Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
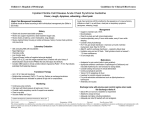
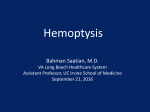
A Case of Postobstructive Pneumonia Secondary to Broncholithiasis By Sara Luckhaupt, MD; LeAnn Coberly, MD—Guest Editors Greg Rouan, MD—Column Editor ABSTRACT An otherwise healthy 54-year-old man presented with shortness of breath and cough that had persisted for 2 weeks, yellow-green sputum, pleuritic chest pain, and orthopnea. His chest examination revealed bibasilar rhonchi—greater on the left side—and intermittent wheezing over the left lung base. Upon evaluation, his condition was diagnosed as community-acquired pneumonia with possible bronchial obstruction. He was admitted to the general medicine service, and despite intravenous (IV) antibiotics, IV fluids, and supplemental oxygen, the patient’s condition worsened. Severe pneumonia with localized wheezing and effusion is typically suggestive of bronchial obstruction due to carcinoma. Though rare, broncholithiasis— endobronchial or peribronchial calcified lymph nodes protruding into the airways—can cause similar postobstructive pneumonia and should be considered in patients with atypical presentations. INITIAL PRESENTATION An otherwise healthy 54-year-old man presented to the emergency department with shortness of breath and cough that had persisted for 2 weeks. At the time of presentation, his symptoms included yellow-green sputum, pleuritic chest pain, and orthopnea. He smoked 1 pack per day for many years, but was not taking any medications. Except for a brother with a diagnosis of lung cancer at age 60, his family history was unremarkable. When examined, he was febrile (temperature, 101.4ºF), with a pulse of 130 beats per minute, and blood pressure of 149/98 mm Hg. His breathing was labored, and his peripheral oxygen saturation was 89% on room air. A chest examination revealed bibasilar rhonchi, which were Dr Luckhaupt is a preventive medicine resident at the University of Michigan Medical School, Ann Arbor, Mich. Dr Coberly is Associate Professor of Clinical Medicine, Department of Internal Medicine, University of Cincinnati College of Medicine, Cincinnati, Ohio. Dr Rouan is Richard W. and Sue Vilter Professor of Clinical Medicine and Associate Chairman of Education, Deprtment of Internal Medicine, School of Medicine, University of Cincinnati, Cincinnati, Ohio. 376 greater on the left side, and intermittent wheezing over the left lung base. An arterial blood gas performed with the patient breathing room air showed a normal pH (7.36-7.44) and PCO2 (normal, 32-48 mm Hg), but a low partial pressure of oxygen (PO2) of 64 mm Hg (normal, 83-108 mm Hg). The initial chest x-ray suggested left lower lobe air space disease with pleural effusion (Figure). The general medicine service admitted the patient with a diagnosis of community-acquired pneumonia, with possible bronchial obstruction. HOSPITAL COURSE Despite intravenous (IV) antibiotics, IV fluids, and supplemental oxygen, the patient’s oxygen requirements steadily increased during the first few days of hospitalization, and serial chest x-rays showed increasing infiltrate and effusion. A chest computed tomography (CT) on the third hospital day revealed extensive loculated left pleural effusion with a compressed lower lobe, which was possibly caused by calcified left hilar lymph nodes. Chest tubes were placed with CT guidance by interventional radiology, and tissue-type plasminogen activator was used to assist in drainage. A repeat CT showed improvement in the effusion, but compression of the left lower lobe persisted. Bronchoscopy was then performed and confirmed the diagnosis of obstructing broncholiths. Figure. Presenting Chest X-ray Showing Left Lower Lobe Consolidation With Pleural Effusion A. B. A. Posteroanterior chest x-ray showing left lower lobe consolidation with pleural effusion, taken upon presentation to the emergency room. B. Lateral chest x-ray, emphasizing the extent of the left lower lobe consolidation, taken upon presentation. Vol. 5, No. 7 n July/August 2005 CLINICAL VIGNETTE Symptoms of Broncholithiasis • • • • • • • Cough Recurrent hemoptysis Fever and chills Purulent sputum Coughing up stones (lithoptysis) Pleuritic chest pain Localized wheezing FOLLOW-UP After recovering from pneumonia, the patient was readmitted to the thoracic surgery team for removal of the obstruction to prevent recurrent pneumonia. Since the broncholiths could not be safely removed via bronchoscopy, left lower lobectomy was performed. Surgical pathology revealed stones consistent with broncholiths, measuring 0.4 to 1.5 cm in diameter, and lymph nodes with necrotizing granuloma, which were negative for neoplasia. Fungi, acid-fast bacilli, or other organisms were not identified in the pathology specimens or in the pleural fluid. DISCUSSION EPIDEMIOLOGY Throughout the last several decades, numerous series of patients with broncholithiasis have been described in the surgical, pulmonology, and radiology literature (Table).1-4 In these series, patients with