Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
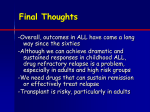
ADVANCES IN DIAGNOSIS AND MANAGEMENT OF LEUKEMIA IN CHILDREN Uma Athale MD Associate Professor, Pediatrics McMaster University, Hamilton, Canada December 28th 2015 Objectives Epidemiology of leukemia in children Evaluation of a child with suspected leukemia Recent advances in the diagnosis of acute leukemia Overview of therapeutic strategy for ALL and recent advances in therapy Objectives What is the epidemiology of childhood leukemia in Zambia? What is the outcome of children with leukemia in Zambia? How can we apply the diagnostic and therapeutic advances in Zambian context? Case # 1 BE –a 2.5 yr. old boy presented with H/O fever for 2-3 weeks Also complains of pain and has limping Has been seen by family doctor on and off Finally referred to a pediatrician Case # 1 Physical examination reveals a pale child Irritable Generalized lymphadenopathy Liver 5 cm BCM Spleen 2-3 cm BCM Case #1 What is your differential diagnosis? What is your next step? Epidemiology of Acute Leukemia ALL is the most common cancer in children Peak age 2-5 years Increased prevalence associated with industrialization and high-affluent societies Age-specific Incidence Rate of Acute leukemia Age adjusted IR per 1000,000 person-years Both AML and ALL demonstrate bimodal distribution but a different pattern Hispanic whites have the highest incidence of ALL/L and blacks the lowest AML & ALL IR higher in males T ALL M:F=2.2 whereas BALL/L 1.2 ©2012 by American Society of Hematology Graça M. Dores et al. Blood 2012;119:34-43 Graça M. Dores et al. Blood 2012;119:34-43 Is the epidemiology of childhood ALL similar in Zambia? ALL incidence is low < 1/100,00/year) esp. in children <5 yr. of age T ALL is more common with peak incidence 514 yr. ALL and AML occur in equal frequency Fleming et al. Leukemia, Letter to the Editor, 1999; 13:1292-3 Etiology of ALL Pathogenesis of ALL Prenatal origin for some childhood leukemia Detection of T-cellreceptor loci in Guthrie cards 1% newborns are shown to have TEL/AML1 (ETV6RUNX1) –leukemia specific putative clone Monozygotic twin studies Knudsen Hypothesis Pathogenesis of ALL Precise mechanism unknown <5% cases are associated with Inherited predisposing genetic syndromes Down’s syndrome Bloom’s syndrome Ataxia-telangiectasia Fannin's anemia Ionizing radiation Many possible factors High birth weight Infection-related Gene-environment interaction Delayedinfection Population mix Pui et al. Lancet 2008; 371:1030-43 Biology of ALL Clonal disease Genetic mutations in hematopoietic progenitor cells committed to T or B-cell pathways Unlimited self-renewal Stage specific developmental arrest >70% show chromosomal abnormalities Structural Chromosomal translocations TEL-AML1 Numerical: , BCR-ABL Hypodiploidy or hyperdiploidy Co-operative mutations Biology of ALL: TEL-AML1 About 25% of patients with pre-B ALL t(12;21)(p13;q22) Both TEL and AML genes important for hemopoiesis Biology of ALL Philadelphia chromosome or t(9;22) >50% T-cell ALL associated with activating mutations involving NOTCH1- gene encodes a transmembrane receptors that regulate normal T-cell development Diagnosis of ALL Sign/Symptoms Fatigue, loss of appetite, listlessness Incidental findings on blood smear Life threatening infection Life threatening hemorrhage Respiratory distress Symptoms and sign related to INFILTRATION OF ORGANS Sign/Symptoms Bone marrow involvement related WBC Fever Hemoglobin Pallor Platelet Bruises Bleeding DIC Sign/Symptoms Other organ involvements Musculoskeletal pain ( 33% ) Nocturnal pain and nonarticular pain Compression fracture of vertebrae Osteopenia and fracture CNS Headache, vomiting, lethargy, nuchal rigidity isolated cranial nerves palsy (rare) Facial nerve palsy Spinal cord compression Sign/Symptoms Genitourinary Tract Testicular mass Hematuria Gastrointestinal Tract Gingival hyperplasia GI bleeding Sign/Symptoms Respiratory Mediatsinal mass Cardiac Manifestations Pericardial effusion Sign/Symptoms Lymphadenopathy > 15 mm inguinal lymph nodes >10 mm > 5 mm for epitrochlear nodes Non tender, firm, rubbery and matted Hepatosplenomegaly Testicular involvement ~ 1-2% of boys will have testicular involvement at the time of initial presentation. Usually older boys with T cell ALL and HR disease Testicular ultrasound at relapse Other unusual presentations Multiple skeletal manifestations Osteoporosis Osetolytic lesions Moth eaten appearance Growth arrest lines Vertebral compression fractures Periosteal elevation Bony infiltrate 4 yr old with pallor and bony tenderness in hands Iranian Journal of Radiology. 