Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
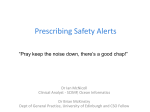
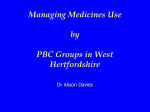
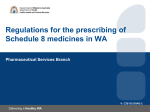
Andrew Barker Clinical Director Pharmacy & Medicines Management [email protected] The DBH experience with the JAC e-prescribing module Electronic Prescribing • Description of the system • Why did we want electronic prescribing? • The DBH Project • • • • History Where we are now? What have we learned? What next? Hospital electronic prescribing and administration recording etc. PAS WARDS PHARMACY OUT-PATIENTS ‘HOSPITAL EPR’ National spine The System • We are using JAC’s prescribing software which incorporates the Multilex Drug Data File from First DataBank Europe to provide decision support warnings for allergies, interactions and duplicate therapy. • In addition to prescribing, the system also provides ‘real time’ electronic recording of medicines administration, clinical pharmacy and medicines management activities. • It is fully integrated with Pharmacy stock control to allow the automated ordering of medicines. Why – to manage clinical risk • 5 - 6 % of hospital admissions result in an adverse event resulting from the use of medicines (Vincent et al, BMJ 2001 & Bates et al JAMA 1995) • Outcomes (Bates et al JAMA 1995) • Fatal 1% • Life threatening 12% Why – to manage clinical risk • Overall 28% of these adverse events are preventable • 42% of those classified as fatal, life threatening or serious were preventable • The following were the main contributory factors to preventable adverse events • Prescribing errors 62% • Administration errors 34% • Dispensing errors 4% Why – to manage clinical risk • Prescribing errors occur at a rate of 3 - 4 per 1000 items prescribed (Leaser et al JAMA 1990 &1997) • Common causal factors were: • Lack of knowledge or application of knowledge about the medicine 30.0% about the patient 29.2% • Calculations 17.5% • Nomenclature 23.4% Why – to manage clinical risk Introduction of electronic prescribing, and associated on-line decision support, can reduce serious adverse drug events by 55% From 10.7 to 4.86 per 1000 patient days (Bates et al JAMA 1988) Why - other benefits • Electronic patient records • Improved communication with primary care • Improved operational efficiency The DBH JAC Project • Initial single ward evaluation (2002 to 2003) • Pilot implementation Montagu Hospital (2003 to 2005) • 2 acute medical wards & 2 rehabilitation wards • Decision support was added to the system in October 2004 • First Operational Implementation Bassetlaw Hospital (November 2005 to 2007) • Medical Unit (6 wards including Acute Admissions Unit and CCU) • Full Trust Implementation agreed 2007/8 The DBH JAC Project • Current position • Live on all three sites • Full system on 20 wards – 11 Medical (including CCU, Renal, Acute & Rehab.) – 8 surgical (including Gen Surg, Ortho & Gynae) • Discharge only on 12 wards • May 2005 • 200 doctors prescribed 24,048 Medicines for 1,537 patients • 329 nurses recorded 144,290 administrations What have we learned? How does electronic prescribing reduce clinical risk? • Unambiguous prescriptions & administration records How does electronic prescribing reduce clinical risk? • Unambiguous prescriptions & administration records • Decision support – Product selection Formulary, protocols, (pathways,) etc. – – – – – Route, dose and frequency defaulting Allergy checking Drug interactions Therapeutic duplication (Max/min dose checking) Audit of Decision Support Warnings 2 month audit on two acute medical wards Patients with electronic prescriptions Individual lines prescribed Decision support warnings issued – Drug interactions: – Allergies – Duplicate therapy: 1,081 33 1,405 387 7,106 2,549 Outcomes of Warnings Audit of Decision Support Warnings Outcomes of warnings: • Heeded • Proceed –Alternative route/PRN product –Intended duplication –Benefit outweighs risk –Patient already stabilised on drugs –Not clinically significant 9.1% 4.3% 45.2% 14.9% 20.1% 6.4% 90.9% Audit of Decision Support Warnings • Further analysis: repeated warnings • Of 2,549 warnings issued 1,582 (62.1%) were repeated warnings • If repeated warnings are excluded then in the region of 20% first warnings were heeded Audit of Decision Support Warnings • The bottom line • On 74 occasions (1 in 97 orders) the prescriber did not complete their initial prescribing intention Patient Outcomes ? Introduction of electronic prescribing, and associated on-line decision support, can reduce serious adverse drug events by 55% From 10.7 to 4.86 per 1,000 patient days (Bates et al JAMA 1998) Audit to determine the effect of electronic prescribing and decision support on potential adverse drug events (Barker & Kay, Hospital pharmacist; 207, 14: 225) Independent review of in-patient prescriptions on two acute medical wards before and after the introduction of electronic prescribing with decision support Patients Items prescribed Before 