Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
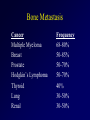
Cancer Pain Management ancer Cancer Statistics: 2010 (ACS, 2010) • One-third of Americans born this year will develop cancer. • Cancer is the second leading cause of death among Americans, accounting for 1 of every 4 deaths. • It will occur in approximately 1,529,560 people and account for about 569,490 deaths this year. • Life-time risk: – Men – 1:2 – Women – 1:3 2010 Estimated US Cancer Cases* Men 789,620 Women 739,940 Prostate 28% 28% Breast Lung & bronchus 15% 14% Lung & bronchus Colon & rectum 9% 10% Colon & rectum Urinary bladder 7% 6% Uterine corpus Melanoma of skin 5% 4% Non-Hodgkin lymphoma Non-Hodgkin lymphoma 4% 4% Melanoma of skin Kidney & renal pelvis 4% 5% Thyroid Oral Cavity & pharynx 3% 3% Leukemia Leukemia 3% 3% Pancreas Pancreas 3% 3% Ovary 20% 3% Kidney & renal pelvis All Other Sites 25% All Other Sites *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2009. 2010 Estimated US Cancer Deaths Lung & bronchus 29% Prostate 11% Men 299,200 Women 270,290 26% Lung & bronchus 15% Breast Colon & rectum 9% 9% Colon & rectum Pancreas 6% 5% Ovary Leukemia 4% 7% Pancreas Esophagus 4% 3% Leukemia Liver & intrahepatic bile duct 4% 4% Non-Hodgkin lymphoma Non-Hodgkin lymphoma 4% 3% Uterine corpus Urinary bladder 3% 2% Liver & intrahepatic Kidney & renal pelvis 3% All other sites 24% bile duct 2% 24% ONS=Other nervous system. Source: American Cancer Society, 2009. Brain/ONS All other sites Cancer Pain: Prevalence • 50% of patients in all stages have pain • 70% - 90 % of patients with advanced disease have moderate-severe pain • I • Inadequate pain control adds to morbidity, mortality, decreased quality of life, and increased costs of care Prevalence of Cancer-Related Pain • World Health Organization estimates 3.5 million people suffer from unrelieved cancer pain each day • Newly diagnosed cancer: 28% • Actively receiving anticancer treatment: 50-70% • Advanced disease: 70-80% – 40-50% report it as moderate - severe; up to 30% report their pain as very severe • Nursing home residents with cancer: – 45-80% have substantially under-treated pain Patient is cancer-free and still has pain • Cancer treatment results in “non-malignant” pain – Post-thoracotomy pain – Post-mastectomy pain – Post-amputation pain • Phantom Limb pain • Stump/Neuroma pain – Chemotherapy-induced painful peripheral neuropathy (CIPN) – Radiation Therapy injuries Pain Follow-up • How do you treat the patient after their cancer has been cured or is in remission? • The line between “malignant” pain and “chronic” pain becomes obscured • Standard opioid medication therapy may not be the most appropriate treatment The Experience of Pain Requires Telling a Personal Story & for Someone to Hear It • Are there differences in the way one tells a personal story? • Are there differences in the way one listens to a personal story? • Are there gender differences? Is There Time to Hear Our Patient’s Pain Story? • • • • Time limitations Competing priorities Distractions Distancing • The average length of a patient’s opening statement is three minutes – 77% of the time, we interrupt within the first 2 minutes – Research shows that 99% of time, once a patient has been interrupted, he/she does not get a second chance (Dr. Neil Irick, N., 2004; 29th ONS Congress Lecture) Pain Assessment in Oncology • Pain history – Location, intensity, quality, temporal patterns, aggravating/alleviating factors – Current and past medication use, include OTC – Meaning of pain • Physical examination • Laboratory evaluation • Reassess frequently Categorizing Cancer Pain • Acute vs. chronic • Etiology (related to cancer or its treatment) • Quality (nociceptive vs. neuropathic) • Multiple sites and types of pain are common Pain Syndromes in Oncology: Acute vs. Chronic Pain • Acute pain – – – – Associated with diagnostic procedures Associated with therapeutic interventions Associated with infection Associated with vascular events • Chronic pain or persistent Acute Pain Syndromes in Oncology • Pain associated with diagnostic procedures – Lumbar punctures – Bone marrow biopsies • Pain associated with therapeutic interventions – Postoperative pain – Tumor embolization – Pleurodesis for pleural effusions Acute Pain Syndromes in Oncology • Pain associated with infection – Acute herpetic neuralgia (shingles) • Pain associated with vascular events – Deep vein thrombosis – Superior vena cava syndrome Pain Syndromes in Oncology: Etiology • Pain associated with the cancer – Bone metastases, liver tumor • Pain associated with cancer treatment – Painful peripheral neuropathy from chemotherapy, postsurgical pain, flare from hormonal therapy, osteoradionecrosis from radiation therapy • Pain unrelated to cancer or its treatment – Arthritis, diabetes Common Nociceptive Pain Syndromes in Cancer • Bone pain due to metastases • Arthralgias due to taxane therapy • Mucositis pain • Surgical pain Bone Pain • • • • >75% Dull ache Intermittent to continuous Continuous with progression of cancer • May worsen at night • Reduced function • Tenderness when tapped Bone Metastasis Cancer Multiple Myeloma Breast Prostate Hodgkin’s Lymphoma Thyroid Lung Renal Frequency 68-80% 50-85% 50-70% 50-70% 40% 30-50% 30-50% Common Sites Site Rib Cage Spine Pelvis Limbs Skull Frequency 58% 54% 40% 32% 19% Common Visceral Pain Syndromes in Cancer • Liver capsule distension • Malignant bowel obstruction • Ureteric obstruction Common Neuropathic Pain Syndromes in Cancer • Post-radiation plexopathies • Surgical neuropathies – postmastectomy syndrome • Brachial plexus neuropathies – lung or breast cancers • Spinal cord compression • Cranial neuropathies – head & neck, breast or lung cancers • Chemotherapy-induced neuropathy – Bortezomib – Cisplatin – Oxaliplatin – Taxanes – Vinblastine – Vincristine Neuropathic pain: State of the Problem Jenson, Madsen, Finnerup (2009); Backonja, M & Woolf, G. J. (2010) • 2/3’s of patients with NP do not get sufficient pain relief by current available treatment • Review of recent clinical trials: – 30-40% of patients with neuropathic pain may achieve >40-50% satisfactory pain relief Backonja, M. & Woolf, C. (2010). • All current treatments for NP are symptomatic rather than disease modifying or curative APS Principles of Analgesic Use in the Treatment of Acute Pain & Cancer Pain, 6th Edition (2008) NCCN Guidelines for Adult Cancer Pain 2010 National Comprehensive Cancer Network (www.NCCN.org) • Consensus statement • Provides algorithms for: – Pain Assessment • Pain scale suggestions for different populations – Pain Treatment and dosing suggestions • Opioid • Non-opioid analgesics • Adjuvants – Very specific and complex Goals of Cancer Pain Treatment • • • • Prevention Determine patient’s and family’s goals Decrease pain Prevent/manage adverse effects associated with treatment • Promote patient safety and function • Enhance quality of life Ideal Optimal Pharmacologic Pain Management Plan Evidence-Based Plan: • Right pain medication(s) • Right dose(s) • Right route • Right time • Right schedule • Minimal adverse side effects • Optimal outcomes – Analgesia/Pain relief – Improved function/Activities of Daily Living – Improved HR-QOL Management of Cancer Pain • Treatment of the Cancer – – – – – – – Chemotherapy Hormonal Therapy Biological Response modifiers Bisphosphonates Radiation Therapy Surgery Intraveneous radiopharmaceuticals • Treatment of the Pain: prevention and management – Pharmacologic strategies: nociceptive & neuropathic – Nonpharmacological strategies • Treatment of the Person: dimensions of pain Etiology-Based Pain Management: Pharmacological Interventions Pain Nociceptive Neuropathic CNS Medicated Somatic Non-Selective Long-acting Visceral Neuralgia Neuropathy Selective NSAIDS Opioids PNS Medicated Anti-Convulsants Short-acting Corticosteroids Tramadol/Tapentadol Baclofen Antidepressants Pharmacological Management of Cancer Pain • Nonopioids • Opioids • Adjuvants • Cancer therapies Special Considerations • Allergies/sensitivities to medications • Chronic pain history • Opioid tolerance • Chemical-dependence • Hepatic impairment • Renal impairment • Elderly patients Nonopioids • Acetaminophen – Analgesic and antipyretic – Use with caution in primary liver or metastatic disease • Nonsteroidal anti-inflammatory drugs – Analgesic, antipyretic and antiinflammatory – Contraindicated in thrombocytopenia due to chemotherapy or bone marrow involvement – Contraindicated in renal compromise (esp. multiple myeloma) – Should not be used concomitantly with steroids Opioid Use in Oncology & EOL Opioids Used in Oncology • • • • • • • Fentanyl Hydrocodone Hydromorphone Methadone Morphine Oxycodone Oxymorphone Opioid Pharmacokinetics • Most short-acting opioids act in a similar fashion – PO: peak 1 hour, duration 3-4 hours – IV: peak 15 minutes, duration 1-2 hours Long-acting Opioids • • • • • Morphine Oxycodone Fentanyl Methadone Oxymorphone Opioid Agonists “Short-acting” • Morphine • Hydromorphone • Oxymorphone • Codeine • Hydrocodone • Oxycodone “Ultra-short acting” • Fentanyl IV, TM – Fentora, Actiq, Onsolis “Longer-acting” • Extended release morphine – MS Contin, Oramorph SR, Kadian, Avinza, various generics • Oxymorphone ER – Opana ER • Oxycodone ER – Oxycontin • Hydrocodone ER – Exalgo • Methadone • Levorphanol • Transdermal fentanyl Cancer Breakthrough Pain (BTP) • Defined as a transitory increase or flare of moderate-tosevere pain that occurs in patients in a background of otherwise controlled persistent pain, using regularly scheduled doses of pain medication • Mean number 6/day • Average time to peak pain 3 minutes; range 1 second to 30 minutes • Three subtypes – Movement or incident pain – End of dose failure – Idiopathic (unpredictable, most episodes) Breakthrough Dosing • Incident and idiopathic BTP: – may require short-acting pain medications or non-pharmacologic interventions as needed, along with their scheduled pain medications. • End-of-dose BTP – may require an increase in the dosage of ATC pain medication or a decrease in the interval between doses. • PO – 10 – 20% of 24-hour long-acting opioid dose – Example: Long-acting morphine 200 mg q 12; breakthrough dose 40 – 80 mg of short-acting morphine • IV or SQ – 50 – 100% of the hourly rate – Example: Continuous infusion IV morphine 6 mg/hour; bolus or breakthrough dose 3 – 6 mg IV every 15 minutes as needed Routes of Administration • Oral • Transdermal – Passive – Iontophoretic • • • • Sublingual Buccal Rectal/stomal Nasal • • • • • Subcutaneous Intravenous Epidural Intrathecal Intramuscular – not recommended Adverse Effects of Opioids • • • • • • Sedation Nausea and vomiting Urinary retention Cognitive slowing Pruritus Respiratory depression (sedation precedes) – Use naloxone only when poor oxygenation; administer small increments to prevent withdrawal syndrome Adverse Effects of Opioids • Constipation (don’t build tolerance) • Myoclonus – usually in high doses & renal impairment • Diaphoresis • Hormonal changes (lowered testosterone) • Immune changes Constipation • Opioids inhibit peristalsis and increase resorption of fluid into lining of gut • People with cancer often have multiple etiologies to constipation • To prevent constipation, use stool softener and a laxative Methylnaltrexone Bromide Relistor® Opioid-induced Constipation in Advanced Disease • FDA approval 2008 • Methylnaltrexone bromide – indicated for the treatment of opioid-induced constipation in patients with advanced illness who are receiving palliative care, when response to laxative therapy has not been sufficient. – Subcutaneous injection dosed according to weight every other day with no more than 1 dose in 24 hour period General Strategies to Manage Opioid Side Effects • Decrease opioid dose • Change the route of administration • Pharmacologic management of side effects • Opioid Rotation Opioid Equianalgesic Conversion • Indications: – Converting between different opioids • Unresponsiveness to one opioid • Intolerable adverse effects – Converting an opioid from oral to parenteral route – Converting an opioid from parenteral to oral route Equianalgesic Dosing Drug Oral (mg) IV (mg) Duration (h) morphine 30 10 3-4 hydromorphone 7.5 1.5 3-4 oxymorphone 10 1 >4 methadone 2-5 2-5 6 – 8? 