2012 March; 9(1): 50-56. , DOI: 10.5812/iranjradiol.6765 Leukemia cutis- a case of congenital leukemia Ann Dermatol 2009; 21-66-70 Aleukemic leukemia cutis Differential diagnoses Infection Nodular mastocytosis Histiocytosis Leukemia cutis Acta Derm Venerol 91 Granulocytic sarcoma Granulocytic sarcoma and gingival hypertrophy How to evaluate a patient with suspected leukemia? Complete blood count with reticulocytes WBC: May be ↑, ↓or normal Platelets: Often ↓ Hemoglobin: Often ↓ Differential: Often neutropenia & blasts 10% of patients have “normal” CBC Usually cannot diagnose type of leukemia from CBC Evaluation of a child with suspected leukemia Chemistry panel: Electrolytes, BUN, creatinine, LDH, urate, liver function tests, serum Ca, PO4, Mg Viral studies: hepatitis panel, CMV, EBV serology ?Malaria parasite in endemic area Peripheral blood flow cytometry with presence of blasts Diagnostic Workup: CXR R/O mediastinal mass Present in 5-10% of ALL (often associated with T-cell subtype) Mass may cause respiratory obstruction Always obtain CXR prior to sedating patient Bone Marrow Examination Aspiration Morphology Immune histochemisrty Flow cytometry Cytogenetics Molecular study Biopsy CSF Examination First LP after confirmation of diagnosis of leukemia Making sure to have platelet count > 50K Avoiding traumatic LP Intrathecal chemotherapy at the same time of first LP CNS involvement Cranial nerve palsy- chloroma CSF positivity Total Cell count Cytospin blasts CNS I < 5/hpf None CNS II < 5/hpf + CNS II > 5/hpf + ALL Subtypes Early Thymocyte Intermediate Thymocyte Late Thymocyte Mature T-Cell T-Cell ALL Pluripotent Stem Cell Lymphoid Stem Cell B-Cell Precursor ALL Early Pre-B Cell Pre-B Cell Immature B Cell Burkitt's ALL Mature B cell Plasma Cell Diagnosis: Phenotype Essential for correct diagnosis of ALL Establishment of definite cell lineage ~ 50% cases will have myeloid associated antigen expression Such aberrant antigen expressions have no prognostic implications Early Thymocyte Intermediate Thymocyte Late Thymocyte Mature T-Cell T-Cell ALL Pluripotent Stem Cell Lymphoid Stem Cell B-Cell Precursor ALL Early Pre-B Cell Pre-B Cell Immature B Cell Burkitt's ALL Mature B cell Plasma Cell Diagnosis: Genotype Chromosomal analyses- karyotype Structural defects Numerical defects Molecular techniques RT-PCR FISH Gene expression profiling- experimental Outcome Acute lymphoblastic leukemia : a prototype of curable cancer Survival of Children with ALL Treated on CCG Protocols 100 Years of Diagnosis 1995-97 1993-95 1989-93 1983-89 1978-83 1975-78 1972-75 % Survival 80 60 40 1970-72 20 1968-70 0 2 4 6 8 Years after Study Entry 10 Survival probability by treatment era for patients enrolled onto Children's Oncology Group (COG) trials Five-year survival increased from 83.7% (SE, 0.4%) in 1990-1994 to 87.7% (SE, 0.4%) in 1995-1999 and to 90.4% (SE, 0.5%) in 2000-2005 Hunger S P et al. JCO 2012;30:1663-1669 ©2012 by American Society of Clinical Oncology ALL: a prototype of curable cancer Therapeutic advances- anti-leukemic and supportive care Biologic advances improving understanding of ALL pathobiology leading to identification of novel ALL subtypes Development of drug resistance Disposition of drugs in the host Precise risk stratification Optimizing risk-directed therapy (Pui CH, Evans WE. Semin Hematol 2013; 50:185-196) Risk assessment Precise risk assessment important Therapy optimization AYA treated on adult-based regimen have significantly worse prognosis Superior outcome of peds regimen Effective therapy Strict adherence to therapy Risk factors affecting prognosis of ALL Age of the patient Initial white cell count Presence or absence of CNS disease Immunophenotype of leukemic cells Genetics of leukemic cells Initial response to antileukemic treatment Risk assessment: age at ALL diagnosis Strong prognostic