94 702 After 95 706 RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing 12 10 8 6 4 2 0 Before After RESULTS Potential ADE by severity per 100 items prescribed before and after the introduction of electronic prescribing 10 8 Before 6 After 4 2 0 Minor Moderate Major RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing by cause of potential ADE Monitoring required Administration Medication Selection Additional Therapy 0 1 Before 2 After 3 4 RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing by cause of potential ADE Medication withheld -100% 0 1 2 Before After 3 4 RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing by cause of potential ADE Dose Selection -88% 0 1 2 Before After 3 4 RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing by cause of potential ADE Unnecessary Therapy -55% 0 1 2 Before After 3 4 RESULTS Potential ADE per 100 items prescribed before and after the introduction of electronic prescribing by cause of potential ADE Medication Selection +74% 0 1 2 Before After 3 4 Other Advantages • EPR, NHSRS etc • Could make all medicines use information (prescribing, dispensing and administration) available as an electronic record – but not yet • Improved communication with Primary Care DISCHARGE LETTER Date: 18-Jul-2007 @ 11:12 Page 1 of 2 Demographics, Ward & Consultant Allergy etc.status Patient: MARGUERITE HOLT NHS No.: 4344829581 Address: 62 WESTMORLAND HOUSE,CUMBERLAND CL,BIRCOTES,DONCASTER S YOR,DN11 8BY Ward: C3 WARD DOB: 20/09/1919 Consultant: Dr M (MM2) Muthiah Hospital: Bassetlaw General Hospital Known drug allergies: SALICYLATES Drug Discharge prescription Dose Route Frequency BUPRENORPHINE MATRIX 35 micrograms released per hour Patches 1 Patch TRANSDERM every 72 hours, AL FERROUS SULPHATE 200 mg Tablets 200 mg ORAL FOLIC ACID 5 mg Tablets 5 mg ORAL GABAPENTIN 300 mg Capsules 300 mg LANSOPRAZOLE 15 mg Capsules Admission details Diagnosis Details of hospital management Suggested further management Further information followup OPtofollow Discharging Doctor Days Supply GP to continue 28 Yes THREE times a day, 28 Yes in the MORNING, 28 Yes ORAL THREE times a day, 28 Yes 15 mg ORAL in the MORNING, 28 Yes PARACETAMOL 500 mg Tablets 1000 mg ORAL FOUR times a day, 28 Yes PREDNISOLONE 2.5 mg Enteric Coated Tablets 2.5 mg ORAL in the MORNING, 28 Yes SOTALOL 80 mg Tablets 80 mg ORAL TWICE a day, 28 Yes , Pharmacist details Pharmacy Notes REPRINT Hosp. No.: B481068 On ward *** Please complete in handwriting the controlled drug prescription(s) on the following sheet(s) *** *** Prescription not verified by hospital pharmacist *** Pharmacy notes: Date admitted: 11/07/2007 (Emergency Admission - DIARRHEA) Date discharged: 17/07/2007 Address discharged to: Home Diagnoses: DIARRHEA Relevant aspects of management in hospital ADMITTED WITH DIARRHEA. INFLAMMATORY MARKERS WERE WITHIN NORMAL LIMITS. TREATED SYMPTOMATICALLY. STOOL CULTURES WERE NEGATIVE. BEING DISCHARGED AND WILL FOLLOWUP WITH GP. Further management suggested: Further information to follow: No further information to follow Out-patient appointment arranged: None Discharging doctor: DR M ALZOUEBI, SENIOR HOUSE OFFICER Bleep: 3124 DISCHARGE LETTER Date: 18-Jul-2007 @ 11:12 Page 1 of 2 Patient: Hosp. No.: Address: NHS No.: Ward: DOB: Hospital: Consultant: REPRINT Known drug allergies: SALICYLATES Drug Dose Route Frequency Medication started during admission Medication started with reasons Drug Reason Medication discontinued or changed during admission Drug Medication changed or discontinued with reasons Reason , Pharmacy notes: Date admitted: Date discharged: Address discharged to: Diagnoses: Relevant aspects of management in hospital Further management suggested: Further information to follow: Out-patient appointment arranged: Discharging doctor: Bleep: Days Supply GP to continue Other Advantages • EPR, ICRS, NHSRS • Makes all medicines use information (prescribing, dispensing and administration) available as an electronic record • Communication with Primary Care • Audit • Massive potential – but not yet fully realised Operational benefit • Medical staff – Compliance with Trust Policy for writing prescriptions from 37% to 96% – Improvement in accuracy of transcription from inpatient to discharge prescription from 46% to 93% Operational benefit • Nursing staff – – – – Work-load prioritisation Date/time stamps Medication round times Compliance with Trust policy on recording administration from 65% to 100% • Pharmacy – work-load prioritisation – stock control/ordering – financial information Other issues • Cultural issues • • • • Doctors Nurses Pharmacy staff Medical records etc. • Hardware & infrastructure Peripheral hardware Other issues • Cultural issues • • • • Doctors Nurses Pharmacy staff Medical records etc. • Hardware & infrastructure • Software Other Issues • Training • Clinical Governance • Validation • Security • Resilience • Finance/affordability Prescribing Administration BLOGGS, JOE KENT, CLARK SMITH, JOHN