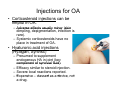
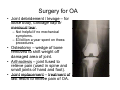
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
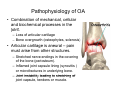
Sports Medicine at Sea 2011 Evaluation and Management of Osteoarthritis R b tS Robert Sallis, lli MD MD, FAAFP FAAFP, FACSM Co-Director; Sports Medicine Fellowship Department of Family Medicine Kaiser Permanente Medical Center Fontana,, California • Joint problems affect some 43 million Americans. • Most common cause off disability di bilit iin adults • More M costly tl th than diabetes and cancer. cancer • Numbers are increasing. Osteoarthritis • Most common joint disorder, with predilection for those over 50. • Slowly Sl l progressive, i causing i continued ti d breakdown of articular cartilage and changes in subchondral bone. • Common synonyms are osteoarthrosis (OA) and degenerative joint disease (DJD). – Osteoarthrosis may be better term since inflammation is usually mild. mild – Degenerative changes are the predominant factor contributing to disability. disability Occupational Hazard for Athletes? The hands of a former NFL f tb ll player football l • Cedric C di H Hardman d – 13 year pro football career defensive d f i end d – SF 49ers and Oakland Raiders – 2 time All Pro – 49ers 49 currentt all-time ll ti sacks leader – Raider Raider’s s Super Bowl XV champion • “No relief, there’s never any relief. Day in, day out, I feel like crap. Don’t believe anything people say about those golden years of your life. They suck” Overview • Review pathophysiology, epidemiology gy and risk factors for OA. • Discuss a practical approach to the diagnosis of OA. • Summarize current treatment modalities for OA from a clinical perspective and present a rational treatment plan. Pathophysiology of OA • Combination of mechanical, cellular and biochemical processes in the j i t joint. – Loss of articular cartilage – Bone overgrowth (osteophytes (osteophytes, sclerosis) • Articular cartilage is aneural – pain must arise from other structures structures. – Stretched nerve endings in the covering of the bone (periosteum). – Inflamed joint capsule lining (synovitis ) or microfractures in underlying bone. – Joint instability instabilit leading to stretching of joint capsule, tendons or muscle. Epidemiology of OA • Over 40 million suffer with OA in U.S. (increasing as baby boomers age). • 70-90% older than 75 have at least one joint j i t iinvolved. l d • Total cost of arthritis exceeds 2% off GNP. GNP • Men & women equally affected: –B Before f 50, 50 prevalence l off OA in i mostt joints greater in men than women. – After 50, women more affected in hand, foot and knee; Men more in hip. Classification of OA • Idiopathic Osteoarthritis – Localized - commonly affects hands, hands feet feet, knee knee, hip, and spine. – Generalized - involves 3 or more joint sites sites. • Secondary Osteoarthritis (specific conditions increase risk): – Other bone/joint disorders like osteonecrosis, RA gout, RA, gout septic arthritis arthritis, Paget’s Paget s, CPPD. CPPD – Other diseases like diabetes, acromegaly, hypothyroidism neuropathic (Charcot) hypothyroidism, arthropathy, and frostbite Risk Factors for OA • • • • • • • • Age A Obesity Injury j y or conditions Genetics Gender Education (lower education level) Physical Inactivity Ethnicity (Whites > Blacks > Hispanics) • Physical and anatomic factors (unequal leg length, flat feet, bowed legs or knock knees) knees). • Congenital joint abnormality (Slipped Capital Femoral Epiphysis, LegCalve Perthe s) Calve-Perthe’s) • Work and leisure activity (risk for injury) Joints Commonly Involved in OA 90% o of Cases Involve 3 Joints • Knees (41%) • Hands H d (30%) • Hips (19%) Diagnosis of OA • Made largely by history & exam and confirmed with imaging. • Signs and symptoms: hallmark is pain and stiffness in one or only a few joints. –P Presentt for f months th to t years; Slowly Sl l progressive; Worsens with activity. – Symmetric