200 130 3-4 20-30 30 - 3-4 3-4 codeine oxycodone hydrocodone meperidine 300 100 2-3 McPherson, M. L. 2010 Patient Controlled Analgesia • Intraveneous or Oral • Assess previous opioid experience • Indications • Special Considerations: – Basal rates/demand doses – Education – Proxy administration: family & nurse Adjuvants • Corticosteroids • Antidepressants • Antiepileptics • Local anesthetics Corticosteroids • Inhibit prostaglandin synthesis & reduce edema • Uses: spinal cord compression, neuropathic pain, bone pain and visceral pain • Dexamethasone has least mineralocorticoid effect • Due to its long half-life, dexamethasone should be ordered every morning to prevents sleeplessness when doses are given in the evening. • Doses: variable and based on pain symptom • May produce psychosis, euphoria • Long term use (4-6 weeks) can cause proximal muscle wasting • Elevated blood sugar, especially in pancreatic cancer, diabetes Neuropathic Pain Management First-Line Medications Dworkin RH, et al. (2007). Pharmacologic management of neuropathic pain: evidencebased recommendations. Pain, 132(3):237-51. • Individual variation in the response to the medications used to treat NP is substantial and unpredictable. • First-line medications (Grade A recommendation) – Tricyclic antidepressants (TCAs) – Selective serotonin and norepinephrine reuptake inhibitors (SSNRIs) – Calcium channel alpha 2-delta ligands – Topical lidocaine Tricyclic Antidepresants (TCA) • Systematic reviews consistently conclude the support the efficacy for TCA therapy in NP (especially PHN & painful DPN) • Mechanism of action: inhibit presynaptic neuronal reuptake of norepinephrine & serotonin at the descending tract • Secondary amine TCAs better tolerated & preferred – Nortriptyline & desipramine • Tertiary amine TCA only if secondary amine not available – Amitriptyline & imipramine • Major side effects: sedation, dry mouth, blurred vision, weight gain, constipation, urinary retention, orthostatic hypotension Tricyclic Antidepresants (TCA) • Precautions: cardiac disease, glaucoma, suicide risk, seizure disorder, concomitant use of tramadol • Nortriptyline associated with cardiac toxicity risk – sinus tachycardia, increased ventricular ectopy in patients with ischemic heart disease – increased sudden cardiac death at dosages > 100mg/day • Recommended: – contraindicated in patients w/ ischemic heart disease & risk for sudden cardiac death – caution in patient at risk for suicide – screening EKG at initiation for patients > 40 years. Selective Serotonin & Norepinephrine Reuptake Inhibitors (SSNRI) • Mechanism of action: inhibit sustained high-frequency neuronal firing by blocking sodium channels after an action potential, reducing excitability in sensitized C-nociceptors • Duloxetine (Cymbalta®) FDA approved 2004 for DNP pain – Major side effects: • Palpitations, fatigue, anxiety, hyperhydrosis, decreased libido, decreased appetite, vomiting, loose stools, erectile dysfunction, muscle cramps, weakness, cough, diaphoresis, nasopharyngitis – Precautions: hepatic dysfunction, renal insufficiency (require dose adjustments), alcohol abuse, concomitant use of tramadol – Other Benefits: Improvement of depression – Monitor: blood pressure Selective Serotonin & Norepinephrine Reuptake Inhibitor (SSNRI) • Venlafaxine (Effexor®, Effexor XR®) FDA approval 1993; “off label” use for DPN pain – Major side effects: • Nausea, vomiting, headache, asthenia, somnolence, dizziness, blurred vision, hypertension, sinus tachycardia, anorexia, insomnia, constipation, nervousness, weight loss, xerostomia, weakness, tremor, neck pain, diaphoresis, impotence – Precautions: • concomitant use of tramadol, cardiac disease, withdrawal syndrome with abrupt discontinuation; dose adjustments for renal & hepatic impairment – Other Benefits: Improvement of depression – Monitor: blood pressure; LFT & serum creatinine Calcium Channel alpha2-delta Ligands • Mechanism of action: – Binds to the 2 subunit of the voltage-dependent calcium channel; reduce influx of Ca2+, less glutamate released from nerve endings – inhibit sustained high-frequency neuronal firing by blocking sodium channels after an action potential, reducing excitability in sensitized C fiber nociceptors • Not metabolized, few drug interactions Calcium Channel alpha2-delta Ligands • Gabapentin (Neurontin®) FDA approved 1994 – Pain Indications: 2002 – PHN, other painful neuropathies, & nerve-related pain – Major side effects: • Somnolance, ataxia, fatigue, nausea, vomiting, peripheral