Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
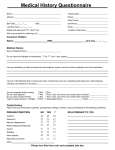
MONTE VISTA EYE CARE Paul W. Heersink, O.D. REGISTRATION FORM Today’s Date ______/______ /_______ PATIENT INFORMATION Legal First Name______________________________ M.I. _____ Last Name ___________________________________ Date of Birth _____/_____ /_____ Age ______ Sex: □ Female □ Male Marital Status: □ Single □ Married □ Other Social Security # ______/______/_______ Mailing Address ______________________________________________________________ Home Phone ____________________________ City _____________________________________________ State _____ Zip _____________ Cell Phone ____________________________ Occupation ____________________________ Employer _________________________________ Work Phone ____________________________ Spouse’s Name ______________________________ If minor, parent(s)/guardian(s) names_____________________________________________ Emergency Contact ______________________________ Relationship _____________________ Telephone # ____________________________ RESPONSIBLE PARTY AND BILLING INFORMATION Legal First Name______________________________ M.I. _____ Last Name ___________________________________ Date of Birth _____/_____ /_____ Social Security # ______/______/_______ Relationship to Patient ____________________________________ Mailing Address ______________________________________________________________ Home Phone ____________________________ City _____________________________________________ State _____ Zip _____________ Cell Phone _____________________________ Occupation ___________________________ Employer __________________________________ Work Phone _____________________________ INSURANCE INFORMATION Vision Insurance Primary _____________________________________ Policy Holder’s Name ____________________________ Date of Birth _____/_____ /_____ Member ID # ______________________________________ Group # _________________________ Medical Insurance Primary ______________________________________________ Member ID # _____________________ Group # _________________________ Secondary ___________________________________________ Member ID # ______________________ Group # _________________________ STATEMENT OF PERMIT I request that payment of authorized Medicare or other insurance carrier benefits be made on my behalf to Monte Vista Eye Care for any services furnished to me by Dr. Paul W. Heersink. I authorize any holder of medical information about me be released to the Health Care Finance Administration (Medicare) or any other insurance carrier that I have contracted with, or their agents, any information needed to determine those benefits or the benefits payable for related services. I have received a copy of the Notice of Medical Information Privacy Rights for Monte Vista Eye Care. ____________________________________________________ ___________________________________ Patient’s Signature Date MONTE VISTA EYE CARE Paul W. Heersink, O.D. HEALTH HISTORY Legal First Name_____________________________ M.I. ____ Last Name _____________________________ Date of Birth _____/_____ /_____ Name of Family Physician ___________________________________________ Telephone # _________________________ List allergies to medications: ________________________________________________________________________________________________ Current medications and reason for taking (attach medication list if needed): __________________________________________________________ ________________________________________________________________________________________________________________________ List any major injuries, surgeries and/or hospitalizations you have had: ______________________________________________________________ ________________________________________________________________________________________________________________________ Are you pregnant and/or nursing? □ Yes □ No Do you wear glasses? □ Yes □ No If yes, how old is your present pair of lenses? __________ Do you wear contact lenses? □ Yes □ No If yes, how old is your present pair of lenses? __________ If NO, are you interested in being fit with contact lenses today? □ Yes □ No Type of contact lenses: □ Rigid □ Soft □ Extended Wear □ Hybrid □ Scleral Are they comfortable? □ Yes □ No Is there any specific reason or concern you are here for today? ____________________________________________________________________ Date of Last Eye Exam ________________ Name of Eye Doctor _______________________________Telephone # _________________________ Please check all conditions that apply to you and/or your family. DISEASE/CONDITION SELF NO YES ? RELATIONSHIP TO YOU Amblyopia (lazy eye) Strabismus (turned eye) Cataract Glaucoma Macular Degeneration Retinal Detachment/Disease Dry Eyes Floaters / Spots / Flashing Lights Headaches / Migraines Cancer Diabetes Heart Disease High Blood Pressure Thyroid Disease Other Social History □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ □ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ ___________________________________________ Do you drive? □ Yes □ No If yes, do you have visual difficulty when driving? □ Yes □ No What do you do for recreation and leisure (hobbies)? _____________________________________________________________________________ Are you active in sports? If so, what type? _____________________________________________________________________________________ Do you use tobacco products? □ Yes □ No If yes, type/amount/how long: ___________________________________________________ Do you drink alcohol products? □ Yes □ No If yes, type/amount/how long: __________________________________________________ Do you use illegal drugs? □ Yes □ No If yes, type/amount/how long: ___________________________________________________ MONTE VISTA EYE CARE Paul W. Heersink, O.D. FINANCIAL AGREEMENT AND OFFICE POLICY Thank you for choosing Monte Vista Eye Care as your eye care provider. Our practice is committed to providing the best treatment for our patients. In order to do so, the following is a statement of our financial agreement and office policy, which we require you to read and sign prior to any treatment. Insurance All patients must supply us with insurance information, if applicable, before seeing the doctor. CO-PAYMENTS AND/OR CO-INSURANCE CHARGES ARE DUE AT TIME OF SERVICE We accept cash, checks, Visa, MasterCard, Discover and Care Credit. We will bill your insurance company if we are an in-network provider with your carrier. You are responsible for any amount not covered by your insurance. We can bill your insurance and provide accurate insurance coverage only if we are provided with current and accurate insurance information. Your insurance policy is a contract between you, your employer and your insurance company. Please be aware that some, and perhaps all, of the services provided may be non-covered services and not considered reasonable and necessary under your insurance program. We will submit insurance claims once. If the claim is denied, it will be your responsibility to pay any remaining balance and resubmit the insurance claim yourself. If you are not using insurance coverage to cover your examination, all exam fees are due at the time of service. I understand that I am responsible for my debt if my insurance company has not paid within 45 days. I understand that I am ultimately responsible for all expenses incurred for services