Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
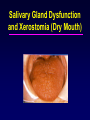
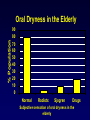
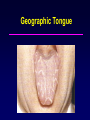
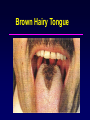
DIAGNOSIS AND MANAGEMENT OF XEROSTOMIA IN THE ELDERLY PATIENT Salivary Gland Dysfunction and Xerostomia (Dry Mouth) XEROSTOMIA • Xerostomia (dry mouth) is defined as a subjective complaint of dry mouth that may result from a decrease in the production of saliva. XEROSTOMIA • It affects 17-29% of samples populations based on self-reports or measurements of salivary flow rates. • More prevalent in women. • Can cause significant morbidity and a reduction in a patient’s perception of quality of life. SALIVA • It keeps the teeth healthy by providing a lubricant, calcium and a buffer. • It also helps to maintain the health of the gums, oral tissues (mucosa) and throat. • It also plays a role in the control of bacteria in the mouth. • It helps to cleanse the mouth of food and debris. • It provides minerals such as calcium, fluoride, and phosphorus. • It helps in swallowing and digesting food. • Lack of saliva will make the mouth more prone to disease and infection. • Lead to a burning feeling. % Population Oral Dryness in the Elderly 90 80 70 60 50 40 30 20 10 0 Normal Radiotx Sjogren Drugs Subjective sensation of oral dryness in the elderly ml / min Flow Rate of Saliva 0.5 0.4 0.3 0.2 0.1 0.0 unstimulated stimulated 20-39 yr 40-59 yr Age > 60 yr Antimicrobial Factors in Human Whole Saliva Non-immunoglobulin Factors Lysozyme Lactoferrin Salivary peroxidase SCNH2O2 Origin Salivary glands, crevicular fluid (PMNs) Salivary glands, crevicular fluid (PMNs) Salivary glands Salivary glands, crevicular fluid Salivary glands, crevicular fluid (PMNs), bacterial and yeast cells Myeloperoxidase Crevicular fluid (PMNs) ClSalivary glands, crevicular fluid Agglutinins, aggregating proteins Salivary glands Histidine-rich polypeptides Salivary glands Proline-rich proteins Salivary glands Immunoglobulin Factors Secretory IgA IgA, IgG, IgM Salivary glands Crevicular fluid • Ionizing radiation can injure the major and minor salivary glands which may lead to atrophy of the secretory components and results in varying degrees of temporary or permanent xerostomia. • Toxic substanaces in chemotherapeutic agents. • Diabetes mellitus: Patients with poor glycemic control, are more likely to complain of xerostomia and may have decreased salivary flow. Dry Mouth With Strawberry Tongue Severe Dry Mouth (Strawberry Tongue) Other Conditions • Anxiety or Depression • HIV • Diabetes, Type 1 or 2 • AIDS • Primary Biliary Cirrhosis • Bone Marrow Transplantation • Vasculitis • Graft-vs.-Host Disease • Chronic Active Hepatitis • Renal Dialysis Salivary Gland Dysfunction and Xerostomia • Clinical Appearance: • Oral mucosa appears dry, pale, or atrophic. • Tongue may be devoid of papillae with fissured and inflamed appearance. • New and recurrent dental caries. • Difficulty with chewing, swallowing, and tasting may occur. • Fungal infections are common. Pale Fisured Tongue Due To Severe Dry Mouth Moderate Xerostomia Warning Signs in Xerostomia 1. 2. 3. Dry, burning mouth and throat Dry, cracking lips, especially in the corners. The cracks may be tender and/or bleed Problems with denture wearing 4. Problems eating and swallowing food 5. Difficulty with speech due to mouth soreness. 