Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
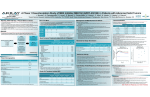
COMMONLY USED PSYCHOTROPIC DRUGS po = by mouth; prn = as needed; qd = 1x/day; bid = 2x/day; tid = 3x/day; qid = 4x/day; qod = every other day; qhs = at bedtime; qac = before meals; = on WalMart’s $4 Rx plan, however not all dosages may be covered NAME DOSE IMPORTANT CLINICAL INFORMATION Commonly used Antidepressants and Antianxiety Medications Start: 100mg bid titrating to 150 mg bid or tid SR or XL preparation is longer acting (bid dosing) Seizure risk ; Stimulating; not good for anxiety 20 – 60mg qam (Start: 20mg qam) Less GI distress than other SSRIs; No clinical CYP 450 interactions Duloxetine (Cymbalta) 20 – 30mg bid (Start: 20 mg bid) Side effect profile like SSRIs and venlafaxine Escitalopram (Lexapro) 10 – 20mg qam (Start: 10 mg qam) Less GI distress than other SSRIs; No clinical CYP 450 interactions 20 – 80mg qam (Start: 10 – 20mg qam) More stimulating than other SSRIs; Long half life prevents withdrawal Bupropion (Wellbutrin) Citalopram (Celexa) Fluoxetine (Prozac) Mirtazapine (Remeron) Paroxetine (Paxil) Sertraline (Zoloft) 30 – 45mg qhs (Start: 15mg qhs) Sedating and appetite promoting; Neutropenia risk (1 in 1000) 20 – 50mg qhs (Start: 10 – 20mg qhs) Anticholinergic, sedating, withdrawal syndrome 50 – 200mg qam (Start: 25 – 50mg qam ) No clinical CYP 450 interactions Trazodone (Desyrel) 50 – 150mg qhs for sleep (Start: 25mg qhs) Commonly used as sleep aid; Priapism risk Venlafaxine (Effexor) Start: 37.5 – 75mg bid with titration to 300 – 375mg daily XR preparation is longer acting (once daily dosing) Side effects like SSRIs; HTN and withdrawal risk Commonly used Antianxiety and Sleep (Hypnotic) Medications Alprazolam (Xanax) Start: 0.25mg – 0.5mg tid Indicated for panic disorder and anxiety; Equivalent dose: 0.5mg Start: 0.25 – 0.5mg bid with doses up to 1 – 4mg in panic disorder and up to 20mg divided bid for seizures Start: 2 – 10mg bid to qid with doses varying widely based on the reason for use Indicated for panic disorder and seizure disorder; Has been effective in mania Onset: intermediate; Elimination: 18 – 50 hrs; Equivalent dose: 0.25mg Many indications including anxiety, seizures, alcohol withdrawal, & muscle spasm Onset: fast; Elimination: 30 – 100 hrs; Equivalent dose: 5mg Oxazepam (Serax) Start: 10mg bid or tid for anxiety. Insomnia: start with 15 mg at bedtime. Indicated for alcohol withdrawal and anxiety; Equivalent dose: 15mg Lorazepam (Ativan) Anxiety: 2 – 3mg bid or tid Indicated for insomnia, anxiety, pre-anesthesia, and status epilepticus Safer in liver disease; Equivalent dose: 1mg Start: 1 – 2mg at bedtime titrated to 3mg Approved for long term use; no evidence of dependence over six month treatment Start: 5mg at bedtime titrated to 10mg Short half life of 2-3 hours. Clonazapam (Klonopin) Diazepam (Valium) Eszopiclone (Lunesta) Zolpidem (Ambien) Zaleplon (Sonata) Ramelteon (Rozerem) Start: 10mg titrated to 20mg Essentially like zolpidem; Has a very short half life of one hour. Start: 8mg at bedtime Melatonin receptor agonist; Appears safe for long term use in insomnia Commonly used Antimanic Medications (Mood Stabilizers) Lithium Valproic Acid Lamotrigine (Lamictal) Start: 150 – 300mg bid with doses up to 1200 – 1500mg daily based on renal function Start: 250mg bid with end dose of 1000 – 2000mg divided bid (max dose: 60mg/kg/day divided bid) Start: 25mg daily for two weeks then 50mg daily for two weeks with a final dose of 200 – 400mg once or divided. Black box warning: toxicity and the need to check levels; Level established (0.5 - 1.2 meq/L) Black box warning: hepatotoxicity, pancreatitis, and teratogenicity; Therapeutic levels (80-120mcg/mL) Black box warning due to rash. No therapeutic drug levels Commonly used Antipsychotic Medications Hyperprolactinemia common; Decanoate (injection) preparation available. Orally dissolvable tablet excellent for acute agitation Risperidone (Risperdal) Start: 0.5 – 1mg qhs or bid titrating to 4 – 6mg daily or bid Olanzapine (Zyprexa) Start: 5 – 10mg daily titrating to 15 – 30mg daily once or divided