provided regardless of my insurance status. Any collection costs, attorney fees, court costs, or service fees incurred to collect on my account will be my responsibility. A monthly rebilling charge of 2% will be assessed on all accounts with balances 60 days or older. Past due accounts held for 90 days are subject to third party action. Medical Exams and Insurance Claims Only routine eye care may be covered by vision insurance. All other medically necessary examinations (i.e., eye infection) should be covered under your medical insurance. It will be necessary to supply our office with the appropriate information in order for us to submit any medical claims. Please verify our participation with your insurance carrier prior to the examination. Appointments Any patient arriving fifteen minutes late for their scheduled appointment may be asked to reschedule their appointment. If you are running late or are unable to make your appointment, please contact our office immediately. There may be a charge for a missed office appointment. To avoid any charges, please give our office 24 hours notice when rescheduling or canceling appointments. Material Fees All materials (spectacles, contact lenses, etc.) will require a minimum 50% deposit to be ordered and must be paid in full prior to being dispensed. Some insurance companies require that you pay for materials in full before ordering. Minor Patients The adult accompanying a minor and the parents or guardians are responsible for all fees or the co-payment and/or co-insurance charges at the time of rendered service. Please make the necessary arrangements for payment if a child is to be examined without a responsible adult present. For unaccompanied minors, non-emergency treatment, other than routine eye examinations (i.e.-new contact lens fittings) will be denied unless charges have been pre-authorized. I have read the Monte Vista Eye Care Financial Agreement and Office Policy. I understand and agree to this Office Policy. I agree to allow information regarding my eye examination to be released to my insurance company for claims processing. This agreement will not require renewal. ____________________________________________________________ Patient Name (print) ____________________________________ ____________________________________________________________ Signature of Patient or Responsible Party ________________________________________ Date MONTE VISTA EYE CARE Date of Birth Paul W. Heersink, O.D. NOTICE OF PRIVACY PRACTICES This notice is effective on or after December 31, 2013 This notice describes how medical information about you may be used and disclosed and how you can obtain access to this information. Please review carefully. Uses and Disclosures Treatment: Your health information may be used by staff members or disclosed to other health care professionals for the purpose of evaluating you health, diagnosing medical conditions, and providing treatment. For example, results of laboratory tests and procedures will be available in your medical record to all health professionals who may provide treatment or who may be consulted by staff members. Payment: Your health information may be used to seek payment from your health plan, from other sources of coverage such as an automobile insurer, or from credit card companies that you may use to pay for such services. For example, your health plan may request and receive information on dates of service, the services provided, and the medical condition being treated. Health care operations: Your health information may be used to support date-to-day activities and management of Monte Vista Eye Care. For example, information on the services you received may be used to support budgeting and financial reports, and activities to evaluate and promote quality. Law enforcement: Your health information may be disclosed to law enforcement agencies, without your permission, to support government audits and inspections to facilitate law-enforcement investigations and to comply with government mandated reporting. Public health reporting: Your health information may be disclosed to public health agencies as required by law. For example, we are required to report certain communicable diseases to the state’s public health department. Other uses and disclosures require your authorization: Disclosure of your health information or its use for any purpose other than those listed above requires your specific written authorization. If you change your mind after authorizing a use or disclosure of your information you may submit a written revocation of the authorization. However, your decision to revoke the authorization will not affect or undo any use or disclosure of information that occurred before you notified us of your decision. Additional uses of information Appointment reminders: Your health information will be used by our staff to send you appointment reminders. Information about treatments: Your health information may be used to send you information on the treatment and management of your medical condition that you may find to be of interest. We may also send you information describing other health-related goods and services that we believe may interest you. Individual Rights You have certain rights under the federal privacy standard. These include: o The right to request restrictions on the use and disclosure of your protected health information o The right to receive confidential communication concerning your medical condition and treatment o The right to inspect and copy your protected health information o The right to amend or submit corrections to your protected health information o The right to receive an accounting of how and to whom your protected health information has been disclosed o The right to receive a printed copy of this notice Monte Vista Eye Care Duties We are required by law to maintain the privacy of your protected health information and to provide you with this Notice of Privacy Practices. We are required to abide by the privacy policies and practices that are outlined in this notice. Right to revise privacy practices As permitted by law, we reserve the right to amend or modify our privacy polices and practices. These changes in our policies and practices may be required by changes in federal and state laws and regulations. Whatever the reason for these revisions, we will provide you with a revised notice on your next office visit. The revised policies and practices will be applied to all protected health information that we maintain. Requests to inspect protected health information As permitted by federal regulation, we require that requests to inspect or copy protected health information be submitted in writing. You may obtain a form to request access to your records by contacting a receptionist, Sharon Lujan or Tabitha Valdez. Complaints If you believe that your privacy rights have been violated, you should call the concern/s to our attention by sending a letter describing the cause of your concern to the same address. You will not be penalized or otherwise retaliated against for filing a complaint. If you would like to submit a comment, question or complaint about our privacy practices, you can do so by sending a letter outlining your concern/s to: Gina Garcia – Office Manager/Privacy Officer at Monte Vista Eye Care, 101 Chico Court, Suite B, Monte Vista, CO 81144 • 719/852-3412 MONTE VISTA EYE CARE Paul W. Heersink, O.D.