Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
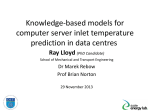
What’s on the horizon? Peter Sandercock ESC Lisbon 23rd May 2012 Outline • What are the key questions now? • What RANDOMISED trials are addressing them? • When will we see the results? • Focus on larger phase III trials Key questions • Clinical patient selection? • Advanced imaging selection? • Any other IV drug clearly better than rt-PA? • Do lower dose IV treatments have a better risk/benefit ratio? • Is IA drug +/- clot pulling really better than IV? Simple clinical selection criteria • • • • • • • • Time from onset Age Clinical severity NIHSS, SSS, OCSP Pre-treatment brain scan BP Glucose Background anti-platelet/anticoagulant Etc… Must combine baseline characteristics • Patients who present early have higher NIHSS • Patients presenting later are more likely to show ischaemic change on CT or MR IST-3 update. Trials 2012 Stroke Thrombolysis Trialists Collaboration (STTC) • Individual patient data meta-analysis of all i.v. rt-PA RCT’s, update of 2010 pooled analysis • Protocol and analysis plan in final draft • Meeting of Steering Group 24th May 2012 • Plan to meet mid 2013 to review preliminary analyses STTC analyses - draft plan Primary analyses • after what treatment delay is benefit lost or does harm begin, • do age or stroke severity modify the proportional effect of rt-PA on stroke outcome? Secondary • Effect of treatment allocation on: death within 90 days, SICH, Symptomatic ischaemic brain oedema • Effect modification by baseline characteristics Ongoing Phase 3 trials iv thrombolysis vs control rt-PA • TESPI (> 80 years < 3hrs) 162/600 • *EXTEND, MR mismatch criteria 3 – 9h • *ECASS 4, MR mismatch criteria 3 – 9h Desmoteplase • *DIAS 4. Vessel occlusion / stenosis on MRI or CTA 3-9 hrs *advanced imaging selection ENCHANTED: questions Compared to standard (0.9 mg/kg) rtPA, is low-dose (0.6 mg/kg) i.v. rtPA: – at least equivalent in clinical outcomes? – safer in terms of a lower risk of symptomatic intracerebral haemorrhage (sICH)? Compared to guideline BP control, does intensive BP control* – provide superior clinical outcomes – have a lower risk of sICH? *(<180-185 mmHg systolic target before initiation of rtPA), vs rapid intensive BP lowering (140-150 mmHg systolic target): • Primary outcome mRS at 90 days • Sample size ~5000 • 100+ sites, with emphasis on Asia ? China 20 centres ? ? Europe (UK, France,, Belgium, Germany, Austria, Italy, Portugal, Spain, Norway, Sweden, Finland Korea 10-15 centres ~30 centres Taiwan 10-15 centres India 15 centres SE Asia (Vietnam, South America (Chile, Brazil, Colombia, Peru) Thailand, Malaysia, Singapore) 10-15 centres ? ~20 centres Australia 14 centres IA/interventional • IMS-III • SYNTHESIS • EXTEND-IA • MR RESCUE • PISTE IMS-3 Design • Randomised trial of combined IV/IA approach vs standard IV t-PA • 900 subjects < 3hrs • NIHSS >/= 10, or NIHSS 8-9 with CTA evidence of ICA, M1 or basilar occlusion prior to initiation of IV rtPA • IA therapy includes choice of catheter/devices and IA t-PA Recruitment and Active Sites N = 631 (22/02/12) Update • stopped by the NINDS because of crossing a futility boundary at a predetermined DSMB review that included 587 patients. • the study had a very low likelihood of demonstrating the pre-specified, clinically significant difference in benefit between the treatment arms of the study. • The DSMB’s decision was based upon the primary outcome in the study, the Modified Rankin Score at 3 months, meeting the threshold for futility. • While enrollment was stopped because of futility, no serious safety concerns were identified Synthesis Investigators SYNTHESIS (n=362) Acute stroke Medical history-Physical Examination-NIHSS score Laboratory-ECG CT scan Verify neuroradiologist's availability Informed consent Randomization(0-4.5 h) Angio & IA rt-PA&devices IV rt-PA <6h < 4.5 h CT scan on day 4 (± 2) Monitoring for 7 days-Adverse events 90 days blind efficacy evaluation-Telephone modified Rankin scale When? • STTC analyses – 2013/2014 • SYNTHESIS and IMS – III – 2013 • The rest – it’s up to you to support these trials! Acknowledgements: thanks to Jo Broderick, Alfonso Ciccone and Craig Anderson for slides