Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
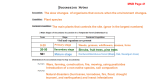
COMPARING ASSOCIATION RULES AND DECISION TREES FOR DISEASE PREDICTION Carlos Ordonez MOTIVATION Three main issues about mining association rules in medical datasets: 1. 2. 3. A significant fraction of association rules is irrelevant Most relevant rules with high quality metrics appear only at low support # of discovered rules becomes extremely large at low support Search constraints: Find only medically significant association rules Make search more efficient MOTIVATION Decision tree a well-known machine learning algorithm Association rules vs. Decision tree Accuracy Interpretability Applicability ASSOCIATION RULES Support Confidence Lift confidence( x y ) lift ( x y ) sup port ( x y ) sup port ( x) confidence( x y ) sup port ( y ) Lift quantifies the predictive power of x y Rules such that lift(xy) > 1 are interesting! CONSTRAINED ASSOCIATION RULES Transforming Medical Data Set Data must be transformed to binary dimensions Numeric attributes intervals, each interval is mapped to an item. Categorical attributes each categorical value is an item If an attribute has negation add that as an item Each item is corresponds to the presence or absence of one categorical value or one numeric interval CONSTRAINED ASSOCIATION RULES 1. Search Constraints Max itemset size (k) 2. Group 3. Reduces the combinatorial explosion of large itemsets and helps finding simple rules gi >0 Aj belongs to a group gi =0 Aj is not group-constrained at all This avoids finding trivial or redundant rules Antecedent/Consequent ci = 1 Ai is an antecedent ci = 2 Ai is a consequent Binned at 40(adult) and 60(old) Percentage of vessel narrowing LAD, LCX and RCA are binned at 70% and 50% LM is binned at 30% and 50% 9 heart regions ( 2 ranges with 0.2 as cutoff) Patients 655 attributes 25 Binned at 200 and 250 PARAMETERS k=4 Min support = 1% ≈ 7 Min confidence = 70% Min lift = 1.2 To get rules where there is stronger implication dependence between X and Y Rules with conf ≥ 90 and lift ≥ 2, with 2 or more items in the consequent were considered medically significant. HEALTHY ARTERIES 9,595 associations 771 rules DISEASED ARTERIES Several unneeded items were filtered out ( with values in lower (healthy) ranges) 10,218 associations 552 rules PREDICTIVE RULES FROM DECISION TREES CN4.5 using gain ratio CART similar results Threshold for the height of the tree to produce simple rules Percentage of patients (ls) Fraction of patients where the antecedent appears Confidence factor (cf) Focus on predicting LDA disease PREDICTIVE RULES FROM DECISION TREES 1. All measurements without binning as independent variables, numerical variables are automatically split Without any threshold on height: 181 node 90% accuracy height = 14 most rules more than 5 attributes except 5 rules, other involve less than 2% of the patients More than 80% of rules refer to less than 1% of patients Many rules involve attributes with missing information Many rules had the same variable being split several times Few rules with cf = 1 but splits included borderline cases and involves few patients PREDICTIVE RULES FROM DECISION TREES With threshold = 10 on height 83 nodes 77% accuracy Most rules have repeated attributes More than 5 attributes Perfusion cutoffs higher than 0.5 Low cf and involved less than 1% of the population With threshold = 3 on height 65% accuracy Simpler rules RELATED WORK PREDICTIVE RULES FROM DECISION TREES 2. Items (binary variables) as independent variables like association rules are used With threshold = 3 on height Most of the rules were much closer to the prediction requirements 10 nodes DISCUSSION Decision trees are not as powerful as association rules in this case Do not work well with combinations of several target variables Fail to identify many medically relevant combinations of independent numeric variable ranges and categorical values Tend to find complex and long rules, if the height is unlimited Find few predictive rules with reasonably sized (>1%) sets of patients in such cases Rules some times repeat the same attribute DISCUSSION - ALTERNATIVES build many decision trees with different independent attributes Create a family of small trees, each tree has a weight It’s error-prone, difficult to interpret, slow for higher # of attributes Each tree becomes similar to a small set of association rules Constraints for association rules can be adopted to decision trees (future work) DISCUSSION – DECISION TREE ADVANTAGES DT partitions the data set, ARs on the same target attributes may refer to overlap DT represents a predictive model of data set, ARs are disconnected among themselves DT is guaranteed to have at least 50% prediction accuracy and generally above 80% for binary target variables, ARs require trial and error to find the best threshold