Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
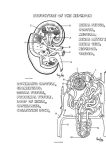
RENAL PHYSIOLOGY DR SYED SHAHID HABIB MBBS DSDM FCPS Associate Professor Dept. of Physiology College of Medicine & KKUH Renal Physiology 1) 2) 3) 4) 5) Introduction Glomerular Filtration Tubular Processing Urine Concentrating Mechanism Micturition RENAL PHYSIOLOGY TUBULAR PROCESSING TUBULAR REABSORPTION & SECRETION URINE COMPOSITION pH usually acidic (pH 6) range= 4.8 - 7.5 Colour Volume Bright Yellow & transparent 1 - 2 L per day Glucose None REABSORTION PATHWAYS inulin urea gluc Creat Urinary Excretion Rate = Filtration Rate – Reabsorption Rate + Secretion Rate % of Filtered Load Reabsorbed Glucose (g/day) Urea Glucose Bicarbonate (mEq/day) Sodium (mEq/day) Chloride (mEq/day) Potassium (mEq/day) Urea (g/day) Creatinine (g/day) 100 >99.9 99.4 99.1 87.8 50 0 PROXIMAL CONVOLUTED TUBULE • • • • many mitochondria brush border tight junctions lateral intercellular spaces. GLUCOSE AND AMINO ACID REABSORPTION IN NEPHRON TUBULAR TRANSPORT MAXIMUM • The Maximum limit/rate at which a solute can be transported across the tubular cells of kidneys is called TUBULAR TRANSPORT MAXIMUM Tm for Glucose is 375 mg/min GLUCOSE REABSORPTION Transport max 375 mg/min Renal Threshold 200mg/dl •FBG=60-110 mg/dl •RBG=110-200 mg/dl HYDROGEN •Secreted in Proximal Tubule and LOH by Counter Transport with Na Na-H COUNTER TRANSPORT Luminal Membrane PCT & LOH PCT Cotransport Cotransport Na G Na AA water Reabsoprtion 65% Na Na H+ Countertransport ATP K Cl- SODIUM HANDLING Na+ moves by co transport or exchange from the tubular lumen into tubular epithelial cells From cells into interstitium it moves by primary active transport In DCT and CT it is under hormonal control SODIUM HANDLING Renal tubular reabsorption Solute reaborption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma). 65% of water and sodium reabsorption occurs in the proximal tubule 100% of glucose & amino acids Proximal tubules: coarse adjustment Distal tubules: fine adjustment (hormonal control). THIN LOOP OF HENLE • few mitochondria • flattened with few microvilli THIN DESCENDING LOOP OF HENLE • few mitochondria • flattened with few microvilli Solutes H2O THICK ASCENDING LOOP OF HANLE AND EARLY DCT Many mitochondria and microvilli, but fewer than in the proximal tubule ASCENDING LOOP OF HENLE Many mitochondria and microvilli, but fewer than in the proximal tubule Solutes H2O ECF Epithelial Cells Events in Thick ALOH Sodium potassium 2 chloride co transport Lumen Absorption through loop of Henle: Descending limb: is water permeable and allow absorption of 15% of filtered H2O. It is impermeable to Na-CL. Thin ascending limb: is impermeable to H2O, but permeable to Na-Cl, where they are absorbed passively in this part . Thick ascending limb: is impermeable to H2O. Na-K-2Cl co-transport occur in this part (25% of Na). ASCENDING LOOP OF HENLE Na-H COUNTER TRANSPORT Luminal Membrane HYDROGEN •Secreted in Proximal Tubule and LOH by Counter Transport with Na PCT & LOH LATE DCT AND CORTICAL COLLECTING DUCT • Mitochondria and microvilli decrease. • Principal Cells (Na Abs and ADH related Water abs) • Intercalated Cells (Acid Sec and HCO3 Transport) DCT AND COLLECTING DUCT I Cell P Cell •Principal Cells (Water reabsortion) •Intercalated Cells (Acid Secretion) Events in DCT Intercalated cell Events in DCT & CT Aldosterone Events in DCT & CT Principal Cell Distal convoluted tubule and collecting ducts • What happens here depends on hormonal control: • Aldosterone affects Na+ and K+ • ADH – facultative water reabsorption FACTORS AFFECTING ADH Increase ADH ↑Osmolarity ↓ Blood volume ↓ Blood pressure Decrease ADH ↓Osmolarity ↑ Blood volume ↑ Blood pressure Clinical applications • Thiazide diuretics • Loop diuretics: • K+ sparring diuretics: MEDULLARY COLLECTING DUCT REABSORPTION OF WATER IN DIFFERENT SEGMENTS OF TUBULES PART OF NEPHRON Proximal tubules PERCENTAGE REABSORBED 65 Loop of Henle 15 Distal tubules 10 Collecting ducts 9.2 Passing into urine 0.8 RENAL PHYSIOLOGY TUBULAR SECRETION DR SYED SHAHID HABIB MBBS, FCPS TUBULAR SECRETION • Tubular Secretion may be by Passive or Active Mechanisms • The most important secretory processes are for H, K and Organic Ions HYDROGEN • Secreted in Proximal Tubule by Counter Transport with Na • In DCT and CT it is secreted by Hydrogen ATP ase • When body fluids are more acidic H secretory process is accelerated and Vice Versa HYDROGEN •Secreted in Proximal Tubule and LOH by Counter Transport with Na •Secreted in DCT by H ATP ase Primary Active Transport Na-H COUNTER TRANSPORT Luminal Membrane PCT & LOH I Cell in DCT RENAL PHYSIOLOGY COUNTER CURRENT MECHANISM COUNTER CURRENT MECHANISM • KIDNEYS HAVE – MECHANISMS FOR EXCRETING EXCESS WATER – MECHANISMS FOR EXCRETING EXCESS SOLUTES NEPHRON TYPES Superficial (cortical) [85 %] o Capable of forming dilute urine Juxtamedullary [15 %] o Capable of forming concentrated (> 300 mOsm/kg) urine EXCRETION LIMITS • At least 600 mmol of solutes must be excreted each day – minimum volume = 600/1200 = 0.5L – maximum volume = 20 Liters EXCRETION LIMITS COUNTER CURRENT MECHANISM • LOOPS OF HENLE OF JUXTA MEDULLARY NEPHRONS establish hyperosmolality of interstitium of medulla. They are called COUNTER CURRENT MULTIPLIERS • VASA RECTA maintain hyperosmolality established by counter current multipliers. They are called COUNTER CURRENT EXCHANGERS 300 300 200 300 300 250 400 400 300 500 500 400 600 600 500 700 700 600 800 800 800 1000 1000 1000 300 Cortex Medulla 300 300 400 Osmolality 1200 1200 1200 DISORDERS OF URINARY CONCENTRATING ABILITY • Failure to Produce ADH: "Central" Diabetes Insipidus. • Inability of the Kidneys to Respond to ADH: "Nephrogenic" Diabetes Insipidus. RENAL PHYSIOLOGY MICTURITION DR SYED SHAHID HABIB MBBS DSDM FCPS Assistant Professor Dept. of Physiology College of Medicine & KKUH MICTURITION It is the process by which the urinary bladder empties when it becomes filled Filling of bladder. Micturition reflex. Voluntary control. Nervous Connections of the Bladder Urogenital diaphragm Micturition Reflex • Actions of the internal urethral sphincter and the external urethral sphincter are regulated by reflex control center located in the spinal cord. – Filling of the urinary bladder activates the stretch receptors, that send impulses to the micturition center. • Activates parasympathetic neurons, causing rhythmic contraction of the detrusor muscle and relaxation of the internal urethral sphincter. – Voluntary control over the external urethral sphincter. • When urination occurs, descending motor tracts to the micturition center inhibit somatic motor fibers of the external urethral sphincter. AUTONOMIC SPINAL REFLEX INNERVATION OF THE BLADDER Nerves 1 Pelvic nerves (parasympathetic fibers) Characteristic Function Both sensory and motor nerve fibers Contraction of bladder The sensory fibers detect the degree of stretch in the bladder wall S-2 and S-3 2 Pudendal Nerve somatic nerve Fibers that innervate and control the voluntary skeletal muscle of the sphincter 3 Hypogastric Nerves sympathetic innervation (L2) Stimulate mainly the blood vessels and have little to do with bladder contraction. Sensory nerve fibers of the sympathetic nerves also mediate the sensation of fullness and pain. CYSTOMETROGRAM