bid Sedation, weight gain, and metabolic complications are common. Quetiapine (Seroquel) Start: 20mg bid titrating to 400 – 600mg daily divided bid (max dose: 800mg) Very sedating with a low incidence of extrapyramidal side effects. Ziprasidone (Geodon) Aripiprazole (Abilify) Start: 20mg bid titrating to 40 – 80mg bid Black box warning for QT prolongation Start:10 – 15mg daily titrating to 15 – 30mg daily May have less metabolic complications than other atypicals Also has an indication for bipolar disorder Most effective antipsychotic for treatment refractory patients Agranulocytosis, orthostasis, tachycardia, weight gain, and drooling Classic typical, high potency neuroleptic. Causes Parkinsonian symptoms (EPS). Comes in an elixir and can be given PO, IM. Long acting (depot) form available. Clozapine (Clozaril) Start: 12.5 daily or bid titrating slowly to 300-450mg daily in divided doses (max dose: 900mg) Haloperidol (Haldol) Start: 0.5 to 5mg daily or bid titrating to 5- 20 mg daily Prazosin (Vasoflex ) Start: 1mg at bedtime (titrate slowly as needed to effect) Orthostatic hypertension– Patient should move slowly from resting to standing COMMONLY USED PSYCHOTROPIC DRUGS po = by mouth; prn = as needed; qd = 1x/day; bid = 2x/day; tid = 3x/day; qid = 4x/day; qod = every other day; qhs = at bedtime; qac = before meals; = on WalMart’s $4 Rx plan, however not all dosages may be covered NAME DOSE IMPORTANT CLINICAL INFORMATION Commonly used Antidepressants and Antianxiety Medications Start: 100mg bid titrating to 150 mg bid or tid SR or XL preparation is longer acting (bid dosing) Seizure risk ; Stimulating; not good for anxiety 20 – 60mg qam (Start: 20mg qam) Less GI distress than other SSRIs; No clinical CYP 450 interactions Duloxetine (Cymbalta) 20 – 30mg bid (Start: 20 mg bid) Side effect profile like SSRIs and venlafaxine Escitalopram (Lexapro) 10 – 20mg qam (Start: 10 mg qam) Less GI distress than other SSRIs; No clinical CYP 450 interactions 20 – 80mg qam (Start: 10 – 20mg qam) More stimulating than other SSRIs; Long half life prevents withdrawal Bupropion (Wellbutrin) Citalopram (Celexa) Fluoxetine (Prozac) Mirtazapine (Remeron) Paroxetine (Paxil) Sertraline (Zoloft) 30 – 45mg qhs (Start: 15mg qhs) Sedating and appetite promoting; Neutropenia risk (1 in 1000) 20 – 50mg qhs (Start: 10 – 20mg qhs) Anticholinergic, sedating, withdrawal syndrome 50 – 200mg qam (Start: 25 – 50mg qam ) No clinical CYP 450 interactions Trazodone (Desyrel) 50 – 150mg qhs for sleep (Start: 25mg qhs) Commonly used as sleep aid; Priapism risk Venlafaxine (Effexor) Start: 37.5 – 75mg bid with titration to 300 – 375mg daily XR preparation is longer acting (once daily dosing) Side effects like SSRIs; HTN and withdrawal risk Commonly used Antianxiety and Sleep (Hypnotic) Medications Alprazolam (Xanax) Start: 0.25mg – 0.5mg tid Indicated for panic disorder and anxiety; Equivalent dose: 0.5mg Start: 0.25 – 0.5mg bid with doses up to 1 – 4mg in panic disorder and up to 20mg divided bid for seizures Start: 2 – 10mg bid to qid with doses varying widely based on the reason for use Indicated for panic disorder and seizure disorder; Has been effective in mania Onset: intermediate; Elimination: 18 – 50 hrs; Equivalent dose: 0.25mg Many indications including anxiety, seizures, alcohol withdrawal, & muscle spasm Onset: fast; Elimination: 30 – 100 hrs; Equivalent dose: 5mg Oxazepam (Serax) Start: 10mg bid or tid for anxiety. Insomnia: start with 15 mg at bedtime. Indicated for alcohol withdrawal and anxiety; Equivalent dose: 15mg Lorazepam (Ativan) Anxiety: 2 – 3mg bid or tid Indicated for insomnia, anxiety, pre-anesthesia, and status epilepticus Safer in liver disease; Equivalent dose: 1mg Start: 1 – 2mg at bedtime titrated to 3mg Approved for long term use; no evidence of dependence over six month treatment Start: 5mg at bedtime titrated to 10mg Short half life of 2-3 hours. Clonazapam (Klonopin) Diazepam (Valium) Eszopiclone (Lunesta) Zolpidem (Ambien) Zaleplon (Sonata) Ramelteon (Rozerem) Start: 10mg titrated to 20mg Essentially like zolpidem; Has a very short half life of one hour. Start: 8mg at