus Growth form of esophageal cancer Symptoms of esophageal cancer General adynamy, weight loss, fatigue, low-grade fever, hypoproteinemia Characteristic of diseases of the chest cavity blunt chest pain, tachycardia after eating, changing the tone of voice, coughing Characteristic of esophageal Dysphagia - reflex, mechanical or mixed, increased salivation, pain, bad breath, bad taste, regurgitation Clinical manifestations of esophageal cancer Dysphagia; Weight loss; Odynophagia; Constant chest pain, epigastric and back; Hiccups; Hypersalivation; Hoarseness; Symptoms of damage to the nervous system and muscles; Vomiting blood. Diagnosis primary binding studies Chest X-ray in 2 projections; Polypositional contrast study of the esophagus and stomach; Esophagoscopy with multiple biopsies from both the tumor and from the mucosal sites are not altered by the expected resection line; Morphological examination of the biopsy specimen; Ultrasound imaging of the mediastinum, supraclavicular areas, abdominal, retroperitoneal, pelvic organs; ECG; bronchoscopy; General analysis of blood and urine tests, biochemical blood tests, coagulation, immunoassay, blood group and Rh factor. Diagnosis additional studies Computed tomography of the chest and abdomen with contrast; Diagnostic thoracoscopy; Diagnostic laparoscopy -with suspect the presence of metastases in the abdominal cavity. Radiographs of patients with esophageal cancer At the level of Th6 determined by restriction esophagus. Patency of barium significantly impeded. CONCLUSION: Cancer middle third of the esophagus. There is a circular narrowing of the esophagus at the level of TH7, for 3.0-3.5 cm. Above which the esophagus suprastenoticheski expanded. CONCLUSION: Cancer between the middle and lower third of the esophagus (endophytic growth). Radiographs of patients with esophageal cancer Esophagus pass all over. At the level of VTh6Th7 determined luminal narrowing, tuberosity contours. The length of the process = 7.0-8.0 cm. CONCLUSION: Cancer middle third of the esophagus. From the level of VTh V-VII, for 7.0-8.0 cm. Celebrated circular narrowing of the esophagus with irregular contours, the destruction of the mucous relief. CONCLUSION: Cancer middle third of the esophagus. The differential diagnosis Cardiospasm. Cicatricial narrowing of the esophagus. Esophageal ulcers and ulcerative esophagitis. Benign tumors of the esophagus. Esophageal varices. Diverticula of the esophagus. Compression of the esophagus from the outside tumors of the mediastinum. Scars after suffering mediastinitis. Abnormally positioned vessels in the mediastinum. Leading in the differential diagnosis of esophageal cancer is morphologically !!! Only multiple negative answer, along with watchful waiting may make relatively favorable judgment. Methods of treatment of esophageal cancer radiation Herbal Surgical Combined Complex Subtotal esophagectomy with intrapleural simultaneous plasticity with stomach by Lewis. Operation - one-step, two available. Access - wide upper midline laparotomy bypassing the navel to the left, then anterolateral thoracotomy in the IV-V intercostal space on the right. Esophagogastroanastomosis in the right pleural cavity.