Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
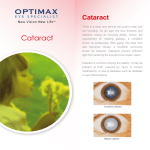
Inspiration, Persistence…Perfection: The Road to Modern Vision Correction In a closed operation room a sixty year old bow-tied doctor is bent curiously over a patient’s head, his mouth moving ever so slightly. With no high-tech equipment to assist him, the doctor is painstakingly careful as he uses a thin, pointed instrument to make an incision in the topmost portion of the patient’s eye, the cornea. After a successful incision, a pair of precision forceps is used to extract a small, clouded, almost opaque lens from the beneath the patients cornea. The doctor discards the troublesome lens and retrieves an acrylic lens, no thicker than a fingernail, to replace the just removed clouded lens. The process takes no longer than an hour, and the patient is carted off to recovery with their ability to see gratefully restored. The year was 1952 and Dr. Warren S. Reese is the surgeon in this story. An ophthalmologist at the Wills Eye Hospital in Philadelphia, Dr. Reese was the first American to successfully implant an acrylic intraocular lens into a cataract patient. Today, cataract removal is the most frequently performed surgery in the United States with a success rate of nearly 98% in all patients. The term cataract is of Latin origin meaning “a downpour of water.” This definition comes from the way a cataract is formed: fluid within the eye becomes trapped in the space between the clear outer lens, the cornea, and the black part of the eye that facilitates vision, the iris. Once the fluid has become trapped, it gels and forms a pseudo-lens, blocking light from entering the iris and thus causing reduced vision or even blindness is some patients. Cataract surgery has been in practice for over 2,000 years. Evidence for a primitive form of cataract surgery has been found in a Sanskrit manuscript dated 1 AD. The procedure described a technique termed “couching” in which a tool is used to push the affected lens out of the field of vision of the patient, it was thought that the clouded cataract lens would eventually disintegrate and vision would be fully restored. Of course, the majority of the time the cataract would return. It wasn’t until the 18th century that the cataract lens was physically removed. A French surgeon by the name of Jacques Daviel was the first to fully remove a cataract lens from a patient’s eye in 1750. The surgery required the doctor to make an incision in the patient’s eye without the luxury of anesthesia. Because of the discomfort, patients often rolled their eyes upward, causing difficulties for the surgeon and leading Daviel to state that “the extraction is only for skillful and experienced hands.” Many of the attempted cataract removals, either by Daviel or other surgeons, were failures due mostly to infection post-surgery or the inexperience of the surgeon. Because of these failures, cataract removal fell by the wayside and couching remained the preferred method for relieving patients of their cataracts until the 20th Century. With the advances of immobilizing and numbing medications the removal of cataracts once again became a feasible for ophthalmic surgeons. During World War II, the techniques for the removal of cataracts were perfected to the point that most surgeons thought no further improvement could be made to the procedure. That was until Dr. Harold Ridley, a British ophthalmologist, noticed that Perspex (a type of Plexiglas) does not cause reactions or infections when embedded into the human eye. This phenomenon was noticed during WWII when plane windshields, made from Perspex, would shatter and remnants would embed in the pilot’s eye. With this knowledge, Dr. Ridley used a plastic lens to replace the cataract lens during surgery. Dr. Ridley’s first attempt at inserting an intraocular lens occurred in 1949 in a 45 year old female patient. Unfortunately, there were complications due to insufficient aftercare and Dr. Ridley removed the implant, but persisted, successfully reinserting the lens in the same patient only a year later. Dr. Ridley continued to perform this new type of cataract surgery, but kept it private by not publishing his astonishingly positive results. All of his secrecy changed in 1951 when a patient accidentally scheduled a cataract removal with a Frederick Ridley instead of Harold Ridley. Frederick convinced Dr. Ridley to publish his results before someone else heard of his technique, and by 1952 Dr. Harold Ridley was in Chicago at the American Association of Ophthalmologists Conference presenting his results. Dr. Ridley’s presentation in Chicago was criticized heavily by his American peers, with the exception of Dr. Warren S. Reese of the Wills Eye Hospital in Philadelphia. Dr. Warren S. Reese was born in Scranton, PA in 1892, joined Wills Eye Hospital in 1920 and was promoted to attending surgeon by 1939. As a pilot himself, Dr. Reese was inspired by Dr. Ridley’s innovation in the field of cataract removal and was eager to try the new procedure himself. So eager, according to Dr. Eric Arnott, a fellow ophthalmologist and friend of both Dr. Ridley and