Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
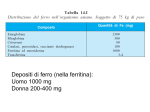
Intossicazione da Pb Fonti ambientali • Costruzione di condutture per scarichi urbani in aumento fino alla seconda guerra mondiale, poi sostituito con materie plastiche. • Batterie • Additivo nelle benzine • Incenerimento dei rifiuti • Industrie metallurgiche NOTA BENE: Il Pb presente negli alimenti deriva soprattutto da inquinamento ambientale Tossicità • Assorbimento più elevato nei giovani • Bersagli primari i globuli rossi, poi il sistema cardiovascolare, gastrointestinale, nervoso, riproduttivo e renale. • Alcuni enzimi della via biosintetica dell’eme sono suscettibili all’intossicazione da Pb: eme sintetasi, d-ALAD (deidrasi), ferrochelatasi, d-ALAS (sintasi), uroporfirinogeno decarbossilasi e coproporfirinogeno ossidasi. Biosintesi dell’eme Ala-sintasi Ala-deidrasi Ferrochelatasi mitocondrio ALA deidrasi citoplasma •ALA deidrasi: ottamero ogni subunità lega 8 ioni Zn, 4 dei quali sono essenziali per l’attività; quando Pb si lega al posto dello Zn si ha inibizione enzimatica. •I conseguenti alti livelli di ALA nel sangue sono responsabili dei disordini neurologici provocati dal Pb. ALA ha struttura simile a GABA (g-aminobutirrico) Test clinici • Misura del Pb ematico (piombemia): il più specifico!!! • Misura della protoporfirina: dal momento che il Pb inibisce la ALA-deidrasi e la ferrochelatasi si accumulano acido delta aminolevulinico e protoporfirina; valori di quest’ultima >35 mg/dL ; Anche nelle anemie da carenza di Fe • Misura della inibizione di ALA-deidrasi Caso clinico 1 • Merryl ha bevuto per diversi giorni acqua contaminata con Pb. [Pb] ematica di 0,9 ppm (mg/L di sangue) • E’ stato curato subito con un chelante (Ca-EDTA) Merryl Caso clinico 2: intossicazione acuta • Aki presentava convulsioni • Misura Pb ematico: 1,3 ppm • Dopo una settimana (senza cura!!): 0,65 ppm • Dopo due settimane e 3 giorni di cura con EDTA: 0,27 ppm • Alla fine della cura: 0,26 ppm • NB: nei cani di controllo 0,05 ppm Pb ematico (come nell’uomo) Aki I bovini della Slovenia • Da uno studio condotto in Slovenia: caso di intossicazione cronica • Nel 1975 1,2 ppm di sangue • Nel 1982 0,25 ppm • Nel 2002 0,05 ppm Gli uccelli acquatici • In uccelli marini, valori di riferimento di 0,045 ppm per zone non contaminate; • Fino a 1,9 ppm in uccelli che avevano ingerito vernici contenenti Pb nei pressi di una base militare in disuso – Heme Metabolism – The largest repository of heme in the human body is in red blood cells, which have a life span of about 120 days. There is thus a turnover of about 6 g/day of hemoglobin, which presents 2 problems. First, the porphyrin ring is hydrophobic and must be solubilized to be excreted. Second, iron must be conserved for new heme synthesis. – Normally, senescent red blood cells and heme from other sources are engulfed by cells of the reticuloendothelial system. The globin is recycled or converted into amino acids, which in turn are recycled or catabolized as required. Heme is oxidized, with the heme ring being opened by the endoplasmic reticulum enzyme, heme oxygenase. The oxidation step requires heme as a substrate, and any hemin (Fe3+) is reduced to heme (Fe2+) prior to oxidation by heme oxygenase. The oxidation occurs on a specific carbon producing the linear tetrapyrrole biliverdin, ferric iron (Fe3+), and carbon monoxide (CO). This is the only reaction in the body that is known to produce CO. Most of the CO is excreted through the lungs, with the result that the CO content of expired air is a direct measure of the activity of heme oxygenase in an individual. – In the next reaction a second bridging methylene (between rings III and IV) is reduced by biliverdin reductase, producing bilirubin. Bilirubin is significantly less extensively conjugated than biliverdin causing a change in the color of the molecule from blue-green (biliverdin) to yellow-red (bilirubin). The latter catabolic changes in the structure of tetrapyrroles are responsible for the progressive changes in color of a hematoma, or bruise, in which the damaged tissue changes its color from an initial dark blue to a red-yellow and finally to a yellow color before all the pigment is transported out of the affected tissue. Peripherally arising bilirubin is transported to the liver in association with albumin, where the remaining catabolic reactions take place. • In hepatocytes, UDP glucuronyl transferase adds 2 equivalents of glucuronic acid to bilirubin to produce the more water soluble, bilirubin diglucuronide derivative. The increased water solubility of the tetrapyrrole facilitates its excretion with the remainder of the bile as the bile pigments. • In individuals with abnormally high red cell lysis, or liver damage with obstruction of the bile duct, the bilirubin and its precursors accumulate in the circulation; the result is hyperbilirubinemia, the cause of the abnormal body pigmentation known as jaundice. In normal individuals, intestinal bilirubin is acted on by bacteria to produce the final porphyrin products, urobilinogens and urobilins, that are found in the feces. Bilirubin and its catabolic products are collectively known as the bile pigments.