factor SJCRH study (n=847) 5 yr. EFS was 88% for pts 1-9 yrs 73% for 10-15 yrs 69% for >15 yrs 44% for infants Outcome of adults worsen with increasing age Risk assessment: presenting WBC Increasing counts conferring poorer outcome esp. pre-B ALL WBC ≥ 50 x 109/L categorized as high risk ALL In T-ALL WBC count > 100 x 109/L is associated with increase in CNS relapse Hyperleucocytosis esp. > 400K is associated with leucostasis Risk Assessment: Immunophenotype T cell and mature B cell phenotype are associated with higher risk of relapse With contemporary therapy may not be associated with poor prognosis May have agerelated effects 5-year EFS B-lineage 79 + 1% T-cell 75 + 4% p=0.56 DFCI ALL studies (1981-95) J Clin Oncol 2003; 21:3616 Risk assessment: Genetic features of lymphoblasts Favorable features: Hyperdiploidy (>50 chromosomes) TEL-AML1 fusion t(1;19) Trisomies 4,10 and 17 Unfavorable or high risk features BCR-ABL MLL-AF4 fusion/t(4;11) Hypodiploidy (<44 chromosomes) Age affects prognostic importance of genetic abnormalities Genetic features: iAMP21 Intrachromosomal amplification of chromosome 21 ~ 2% of children with ALL with Associated with preB-ALL Older age Low white cell count Three fold increase in relapse Blood 2007; 109; 2327-30 Risk factors affecting prognosis of ALL Age of the patient Initial white cell count Presence or absence of CNS disease Immunophenotype of leukemic cells Genetics of leukemic cells Initial response to antileukemic treatment ALL: a prototype of curable cancer Therapeutic advances- anti-leukemic and supportive care Biologic advances improving understanding of ALL pathobiology leading to identification of novel ALL subtypes Development of drug resistance Disposition of drugs in the host Precise risk stratification Optimizing risk-directed therapy (Pui CH, Evans WE. Semin Hematol 2013; 50:185-196) Earlier studies in childhood ALL recognized that patients who required longer treatment to achieve remission had a lower likelihood to maintain remission (Cancer Res 1973;33:3278-3284) How do we assess CR? Clinical examination – to confirm absence of organomegaly (liver, spleen, LN) or any leukemia lesions CBC to confirm marrow recovery from myelosuppressive chemotherapy (e.g. platelets ≥ 100K and APC ≥ 1. BM aspiration- morphology, flow cytometry BM biopsy LP with CSF examination Radiological evaluation i.e MR if CNS lesion Early response to antileukemic therapy: Funnel Effect ALL therapy Therapy adherenc e in vivo response to therapy Assessment of in vivo sensitivity of ALL Early blast cell reduction in peripheral blood (day 8) Day 15 BM End of remission-induction bone marrow (BM) response- complete remission (CR) However, majority of relapses occur in patients with M1 or M2 BM on day 15 or even those who achieve CR at the end of induction (Campana D. Curr Hematol Malg rep 2012;7:170-177; Borowitz MJ et al. Blood 2008; 111:5477-5485) Assessment of in vivo sensitivity of ALL Early response to therapy in patients with ALL predicts the risk of relapse To sharpen the predictive power of early response it is important to develop better ways to measure the treatment response To that effect understanding the leukemic cell kinetics and treatment response is important Leukemic burden at various phases of disease From: PizzoPA, Poplack DG. Eds. Principles and Practice of Pediatric Oncology, 6th Ed, Lippincot Williams & Wilkins, 2011;548 Leukemic burden at various phases of disease Thus, clinical and morphological remission is compatible with significant amounts of residual disease From: Pizzo PA, Poplack DG. Eds. Principles and Practice of Pediatric Oncology, 6 th Ed, Lippincot Williams & Wilkins, 2011;548 Leukemic burden at various phases of disease Therapy abandonment From: Pizzo PA, Poplack DG. Eds. Principles and Practice of Pediatric Oncology, 6 th Ed, Lippincot Williams & Wilkins, 2011;548 Pitfalls of morphological diagnosis of “Remission” Large number of residual blasts despite attaining “CR” Misinterpretation of “hematogones” as blasts Minimal Residual Disease (MRD) “Lingering” or “sub-morphologic” leukemia MRD is the disease that is detected by laboratory techniques more sensitive than morphology Kinetics of Leukemic cell clearance MRD estimation by flow cytometry MRD