joint involvement. – Morning stiffness; usually resolves in <30 min. “Gelling” after periods of inactivity. – Prolonged P l d stiffness tiff and d jjoint i t enlargement often evident with progression – Crepitus C it ((grating ti sensation ti iin jjoint) i t) iis late symptom. Exam Finding g with OA • Boney deformity – Heberden’s (DIP) and Bo chard’s (PIP) nod Bouchard’s nodules les – Osteophytes – Muscle atrophy • Painful motion – Painful IR with hip OA – Painful to squat with knee OA. – Painful pinch with thumb OA. OA • Neurological signs (altered sensation, reduced strength or reflexes). Muscle atrophy Radiographic Changes of OA • X-ray findings with OA include: – Joint space narrowing and osteophyte formation. – Pseudocysts P d t and d iincreased d density of subchondral bone. • Can provide objective evidence of disease. – Absence does not exclude diagnosis. – Can have x-ray changes of OA b t no symptoms but t or disability. di bilit Treatment Goals for OA • 4 Main Goals – Control pain and swelling – Minimize disability y – Improve the quality of life – Educate patient about their role in the management •S Subjective bj ti complaints l i t and d objective bj ti findings help guide the design of appropriate therapeutic goals. OA Treatment Should be Individualized to: • Patient's Patient s expectations • Level of function and activity • Joints involved and the severity of patient's disease • Occupational and vocational needs • Nature of any coexisting medical problems Treatment Options for OA • Non-pharmacologic measures • Oral medications – Acetaminophen and NSAID s NSAID’s – Narcotic analgesics – Antidepressants – Supplements • Topical Treatments (ice, heat, creams) • Injectables – Cortisone – Hyaluronic acid • Surgical treatment Treatment of OA • Paradigm shift in OA treatment over past few years – non-pharmacologic measures (not drugs) have become the keystone of treatment. • Previouslyy NSAID’s were focus. – Studies showed only modest effectiveness. – Potential serious adverse effects effects. • Drugs should be used as adjuncts ((not alternatives)) to other measures. – Benefits of non-pharmacologic measures and drugs often additive – May permit reduction in dose of NSAID NSAID’ss or analgesics used. Non-Pharmacologic Non Pharmacologic Measures • Exercise and weight loss • Thermal modalities • Education • Joint J i t protection t ti • External supports • Rehabilitation and sports activity y Exercise and Weight Loss • Exercise – can improve general health and be therapeutic. – OA is major reason for inactivity in elderly – health benefits of exercise lost. – “Functional” Functional exercises involving ADL’s best (climbing stairs, getting out of chair). – Non weight bearing with bike or water exercise. • Weight loss – helps pain with knee or hip OA OA. – Decreases risk for developing OA. – Next to age, obesity biggest risk f OA. for OA Thermal Modalities • Heat – helps pain and spasm – use prior to stretching. g – Moist heat better than dry. – Hot paraffin or heat mitten for hands. – Deep heat given by ultrasound or diathermy (microwave or shortwave) • Cold – helps relieve muscle aches after exercise. – May help control swelling. swelling – Apply by ice packs, ice massage or local spray. Education and Joint Protection • Patient education – that gives encouragement, reassurance, advice on exercise and measures to unload joint (cane (cane, footwear) helps in selfself management. protection – of arthritic jjoint from stress • Joint p decreases pain and preserves cartilage. – Walking transmits 3.5x body weight across joint, while squatting transmits 9x (choose swimming over running over tennis). – Instability in knee OA common – helped with therapy program or controlled t ll d exposure tto movements t th thatt challenge stability. – Ambulatory assistive devices – such as canes and walkers can support gait. Fitting a Cane • When placed vertically alongside l id ttoes, ttop off cane should be aligned