Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
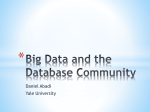
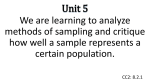
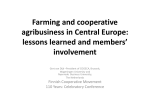
The Impact of Drug Benefit Caps Geoffrey Joyce, PhD Acknowledgements Collaborators: Dana Goldman Pinar Karaca-Mandic This research was funded by: National Institute on Aging A6794c-2 6/06 Benefit Cap • Annual limit on the plan’s contribution • In this case, $2,500 benefit cap • Common in Medicare M+C plans • Impact of caps on retirees < age 65 and 65+ in 2003-2004 A6794c-3 6/06 Imposing a Spending Cap Creates a Fundamental Trade-off Imposing a spending cap decreases the cost to provide the prescription benefit Makes coverage available to more beneficiaries A spending cap creates a coverage gap (or “donut hole”) for beneficiaries Increases the risk that patients will reduce or cease drug therapy A6794c-4 6/06 As Set Up, Medicare Part D Raises Some Issues Stop-Loss $5,100 ($3,600 in out-of-pocket) Catastrophic Coverage Catastrophic Coverage Insurer Pays Insurer Pays 95% ofCosts Costs 90% of Beneficiary Pays Next $2,850 in Rx Spending 5% Cost-Sharing Above Stop-Loss Beneficiary Paid Insurer Paid Initial Coverage Limit $2,250 75% Paid by 50% of Costs Paid Plan by Insurer ($1,500) ($2,113) 25% Copay ($500) $250 Deductible 2006 A6794c-5 6/06 Tseng et al (2004): Surveyed Beneficiaries to Assess the Effects of Spending Caps 1,300 Medicare+Choice enrollees in one state in 2001: Group who exceeded their annual prescription benefit cap of $750 or $1,200 Matched controls who did not exceed their annual cap of $2,000 Those exceeding the cap had resulting coverage gaps of 75–180 days A6794c-6 6/06 Beneficiaries Reported Using Several Strategies When They Exceeded Caps Switched Drugs 15 (9) Used Drugs Less Often 18 (10) Used Free Samples 34 (27) 0 10 20 30 40 Percent of Beneficiaries Using Strategy A6794c-7 6/06 Hsu et al (2006): Impact of $1,000 Cap on Utilization, Costs, & Clinical Measures Compared clinical and economic outcomes in 2003 among Kaiser M+C members in capped vs. noncapped plans in 2002-2003 (age 65+) Employer-supplemental insurance – No cap Individual-purchased - $1,000 benefit cap About 13% reached the cap in 2003 Those in capped plan: 31% lower Rx costs No difference in total medical costs A6794c-8 6/06 Hsu et al (2006) But had higher rates of ED visits (RR=1.09) Nonelective hospitalizations (RR=1.13) Mortality rate (1.22) Non-adherence (1.2-1.3) Capped members had higher odds (1.2 – 1.3) Elevated LDL Systolic blood pressure HbA1c A6794c-9 6/06 Aims of This Study Examine Rx utilization and costs in more detail Behavior pre- and post-cap Timing of cap Stopping, switching, mail-order use, by class Do those who stop resume drug therapy in subsequent year Impact on hospitalizations and ED visits A6794c-10 6/06 Data & Methods We linked health care claims to health plan benefits of 30 large employers (1997-2004) Over 50 health plans Nearly 8 million person-years Analyze 7 plans in 2003-2004 from large employer 2 plans had an annual Rx benefit cap of $2,500 Compare Rx and medical use Among groups within the same (capped) plan Among persons in capped vs. uncapped plans A6794c-11 6/06 Distribution of Health Plan Spending in Capped Plans (PPPY) PPPY Spending by Health Plan < $2,400 $2,401$2,499 >= $2,500 N % 6,843 94.1 192 2.6 239 3.3 N % 25,972 88.6 1,359 4.6 1,981 6.8 Plan 1 Plan 2 A6794c-12 6/06 Classify Members Into 3 Groups Group 0: Rx spending by the health plan <= $2,400 Group 1: Rx spending by the health plan > $2,400 But no subsequent Rx claims Group 2: Rx spending by the health plan > $2,400 With subsequent Rx claims A6794c-13 6/06 When Do Members Reach the Cap? Percentile of Those Reaching the Cap th 5th 10th 25th 50th 75th 90 Feb April June Sept Nov Dec A6794c-14 6/06 Monthly Rx Spending in Capped vs. Non-capped Plans (>$2,400) PMPM Rx Spending 700 600 500 400 300 200 100 0 1 2 3 4 5 6 7 8 9 10 11 12 Month in 2004 A6794c-15 6/06 Monthly Rx Use in Capped vs. Non-capped Plans (>$2,400) PMPM N30DE Scripts 12 10 8 6 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 Month in 2004 A6794c-16 6/06 Percent Switching Medications Post-Cap (Among Those Reaching the Cap Before November) Diabetes Percent Switching Post-Cap Cap No Cap 3.3 5.8 Cardiac 9.6 8.1 Hypertension 7.2 6.3 Depression 4.2 6.1 Cholesterol 2.1 2.4 A6794c-17 6/06 Percent Stopping Medications Post-Cap (Among Those Reaching the Cap Before November) Diabetes Percent Stopping Post-Cap Cap No Cap 4.9 3.3 Cardiac 5.2 5.4 Hypertension 7.0 6.6 Depression 16.4 8.7 Cholesterol 13.0 4.8 A6794c-18 6/06 Resumption of Medication Use • Among those who stopped taking a class of medications in capped plans Modest take-up in Q1 of 2004 May be related to data problem in 2003 A6794c-19 6/06 Preliminary Conclusions Imposing a spending cap: Reduces Rx use overall 50% - 66% reductions in Nov-December Effects vary modestly by therapeutic class Increases the risk of adverse health outcomes Inconsistent evidence on medical use A6794c-20 6/06