edema – Precautions: renal insufficiency; dosing in elderly (start low, go slow) – Other benefits: improved sleep disturbance, no clinically significant drug interactions – Monitoring: serum creatinine for renal impairment Calcium Channel alpha2-delta Ligands • Pregabalin (Lyrica®) FDA approval 2005 – Indications: DPN pain, PHN, fibromyalgia (2007) – Major side effects: • Drowsiness, dizziness, fatigue, nausea, sedation, peripheral edema, visual disturbance, ataxia, tremor, constipation, dry mouth – Precautions: renal insufficiency; dosing in elderly (start low, go slow) – Other benefits: improved sleep disturbance, improved anxiety, no clinically significant drug interactions – Monitoring: serum creatinine for renal impairment Lidocaine 5% Patch • FDA approved 1999 for local neuropathic pain syndromes • Mechanism of action: topical anesthetic; blocks the conduction of impulses & stabilizes neuronal membranes to sodium • • Apply patch to intact skin with no blisters to cover most of painful area • Use up to 3 patches once a day for up to 12 hours on and 12 hours off – Can be kept on 24 hours (Gammaitoni 2002) • Pain relief is individual and may take anywhere from 4 hours to 14 days according to clinical studies • Minimal system absorption • • Major side effects: local erythema, rash • Precautions: blood levels are minimal; however, avoid use in patients receiving oral Class I antiarrhythmic medications Prescribing Recommendations for First-Line Medications Medication Class Secondary Amine TCA Nortriptyline Desipramine SSRI Duloxetine Starting Dose Titration Maximum Dosage Duration of Adequate Trial 25mg at bedtime Increase by 25mg daily every 3-7 days as tolerated 150 mg daily or divided 4 time/day 6-8 weeks with at least 2 wks at MTD 30mg once daily Increase to 60mg once daily after 1 wk 120 mg or 60mg BID 4 weeks 37.5 mg daily or BID Increase by 75 mg each week 225mg daily 4-6 weeks 3600 mg daily (1200 mg TID; reduce if impaired renal function 3-8 weeks for titration plus 2 weeds at maximum dosage 600 mg daily (200mg TID or 300mg BID; reduce if renal impaired 4 weeks 3 patches daily for 1218 h 3 weeks Venlafenxine Calcium channel alpha2delta ligands Gabapentin 100-300mg at bedtime or 100-300mg TID Pregabalin 50 mg TID or 75 mg BID Topical Lidocaine 5% Maximum of 3 patches daily for a maximum of 12 h Onset: 2 weeks Increase by 300 mg daily every 1-7 days Onset: more rapid (starting dose is efficacious) Increase to 300 mg daily after 3-7 days, then by 150 mg every 3-7 days as tolerated None needed Pharmacological Treatment/Management Second-Line Medications • Second-line medications: (Grade A recommendations) • Opioid analgesics • Tramadol Treatment of chronic NP with opioid agonists should be generally be reserved for patients who have failed to respond to or cannot tolerate the first-line medications alone or in combination. Tramadol • Mechanism of action: weak mu-opioid agonist & also inhibits the reuptake of norepinephrine and sertonin • Major side effects: somnolence, dizziness, nausea, weakness, dyspepsia, orthostatic hypotension, restlessness, seizures, respiratory depression (not completely reversible with naloxone), serotonin syndrome; abuse potential, but not scheduled • Precautions: history of substance abuse, suicide risk, seizure disorder, concomitant use of SSRI, SSNRI, TCA Tramadol (continued) • Slow titration: increase by 50mg PO every 3 days • • • • Onset: 1 hour Peak: 2-3 hours Duration: approximately 6 hours Steady-state: 2 days • High tissue affinity w/ minimal protein binding • Daily dose not to exceed: 400mg; 300mg for elderly Tapentadol (NuCynta®) • • • • Newer than Tramadol Stronger µ opioid agonist Norepinephrine reuptake inhibitor 50-100 mg PO similar in efficacy to oxycodone 10-15 mg • Schedule II • Cost can be an issue Prod Info tapentadol immediate release oral tablets, 2008 Prescribing Recommendations for Second-Line Medications Medication Class Opioids agonists Morpine, oxycodone, methadone Tramadol Short-acting & Extended Release Formulations Starting Dose Titration Maximum Dosage Duration of Adequate Trial 10-15 mg morphine equivalent every 3-4 hours as needed After 1-2 weeks, convert total daily dosage