with ith ulnar l styloid. t l id • Force on the cane should be directed downward. • Should be placed in contralateral hand. External Supports • Functional knee braces (unloader brace) – helpful for medial compartment arthritis. arthritis Produce valgus thrust to unload medial compartment. • Elastic bandages – can reduce pain and feeling of giving way. Loose fitting bandages better. • Patella taping – can reduce pain and improve function in patellofemoral compartment OA. • Wedged insoles / orthotics – may reduce loading on medial or lateral knee compartment. • Splinting for hand OA – helps relieve pain for base of thumb OA. Unloads medial compartment Other Non-Pharmacologic Measures • Contractures – of soft tissues and tendons around joint with OA are common. common Can prevent by passive ROM and stretching g and active ROM exercises. • Tai Chi – ancient Chinese f form off conditioning diti i exercises i shown to reduce falls in elderly. y • Acupuncture – may relieve pain and improve function (d t nott conclusive). (data l i ) Medications • None shown to halt the progression of OA. • Common meds used: – Acetaminophen and NSAID’s – Tramadol – COX-2 inhibitors (Coxibs) – Narcotic analgesics – Topical Creams (Capsaicin cream, Bengay, NSAID’s) – Antidepressants A tid t – Supplements NSAID’s and Acetaminophen • How did NSAID’s fall from grace? – Efficacy of anti-inflammatory dose of NSAID (Motrin 800 TID) shown no better than analgesic dose (400 TID) or ACET (1gm QID). – Based on safety safety, efficacy and cost, cost 1995 ACR guidelines recommended ACET as 1st line treatment for OA. – ACR recommends NSAID if signs of joint inflammation (no good data to support). – Black Box warning (all NSAIDs) for CV & GI effects (2005). • ACET and NSAID effects may be additive (can use lower dose of NSAID). • NSAID’s NSAID’ and d ACET only l modestly d l effective ff i iin OA – symptom control rarely complete. Acetaminophen (Tylenol) • Nonprescription analgesic that is drug of choice for OA pain. • Dose up to 4 g/day – 1000 mg four times a day. – 650 mg every 4 hours. • Adverse effects generally mild mild. – Hepatotoxicity is rare; usually a/w excess alcohol use use. – There is suggestive evidence (not definitive) that chronic use has dosedose dependent, long-term nephrotoxicity. NSAID’s • Indicated for inflammatory OA or non-inflam failing to respond to ACET; or for moderate to severe pain. – Most often use oral – Topical preparations available (Diclofenac gel or patch). • 2004 meta meta-analysis anal sis (15 RCT’s) – ACET superior to placebo in relief of OA pain, but less effective than NSAIDs. – GI side effects more common with NSAID’s; ACET and COX-2 about same GI risk. • Diclofenac (Voltaren) gel first topical NSAID – Mainly for hand & knee OA when can’t take oral NSAID. – Efficacy no better than placebo after 2 weeks. – Black box warning for CV and GI risk. Classification of NSAID’s • Non-selective COX Inhibitors: – Propionic acid derivatives (Ibuprofen, Naproxen) – Acetic acid derivatives (Indomethacin, Sulindac, Diclofenac, Nabumetone) – Salicylic Acid derivatives (Aspirin, (Aspirin Diflunisal) – Nonacetylated salicylates (Salsalate) – Enolic acid ((Oxicam)) derivatives ((Piroxicam,, Meloxicam) – Fenamic acid derivatives (Meclofenamic acid, Tolfenamic acid) • Selective COX-2 inhibitors: – Celecoxib FDA alert (Rofecoxib & Valdecoxib withdrawn) • If one not working, try one from a different class. COX-2 Inhibitors (Coxibs) • These NSAID’s selectively inhibit COX-2 and spare COX-1. – Lower incidence of upper GI irritation (lost if taking ASA) ASA). – Despite lay press claims, efficacy in OA no greater than nonselective NSAID’s. – Cost C t off these th drugs d much h hi higher. h – Traditional NSAID plus PPI (to protect stomach) just as good for those with GI upset and much cheaper. • Vioxx and Celebrex may slightly (.3-.5%) increase risk of MI. – Sept 04’ 04 Merck withdraws Vioxx from market. – Celebrex shown to have