bedtime Melatonin receptor agonist; Appears safe for long term use in insomnia Commonly used Antimanic Medications (Mood Stabilizers) Lithium Valproic Acid Lamotrigine (Lamictal) Start: 150 – 300mg bid with doses up to 1200 – 1500mg daily based on renal function Start: 250mg bid with end dose of 1000 – 2000mg divided bid (max dose: 60mg/kg/day divided bid) Start: 25mg daily for two weeks then 50mg daily for two weeks with a final dose of 200 – 400mg once or divided. Black box warning: toxicity and the need to check levels; Level established (0.5 - 1.2 meq/L) Black box warning: hepatotoxicity, pancreatitis, and teratogenicity; Therapeutic levels (80-120mcg/mL) Black box warning due to rash. No therapeutic drug levels Commonly used Antipsychotic Medications Hyperprolactinemia common; Decanoate (injection) preparation available. Orally dissolvable tablet excellent for acute agitation Risperidone (Risperdal) Start: 0.5 – 1mg qhs or bid titrating to 4 – 6mg daily or bid Olanzapine (Zyprexa) Start: 5 – 10mg daily titrating to 15 – 30mg daily once or divided bid Sedation, weight gain, and metabolic complications are common. Quetiapine (Seroquel) Start: 20mg bid titrating to 400 – 600mg daily divided bid (max dose: 800mg) Very sedating with a low incidence of extrapyramidal side effects. Ziprasidone (Geodon) Aripiprazole (Abilify) Start: 20mg bid titrating to 40 – 80mg bid Black box warning for QT prolongation Start:10 – 15mg daily titrating to 15 – 30mg daily May have less metabolic complications than other atypicals Also has an indication for bipolar disorder Most effective antipsychotic for treatment refractory patients Agranulocytosis, orthostasis, tachycardia, weight gain, and drooling Classic typical, high potency neuroleptic. Causes Parkinsonian symptoms (EPS). Comes in an elixir and can be given PO, IM. Long acting (depot) form available. Clozapine (Clozaril) Start: 12.5 daily or bid titrating slowly to 300-450mg daily in divided doses (max dose: 900mg) Haloperidol (Haldol) Start: 0.5 to 5mg daily or bid titrating to 5- 20 mg daily Prazosin (Vasoflex ) Start: 1mg at bedtime (titrate slowly as needed to effect) Orthostatic hypertension– Patient should move slowly from resting to standing Provide d by Mental H ealth Infrastructure a nd Train ing (MHIT) Project an d REACH NOLA (w ww.reac hno la.org) MAXIMUM THERAPEUTIC DOSES (mg PER DAY) COMMONLY USED ANTIDEPRESSANTS OF (Medication "failures" are often due to inadequate dosing*) Bupropion (Wellbutrin) 450mg Citalopram (Celexa) 60mg Duloxetine (Cymbalta) 60mg Escitalopram (Lexapro) 30mg Fluoxetine (Prozac) 60mg Mirtazapine (Remeron) 60mg Paroxetine (Paxil) 60mg Sertraline (Zoloft) 200mg Venlafaxine (Effexor) 300mg *Treat at the maximum tolerated therapeutic dose for 6 to 8 weeks before switching. GOOD REASONS • • • • TO STOP A MEDICATION Intolerable side effects Dangerous interactions with other necessary medications It was never "indicated" to begin with (wrong diagnosis or wrong medicine for diagnosis) It has been at the maximum therapeutic dose for 6 to 8 weeks with no results Originally created by Alex Thompson, MD, MPH, MBA and Stephen Thielke, MD, MPH University of Washington MAXIMUM THERAPEUTIC DOSES (mg PER DAY) COMMONLY USED ANTIDEPRESSANTS OF (Medication "failures" are often due to inadequate dosing*) Bupropion (Wellbutrin) 450mg Citalopram (Celexa) 60mg Duloxetine (Cymbalta) 60mg Escitalopram (Lexapro) 30mg Fluoxetine (Prozac) 60mg Mirtazapine (Remeron) 60mg Paroxetine (Paxil) 60mg Sertraline (Zoloft) 200mg Venlafaxine (Effexor) 300mg *Treat at the maximum tolerated therapeutic dose for 6 to 8 weeks before switching. GOOD REASONS • • • • TO STOP A MEDICATION Intolerable side effects Dangerous interactions with other necessary medications It was never "indicated" to begin with (wrong diagnosis or wrong medicine for diagnosis) It has been at the maximum therapeutic dose for 6 to 8 weeks with no results Originally created by Alex Thompson, MD, MPH, MBA and Stephen Thielke, MD, MPH University of Washington Provide d by Mental H ealth Infrastructure a nd Train ing (MHIT) Project an d REACH NOLA (w ww.reac hno la.org)