level < 10-4 Immunologic remission was achieved by 2 weeks in 49% of patients, by 6 weeks in 75% of patients 12% patients required 722 weeks whereas 13% patients required >22 weeks Pui CH, Campana D. Leukemia 2000;14:783-785 How low can you go? Depth of remission From: PizzoPA, Poplack DG. Eds. Principles and Practice of Pediatric Oncology, 6th Ed, Lippincot Williams & Wilkins, 2011;548 Minimal Residual Disease (MRD) Helps to guide therapeutic decisions: Early phases of therapy: Identify patients who responded well to therapy and hence their therapy can be minimized Those patient who require additional or intensive therapy Prior to stem cell transplant Early detection of recurrence or relapse. MRD Estimation Number of leukemic blasts present in a population of nucleated cells following therapy Major challenges: Regenerating normal immature lymphocytes Clonal evolution of leukemia How to detect MRD? Choice of technique depends on the aims for MRD estimation resource availability availability of expertise Identification of high risk (HR) patients: may use faster but less sensitive method To identify “good responders” where therapy could be minimized requires highly sensitive method How to detect MRD? PCR based method: Allele-specific oligonucleotide polymerase chain reaction (ASO PCR) analyses for immunoglobin (Ig) and T cell receptor (TCR) gene rearrangement Flow cytometry based method: Multiparametric flow cytometry (FCM) for detection of aberrant immunophenotype PCR for specific translocation like BCR-ABL, MLL gene rearrangements or TEL/AML1 Deep sequencing Deep sequencing methods High-throughput sequencing method Universally amplifies antigen-receptor gene segments and identifies all clonal gene rearrangements Capacity to identify all leukemia-specific sequences Advantages: Detect clonal evolution More precise Highly sensitive (<0.01%) (Faham M et al. Blood 2012; 120:5173-5180) MRD evaluation in relation to therapy Remission induction Consolidation Maintenance Clinical significance of MRD: ALL Multiple studies from contemporary therapeutic trial groups have endorsed the prognostic correlation of MRD levels during and end of remission induction and in the early phases of postremission therapy Independent prognostic marker End of Induction MRD is the powerful predictor of Survival: COG study Patients with new diagnoses of pre B-ALL (n=1971) Received 3 drug dexamethas one based (SR) or 4 drug (prednisone based) (HR) induction therapy (Borowitz MJ et al. Blood 2008; 111:5477-5485) Prognostic Significance of Day 8 Peripheral Blood MRD on EFS:COG study Satisfactory peripheral blood MRD (n=1920) 70% patients were MRD +ve (>0.01%) 5-year EFS for MRD -ve patients was 90% Stepwise reduction in EFS at each (Borowitz MJ et al. Blood 2008; 111:5477-5485) Risk of relapse by end of induction BM MRD: DFCI ALL Therapy Protocol 95-01 Undetectable DFCI study 95-01 (n=284) 10-6 to <10-5 10-5 tp <10-4 10-4 to <10-3 MRD estimation for pre B ALL by PCR 5-yr risk of relapse was 5% in children with no detectable MRD (n= 176) ©2007 by American Society of Hematology 10-3 to <0.01 ≥ 0.01 Zhou J et al. Blood 2007;110:1607-1611 Risk of relapse by end of induction BM MRD: DFCI ALL Therapy Protocol 95-001 <1 in 1000 Recursive partitioning and clinical characteristics identified optimal cut off level for MRD to predict outcome was 10-3 5-yr risk of relapse was 12% in children with low MRD (n= 246) compared to 72% in those with high MRD (n=38) (p<0.001) ©2007 by American Society of Hematology >1 in 1000 (Zhou J et al. Blood 2007;110:1607-1611) MRD estimation in children with de novo ALL MRD testing has redefined remission Strong body of evidence supports that MRD is an independent prognostic factor irrespective of different techniques, age group, genetic subtypes and chemotherapy regimens Major therapy groups now use MRD based risk stratification for Relapsed ALL About 20-25% of children with ALL will suffer leukemia relapse The probability of second CR with current salvage protocols is 70-95% However cure rates following first relapse are 30-40% Short duration of first CR, isolated BM relapse and T cell immunophenotype are poor prognostic features For high risk relapse ALL the cure rate is ~ 20% with allogeneic stem cell