6. Increased caries and periodontal disease Diagnosis of Xerostomia • It has been estimated that a 50% reduction in salivary secretion needs to occur before the xerostomia becomes apparent. • An affirmative response to at least one of the five following questions about symptoms has been shown to correlate with a decrease in salivary flow: 1. Does your mouth usually feel dry? 2. Does your mouth feel dry when eating a meal? 3. Do you have difficulty swallowing dry food? 4. Do you sip liquids to aid in swallowing dry food? • 5. Is the amount of saliva in your mouth too little most of the time, or don’t you notice it? When unstimulated salivary flow is less than 0.12 to 0.16 ml/minute, a diagnosis of hypofunction is established. MANAGEMENT • The general approach to treating patients with hyposalivation and xerostomia is directed at palliative treatment for the relief of symptoms and prevention of oral complications: • Consult with physician to decrease drug dose, alter drug dosages, or substitute one xerostomic medication for a similar-acting drug with fewer salivary side effects. • Symptomatic Treatments: • Sip water frequently all day long • Let ice melt in the mouth • Restrict caffeine intake • Avoid mouth rinses containing alcohol • Humidify sleeping area • Coat lips with lubricant. • Coat the lips with a petroleum jelly like Vaseline, Blistex, or lanolin. • Maintain good oral hygiene. Floss daily. • Brush at least twice a day. • Use toothpaste with fluoride and alcohol free (e.g. Biotene toothpaste). • Avoid Tobacco use, spicy, salty, and highly acidic foods that irritate the mouth. Saliva Substitutes: Rx: Sodium carboxymethyl cellulose* 0.5% aqueous solution [OTC] Disp:8 fl. Oz. Sig: Use as a rinse as frequently as needed. *Generic carboxymethyl cellulose solutions may be prepared by a pharmacist. Commercial Salivary Substitute • Commercial oral moisturizing gels (OTC) includes: • OralBalance. • XERO-Lube • Salivart • Moi-Stir Orex • Optimoist Commercial Oral Moisturizing Gels [OTC]: Laclede Oral Balance Oral Balance Ingredients •Polyglycerylmethacrylate (moisturizing agent) •Lactoperoxidase (antibacterial) •Glucose Oxidase (antibacterial) •Lysozyme (antibacterial) Saliva Stimulants: The use of sugar free gum, lemon drops or mints are conservative methods to temporarily stimulate salivary flow in patients with medication xerostomia or with salivary gland dysfunction. Rx: Biotine chewing gum [OTC] Disp: 1 package Sig: Chew as needed. Due to problems of abrasion of the mucosa under the denture and potential adhesion of the gum to the denture, use caution if the patient has removable dentures. Rx: Pilocarpine HCl (Salagen) Tablets 5 mg Disp: 21 tablets Sig: Take 1 tablet tid 1/2 hour prior to meals. Dose may be titrated to 2 tablets tid. Some authors recommend using 1 tablet of pilocarpine 4-5 times daily. Rx: Pilocarpine HCL solution 1 mg/ml Disp: 100 ml Sig: Take 1 teaspoonful tid. Pilocarpin HCl • May need 2-3 months to determine effectiveness. • Side effects include sweating and diarrhea. • Avoid in patients with narrow angle glaucoma, severe asthma, pulmonary diseases. Rx: Cevimeline (Evoxac) Capsules 30 mg Disp: 21 tablets Sig: Take 1 tablet tid. Rx: Bethanechol (Urecholine) tablets 25 mg Disp: 30 tablets Sig: Take 1 tablet up to 5 times daily. Conditions Affecting the Tongue Conditions Affecting the Tongue • • • • • Geographic tongue Hairy tongue Fissured tongue Varices Vitamin deficiencies Benign Migratory Glossitis (Geographic tongue) • Etiology: • Unknown • May be associated with psoriasis and Reiter’s syndrome. • Appearances: • Changing pattern of erythematous patches on the tongue dorsum caused by atrophy of the filiform papillae. Geographic Tongue Hairy Tongue • Etiology: • • • • • Antibiotics Tobacco Chlorhexidine Food debris Oral candidiasis Black/Brown Hairy Tongue Brown Hairy Tongue Hairy Tongue • Treatment: • Proper oral hygiene and tongue brushing. • If a fungal infection is suspected, perform a fungal culture and use topical antifungal. Fissured Tongue • Etiology: • Unknown • Appearance: • Numerous small furrows and fissures on the dorsum of the tongue. May be attributed to trauma, vitamin deficiencies, salivary gland dysfunction. Nutritional Deficiencies • Etiology • Vitamin B1, B2, B6, B12 and folic acid deficiency. • Appearance • Loss of filiform papillae produce a painful erythematous and granular appearing tongue. • Eventually papillae atrophy leaving a smooth/bald tongue.