Dr. Reese, that “[he] immediately flew back in his private plane to Philadelphia.” The very next day, on March 18, 1952, with the help of a fellow ophthalmologist, Dr. Turgut Hamdi, Dr. Reese became the first American to successfully complete an intraocular lens implant surgery. Eight months after Dr. Reese’s first operation, the Chicago Daily Tribune reports: “Of 27 patients who have undergone this operation, only the first two had unsatisfactory results.” The number reported by the Tribune includes both American and British patients, and the two “unsatisfactory results” include the first female patient operated on by Dr. Ridley as well as his second patient when he was still perfecting his revolutionary technique. At the time of Dr. Ridley’s presentation in Chicago, Dr. Reese was a sixty year old man. While Dr. Reese was able to perform and modify the Ridley operation for two years, in 1954 he became blind in one eye and his years as a practicing ophthalmic surgeon came to an end. Even though he was unable to perform the surgeries, Dr. Reese still acted as an assistant to his colleague Dr. Turgut Hamdi. Five years after his first operation, Dr. Reese co-wrote a paper with Dr. Hamdi aptly titled Five Years’ Experience with the Ridley Operation in which he reports on 115 operations he and Dr. Hamdi had completed. Even after five years of successful operations, many American ophthalmologists were still skeptical about the insertion of a foreign body into the eye. Dr. Reese recollects “few mature, experience ophthalmic surgeons have attempted the Ridley operation, and so there is practically no literature on it and the various modifications that have been proposed.” 2 Even with the lack of literature, Dr. Reese was able to modify the original Ridley operation for the better. The technique Dr. Reese and Dr. Hamdi used on the majority of their patients was “designed for simplicity, speed, control of hemorrhage and minimum trauma.” This new technique was very successful, allowing operations to be performed on patients in a wide age rage, as well as those who required superior vision for their career; these included a surgeon, a pilot and a train conductor. Dr. Reese states in his paper that “the commercial pilot astounded the Civil Aeronautic Examiners with his remarkable depth perception” which shows the degree to which the Ridley operation, as well as Dr. Reese’s modifications, restores a patients vision. While the techniques for cataract removal have stayed shockingly similar since the 1960’s, the types of lenses implanted into the patient’s eye continue to evolve. Patients today have the advantage of multifocal, toric, blue-light filtering or light-adjustable intraocular lenses. All of which provide extraordinary vision corrections post-cataract removal, depending upon the needs of the patient. Dr. Angela Chango, an optometrist with ten years of experience and a graduate of the Pennsylvania College of Optometry, believes that without the advancements made by Dr. Ridley and Dr. Reese “the forefront of ophthalmic technology on preventing or treating cataracts and not all of these wonderful elective procedures we have now like Lasik and intraocular contact lenses would exist.” Dr. Warren S. Reese died September 19, 1985 at the age of 93. Dr. Eric Arnott remembers Dr. Reese as “one of America’s most illustrious surgeons.” Certainly Dr. Reese contributed a great deal to the practice of ophthalmic surgery. Had it not been for Dr. Ridley’s inspiration and Dr. Reese’s persistence in perfecting the surgery the 22 million American’s with cataracts might be destined to wear thick glasses for the rest of their lives. Sources: Albert, Daniel M. and Diane D. Edwards. The History of Ophthalmology. Cambridge, MA: Blackwell Science, Inc, 1996. Print. Arnott, Eric J. A New Beginning in Sight. London: Royal Society of Medicine, 2007. Print Choyce, Peter. "One on One with Peter Choyce." Interview. Ocular Surgery News 1 Nov. 1999: n.pag. OSNSuperSite. Web. 10 Oct. 2010. <http://http://www.osnsupersite.com/view.aspx?rid=14281> "Interview with Dr. Angela Chango, OD." E-mail interview. 07 Nov. 2010. Reese, Warren S., and Turgut N. Hamdi. "Five Years' Experience with the Ridley Operation." American Medical Association 58.3 (1957): 389-91. JAMA & Archives: Archive of Ophthalmology. Web. 12 Oct. 2010. <http://http://archopht.amaassn.org/cgi/reprint/58/3/389?maxtoshow=&hits=10&RESULTFORMAT=1&author1=Reese&and orexacttitle=and&andorexacttitleabs=and&andorexactfulltext=and&searchid=1&FIRSTINDEX=50 &sortspec=relevance&fdate=7/1/1950&resourcetype=HWCIT>. Segre, Liz. "Intraocular Cataract Lenses (IOLs): Premium | Aspheric | Toric." Consumer Guide to Eyes, Eye Care and Vision Correction - LASIK, Contact Lenses and Eyeglasses. Mar. 2010. Web. 12 Oct. 2010. <http://www.allaboutvision.com/conditions/iols.htm>. 3 Tasma, William. "Warren S. Reese, M.D." Trans Am Ophthalmol Soc 88 (1990): 13-15. National Center for Biotechnology Information. Web. 10 Oct. 2010. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1298573/pdf/taos00011-0043.pdf>. Van Dellen, Dr. Theodore R. "How to Keep Well." Chicago Daily Tribune 4 Nov. 1952: 14. Print. 4