similar risk (NEJM, 3/05) – on market with black box warning. – Bextra removed from market 4/05 due to life-threatening life threatening skin reactions. Selecting an NSAID • Immense variability in patients' response to the wide variety of NSAID’s used. – Start with OTC (aspirin, ibuprofen or naproxen). – Low dose ibuprofen p ((<1600 mg/day) g y) may y have less serious GI toxicity. – Nonacetylated salicylates (salsalate), sulindac, and nabumetone appear to have less renal toxicity. – Salsalate & nabumetone less antiplatelet activity. – Avoid long-term indomethacin with hip OA (? accelerated l t d jjoint i td destruction). t ti ) – Avoid COX-2 if hx of CVD or risk factors Tramadol • Analgesic with uncertain MOA – Side effects similar to weak opioids (constipation); rate of GI upset may be higher. – Seizures additional risk (esp if on antidepressants or neuroleptics) • Used alone or in combo with ACET; may also be added to NSAID or COX-2. – Tramadol + ACET roughly equivalent to Tylenol #3 for OA pain. Other Medications • Narcotic N ti analgesics l i – Consider when ACET and/or NSAID’s not providing adequate analgesia. – Concerns about tolerance and dependence. – Tramadol nice alternative. • Antidepressants – Good for chronic pain (depression common). – Amitriptyline and Imiprimine most used. used • Topical Creams – Capsaicin cream, Bengay. – Shown to relieve pain in OA of hand and knee. Supplements • Glucosamine – likely effective. • Chondroitin – may be effective, often combined with Glucosamine. • SAM-e – mayy be as effective as coxib. • Selenium – no benefits shown. • Folic Acid – may be effective for hand OA (combined with B-12). • Zinc – more study needed. • Vitamin C – more studyy needed. Injections for OA • Corticosteroid injections can be helpful in OA. – Adverse effects usually minor (skin dimpling, depigmentation, infection is rare). – Systemic corticosteroids have no place in treatment of OA. • Hyaluronic acid injections (Hyalgan Synvisc) (Hyalgan, – Presumed to supplement endogenous HA in joint (key component of synovial fluid) fluid). – Efficacy similar to steroid injection. – Severe local reactions reported. – Expensive E i – classed l d as a d device, i nott a drug. Surgery for OA • Joint debridement / levage – for loose body, cartilage flap or meniscal tear. – Not helpful if no mechanical symptoms. – $3 billion a year spent on these procedures. • Osteotomy – wedge of bone removed to shift weight off damaged area of joint. • Arthrodesis – jjoint fused to relieve pain (used in spine and small joints of hand and foot). • Joint replacement – treatment of last resort to relieve pain of OA. EBM Recommendations For Tx Knee OA From BMJ Clinical Evidence • Beneficial Treatments – Exercise and physiotherapy (pain relief and improved function) – NSAIDs (oral) for short term pain relief • Likely to be Beneficial Non-surgical Treatments – – – – – – Corticosteroids (intra (intra-articular articular — short-term short term pain relief) Hyaluronan (intra-articular) Joint bracing NSAIDs (topical) for short-term pain relief Simple oral analgesics (short-term pain relief only) Taping EBM Recommendations For Tx Knee OA From BMJ Clinical Evidence • Likely to be Beneficial Surgical Treatments – Knee K replacement l t – Osteotomy • Trade off between Benefits and Harms – Opioid analgesics • Unknown Effectiveness – – – – – – Acupuncture Capsaicin Chondroitin Education (to aid self management) Glucosamine Insoles My Approach to Treating OA • Rest until pain free; exercise to tolerance (cross train). – Weight loss – Thermal treatments – PT, braces, cane etc. • A Acetaminophen t i h up tto 4 gm/d, /d consider adding NSAID (different class if no response). ) • Glucosamine 500 mg TID, Chondroitin 400 TID, SAM-e 200400 TID ($$) ($$). • Cortisone injections. • Elavil HS ((help p with sleep), p) Tramadol for severe pain. • Surgical options last resort. Arthritis Foundation Ads “Moving is the best medicine” medicine Thank You!