to long-acting opioid analgesic & continue short-acting medication as needed No maximum dosage with careful titration; consider evaluation by pain specialist at relatively high dosages (100180mg morphine equivalent daily) 4-6 weeks 50 mg once or twice daily Increase by 50-100 mg daily in divided doses every 3-7 days as tolerated 400 mg daily (100mg four times daily; in patients older than 65 years, 300 mg daily 4 weeks ER: 100, 200, 300 mg doses once daily Lower starting doses & slower titration in geriatric patients ER: Increase the dose by 100 mg every 3-4 days Mutimodal Pain Management Benefits • Multiple complex mechanisms may require different medications with different MOA • Additive or synergistic analgesia • Lower doses of individual agents may be used to decrease adverse side effects & provide opioid-sparing effects Interventional Techniques • Intrathecal implanted pumps; spinal cord stimulators • Nerve blocks – Well-localized pain – celiac plexus block for abdominal pain due to pancreatic cancer • Vertebroplasty – Stabilize vertebral body weakened by tumor • Lesioning of nerves, roots, plexus, spinal cord – Reserved for small number of individuals who do not obtain relief with any previous therapies Anticancer Therapies • Radiation therapy – Bone metastases & metastatic lesions (i.e. brain, spinal cord compression, obstruction) • Chemotherapy • Bisphosphonates – (pamidronate (Aredia) and zolendronic acid (Zometa) • Octreotide: malignant bowel obstruction, carcinoid syndrome • Surgery – stents, stabile bony structures -SCC Radiation for Bone Metastases • 40% of radiation is given for the goal of palliation of symptoms • External beam radiation to specific painful site • Intravenous systemic radioisotope therapy: – Phosphoruous-32 – Metastron (Stontium-89) – Quadramet (Samarium Sm-153 lexidronam) Nonpharmacological Strategies • Physical – Superficial Heat/Cold Therapy – Massage – Repositioning/bracing – Transcutaneous Electrical Wave Stimulation (TENS) • Cognitive – Distraction • Music, Humor, Activity – – – – – – Relaxation, Guided Imagery Expressive arts/music Biofeedback Education Support groups Spiritual counseling/prayer/meditation Pain Management at End of Life • Simplify medication regimen • If patient unable to swallow, consider alternate routes • If liver and renal dysfunction, drug clearance impaired; may need to reduce dose • Consult other team members – social work, chaplains, etc • Support family and other caregivers Palliative Sedation at End of Life • When all available treatment options have been exhausted and pain persists, may employ palliative sedation • Agents used include midazolam, propofol, barbiturates, and others • Requires consent of patient and family • Education is key: this is not euthanasia or assisted suicide Intractable Pain: Principle of Double Effect Basic Rules: 1. The treatment (ex. high dose opioid) is the only means to meet the end desired (pain relief) 2. The physician must intend only the good effect – relief of pain 3. The good effect must outweigh any unintended bad effect 4. The bad effect (possible earlier death) should not be the means to the good effect (pain relief). Monitoring Outcomes of Pain Relief Plan • Analgesia (presence or absence of satisfactory pain relief ) • Activities of daily living (improved function) • Adverse side effects or toxicities (acceptable or unacceptable) • Evidence of Aberrant behavior (are potential signs of inappropriate use of opioids present) • Achievement of goals for pain management (are goals met or need modification) Passik, S. et al, (2002); Curtiss, C. P. (2010) Patient/Family Education • Dispel & clarify any misconceptions/ attitudes/fears toward pain medications • Pain medications, dose, frequency & schedule • Expected side effects & their management • Safety issues • When to notify MD/RN Principles of Cancer Pain Management • • • • • • Consider variety of cancer pain syndromes Conduct thorough pain assessment Ascertain patient’s and family’s goals of care Incorporate multimodal therapies Prevent or rapidly treat adverse effects Reassess frequently and change therapies if needed • Address existential distress • Educate patients, families, other caregivers