Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
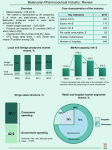
Reform of the Lithuanian health system Martynas Marcinkevičius Advisor to the Minister of Health Dynamics of Compulsory Health Insurance Fund’s Budget and Gross Domestic Product (GDP) from 1998 to 2011 111,5 GDP, bil. LTL 98,1 CHIF budget, bil LTL 92,0 95,7 98,8 82,8 Percentage of GDP 72,1 62,7 44,7 43,7 45,7 4,3 48,6 52,1 4,2 4,0 57,0 3,8 3,7 3,7 3,8 4,0 4,1 4,1 4,1 4,8 4,2 4,58 4,46 4,0 1,94 1,83 1,83 1,87 1,92 2,1 2,39 2,89 3,41 4,0 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 4,3 4,2 2011 plan Number of beds and hospitals Lovų skaičius 1000 gyv. Ligoninių skaičius 100 000 gyv. 9 8 5 7 4 6 5 3 4 2 3 2 1 1 Šaltinis: Europos sveikatos duomenų bazė. http://www.euro.who.int/HFADB ES tij a Li et ES uv na a uj ų na r ių Es ėn ija Kr oa tij a Ve ng rij a Sl ov ak ija M ak ed on ija Če ki ja La tv ija nd ija Sl ov Ol a Šaltinis: Europos sveikatos duomenų bazė. http://www.euro.who.int/HFADB Da No nija rv e Sl gija ov ėn Ol ija an di j Le a nk i Kr ja oa tij a Es tij Sl ov a ak Ve ija ng rij a La tv ija Če ki Li ja et uv a 0 0 Health care system reforms. Funding Transition from the budget-based to the insurance-based system Patient fund institution (1997) All health care institutions became public institutions (1997) (according to the pattern of state limited companies) Health care system reforms. Health care institution Introduction of General Practitioner institutions (nearly half of them are private) Three stages of hospital reduction (2002,2004,2010-2011) Expansion of the network of nursing hospitals Reorganisation of the hospital network in 2010-2011 Reorganisation of hospitals. Goals Goals Improving the quality of treatment and patient security Strengthening the primary care and outpatient levels by transposing funds and professionals from the in-patient level Efficient use of existing resources Trends Restructuring of health care services (RRR reform) Optimisation of the network of health care institutions Region and district hospitals Region hospitals must meet two basic criteria: more than 1,100 major surgeries and more than 300 childbirths District hospitals With surgery and obstetrics (if tending to over 300 childbirths) With surgery (if performing over 660 major surgeries) Without surgery and obstetrics Optimisation of the hospital network and services (ongoing) The number of health care institutions (legal entities) decreased by 11 More than 70 different services (surgery, obstetrics, neurology, psychiatry, cardiology, etc.) are no longer bought from different hospitals Optimisation of the hospital network Principles: Integrating mono-profile hospitals into multi-profile ones Merge geographically proximate institutions Network: 2 University research and treatment centres 8 National level hospitals 8 Regional level hospitals 39 District level hospitals (including 10 with surgery and obstetrics unit and 12 with surgery unit) Localisation of personal health care institutions by category Skuodas Mažeikiai N. Akmenė Joniškis Kuršėnai Kretinga Klaipėda Plungė Telšiai Šiauliai Biržai Pasvalys Pakruojis Panevėžys Gargždai Rokiškis Kupiškis Radviliškis Zarasai Kelmė Šilalė Utena Kėdainiai Šilutė Tauragė Visaginas Anykščiai Raseiniai Molėtai Ukmergė Jurbarkas Kaunas Jonava Kaišiadorys Šakiai Kazlų Rūda Marijampolė Vilkaviškis Region hospitals Švenčionys Širvintos Vilnius Elektrėnai Trakai Prienai Alytus Kalvarija Šalčininkai District hospitals Lazdijai Varėna Druskininkai Municipalities without multi-profile hospitals Ignalina New Pharmaceutical Policy in Lithuania Goals of the Plan Stop growth in expenditures of the Compulsory Health Insurance Fund on reimbursable medicinal products Reduce public expenditures on all medicinal products (reimbursable/non reimbursable) 28 measures of the Plan Involve all players of the pharmaceutical market: manufacturers of ethic/generic medicinal products, wholesalers, pharmacy chains, individual pharmacies, medical doctors and competent authorities Means to save expenditures of the Compulsory Health Insurance Fund (CHIF) budget Options for clustering medicinal products in the Price-list 1 producer original Expenditures of the CHIF on the reimbursement of medicinal products for the year 2008 352.469.704 Clustering medicinal products of the same therapeutic action for the basic price 15 mln LTL Clustering medicinal products of the same active substance for the basic price 3 mln LTL Price-cutting of the generic medicinal products Valid at the moment (expenditure reduction 10 mln LTL in year 2009) 1 producer generic 12.856.132 2 producers 93.478.775 5 mln LTL 3 producers 29.814.468 3 mln LTL 4 producers 147.433.243 Total 636.052.322 Reimbursement of complex medicinal products according to the lowest price of the component 5 mln LTL Signing agreements on the limitation of expenditures Protects from the uncontrolled rise in expenditure 5-10 mln LTL The unification of retail prices and copayments 5-10 mln LTL Predictive saving for the calendar year ~ 50-60 mln LTL Means to reduce patient expenditures on the purchasing of the medicinal product Setting maximum mark-ups for prescription medicinal products The unification of retail prices and copayments Obligation to present visual information about the prices and other means to strengthen control over the sales of medicinal products Obligation of doctors to prescribe the exact quantity of medicinal product Obligation if doctors regarding rational pharmacotherapy 40-60 mln LTL 20-40 mln LTL 20-30 mln LTL 5 mln LTL 5-10 mln LTL Predictive saving for the calendar year ~ 90-145 mln LTL Compulsory Health Insurance budget’s expenditure for reimbursed pharmaceutical and medical devices for ambulatory care, million euros 300 217 201 200 186 170 147 127 100 93 94 93 103 89 93 89 125 94 105 99 110 107 122 139 155 179 198 202 189 2006 2007 2008 2009 2010 0 1998 1999 2000 2001 2002 2003 CHIFB Expenditure for pharmaceutical and MD 16 2004 2005 CHIF budget for pharmaceutical and MD 2005/2010 ratio between reimbursable amount for medicinal products and MA and the patient mark-up amount (mln LTL) as well as dynamics of patient mark-up +20.9 % 1000,0 +20,7 % 205,7 800,0 213.8 165,4 170,1 700,0 mln. Lt -22.6% +21,4 % 900,0 600,0 +3.9 % 141,1 116,9 500,0 400,0 300,0 480,4 538,4 624,4 683,2 696,2 653,3 200,0 100,0 0,0 2005 2006 Reimbursed amount, Lt 2007 2008 2009 Patient mark-up amount, Lt 2010 Changes in prices for medicinal products in 2010 After introducing regulation of prices for non-reimbursable medicines, prices for medicines decreased by around 10% (by approximately 30 mln LTL). The average mark-up on prescription for reimbursable medicines decreased by as much as 22.6%, and patients saved around 49 mln LTL. For the first time since 2002, a reduction in expenditure of the Compulsory Health Insurance Fund budget on reimbursable medicinal products has been recorded. In 2010 expenditure on medicines was by 6%, or 43 mln LTL, lower than in 2009. In 2011, the decreasing trend in prices and patient mark-ups for medicinal products remains. Savings will enable starting to reimburse new modern medicines and to include new diseases and indications. Nearest plans and goals Introduction of voluntary health insurance Correct payment service (DRG etc.) Quality assurance and measurement Introduction of e-health