transplant Clinical trials have shown that MRD estimation is clinically informative in children with second CR (Blood 1991;78:1166-72; Cancer 1998; 82:1387-95; Br J Haematol 2000;108:531-43 and 2002:118:741-7, J Clin Oncol 2005:23:7942-50) Infant Leukemia ALL or AML diagnosed before the age of 1 year Rare but extremely challenging Estimated incidence in US: 41 cases per million per yr ~160 cases; 90 with ALL Aggressive clinical presentation High WBC Large hepatosplenomegaly CNS disease Leukemia cutis Infant Leukemia: Role of MLLr in leukemogenesis Characterized by balance translocation involving mixed lineage leukemia (MLL) gene at locus 11q23 MLL gene rearrangement (MLLr) ocurrs in ~ 70%-80% of infant ALL and ~50% in infant AML Over 79 partner genes- common in ALL are AF4, ENL, AF9 and AF10 whereas AF9, AF10 and EML in AML Acquired in hematopoietic precursers in utero Infant leukemia Infant ALL with MLLr CD10 negativity + ≥ 1 myeloid markers Poor prognostic factor (EFS ~35% in MLLr compared to 60-70% in MLLg) Chemoresistant phenotype common Infant AML with MLLr Monocytic differentiation No prognostic implication Infant ALL: Management Vulnerable host – increased risk of complications and toxicities Rapidly changing physiology High induction death rates (15% to 25%) Long term effects on survivors Risk based therapy Brown P. ASH Educational Book 296 Treatment strategy Induction Consolidation & CNS prophylaxis Maintenance Risk Stratifications Total length of therapy 2 -3 years Hamilton – Dana Faber Cancer Institute Remission Induction Phase Goal To eradicate 99% leukemic cell burden Restore normal hematopoiesis and Healthy PS 3- 4 or more drugs in combination including glucocorticosteroid CR- change in definition CR in 96-99% children and 78-93% adults Consolidation (Intensification) therapy Goals To eradicate drug-resistant residual leukemic cells To reduce risk of relapse Various combinations of drugs Asparaginase HD MTX ARA-C CTX Anthracylines intensification Continuation (Maintenance) Therapy Goal To ~ 60% of children with ALL can be cured by 12 months of therapy No prevent or delay relapse prospective criteria identified All pts receive 2-2.5 yr therapy Mercaptopurine and low dose MTX form mainstay of therapy Dose adjustment to ANC nadir Thioguanine vs. mercaptopurines 6TG more potent than 6MP Leads to higher intarcellular and CSF concentration Produces superior antileukemic respoonse However associated severe toxicities Severe thrombocytopenia Increased rate of death in CR Very high rate (10-20%) of hepatic VOD CNS-directed therapy CNS relapse- major obstacle in earlier trials (30-40% relapses) Risk factors T cell ALL Hyperleukocytosis High risk genetic abnormalities (Ph +ve ALL. MLL gene rearrangement) Presence of leukemic cells in CSF (including iatrogeneic introduction) Allogeneic HSCT Reserved only for certain subtypes of ALL Philadelphia +ve ALL esp in combination with TKI Poor respons eto initial therapy Adults with HR disease Role in Infant ALL unclear Role in relapsed ALL Newer therapies Newer Therapies Immunotherapy Anti CD 20, CD 22, anti CD52 antibodies CAR-T cells Novel transplant procedures Haplotransplant Blinatumomab: Anti-CD19 monoclonal antibody 1 - Enables a patients T-Cells to recognize Malignant B-cells 2 - Has 2 binding sites - CD3 on T-Cell and CD19 on B-cells 3 - After linking the 2 cells it activates the T-Cell to exert cytotoxic activity on the target B-Cell. CD19 December 2014 approved for use by FDA for relapsed/refractory (Ph-) B-ALL. When launched it was the most expensive cancer drug on the market. ($64,260/mo) Pui et al. Lancet 2008; 371:1030-43 How do we relate this information to children in low income countries? Childhood cancer in LIC 80% of children affected with cancer live in low or middle income countries Overall survival is very poor for these children even with low risk cancers like ALL What are the challenges? Challenges- systems disorder Delayed or no diagnosis Lack of proper therapy Therapy abandonment What is the situation in Zambia? Study by Slone and Chunda-Liyoka et al (PLoS One 9; e89102) ~52% children had cancer diagnosis confirmed by histopathology Mortality on therapy was 46% Abondonment was 46% How can we change this situation? Thank you