broncholithiasis ranged from 48.5 to 56.8 years of age; the ratio of men to women was fairly even. Commonly reported symptoms included cough, recurrent hemoptysis, fever and chills, purulent sputum, and lithoptysis (ie, expectoration of stones). Some patients presented with pleuritic chest pain, localized wheezing, or massive hemoptysis. Broncholiths appeared to be more common in the rightside airways than in the left side. Historically, a diagnosis of broncholithiasis was reserved for cases in which at least part of a calcified lymph node actually eroded into the lumen of a bronchus, often resulting in lithoptysis. In order to encompass earlier stages of this dynamic disease, investigators from the Mayo Clinic proposed an extended definition of broncholithiasis in 1971. The updated definition included all patients with peribronchial calcific nodal disease resulting in distortion of the bronchi, as demonstrated by roentgenography or bronchoscopy. Using this broadened definition, 253 cases of broncholithiasis were identified and described at the Mayo Clinic over the course of 30 years.1,2,5 In the early Mayo Clinic series, 86 patients (34%) experienced lithoptysis; obstructive pneumonitis was present in 85 cases (34%) by x-ray (Table). The average duration of clinical manifestations from onset to diagnosis in this series was 41/2 years, whereas the average duration of symptoms in a later study was only 8 months.2 Although asymptomatic broncholithiasis may be found incidentally on chest radiography, broncholithiasis sometimes presents very dramatically. Potential complications include Johns Hopkins Advanced Studies in Medicine bronchoaortic or bronchoesophageal fistula, fatal hemoptysis due to rupture of a pulmonary artery branch, mediastinal abscess, granulomatous mediastinitis with both hemoptysis and hematemesis, and bronchial dehiscence in a lung transplant recipient.3,4,6-9 ETIOLOGY Broncholithiasis has a variety of potential causes. Although organisms are rarely found in extracted broncholiths, evidence exists that broncholithiasis is often preceded by tuberculosis or a fungal infection, such as histoplasmosis.1,2,5 Another cause of broncholithiasis may be silicosis.2,3 Though the reasons are unclear, only a small number of persons with pulmonary hilar calcifications—a common finding on routine chest x-ray—develop broncholithiasis. When calcified material itself has not eroded into the airway, distortion may be caused by an associated inflammatory process.4 In the present case, the exact cause of broncholithiasis was unclear, but the patient lived in a region where histoplasmosis was endemic. Miks et al reported that chemical analysis of a removed broncholith revealed hydroxyapatite crystals, which contained calcium and phosphorus.10 Lin et al reported a broncholith composed of calcium magnesium phosphate and a small amount of calcium carbonate.6 DIAGNOSIS The diagnosis of broncholithiasis usually can be made from a combination of history, radiographic studies, and/or bronchoscopy. The key radiologic finding is a calcified endobronchial or peribronchial lymph node. Other CT findings, including atelectasis, infiltration, bronchiectasis, air trapping, and fluid bronchograms, are due to bronchial obstruction.2,4,11 TREATMENT Depending on the severity of the symptoms, experts recommend observation, or bronchoscopic or surgical treatment.3 Table. Selected Broncholithiasis Case Series Author Year Arrigoni1 (n = 253) Dixon2 (n = 19) Conces4 (n = 15) Olson3 (n = 95) 1971 1984 1991 1999 Male (%) 48 63 53 52 Mean age 54.5 (male)/ 50.6 (female) 52.1 48.5 56.8 Lithoptysis (%) 34 16 13 16 Pneumonia (%) 34* 52† 27‡ 11† Surgery (%) 27 73 60 28 *Radiologic finding of obstructive pneumonitis. †Symptoms of fever or purulent sputum. ‡Symptomatic pneumonia. 377 CLINICAL VIGNETTE Removal of broncholiths by fiberscopic bronchoscopy is difficult and carries a high risk of bleeding. Therefore, rigid bronchoscopy2—with or without fragmentation by forceps,9 laser,10 or surgical resection1,2—may be required to relieve obstruction and prevent bleeding and recurrent infection. The success of bronchoscopic removal depends upon the stage of broncholithiasis. Olson et al reported a success rate of 100% for bronchoscopic removal of broncholiths that were free in the airway lumen. Yet, when removing partially eroded broncholiths, a 48% success rate was achieved. Attempts to remove broncholiths that were distorting airways but had not yet eroded into the lumen were not reported.3 CONCLUSION Broncholithiasis is a less common cause of bronchial obstruction. This patient’s presentation provided several clues that he did not have a typical case of communityacquired pneumonia. Despite having no comorbid illnesses, he was very ill at presentation with significant hypoxemia that progressed despite appropriate therapy. Wheezing localized to the left lower lobe raised suspicion for bronchial obstruction, and the medical team was concerned about the possibility of carcinoma given the patient’s smoking history. Further evaluation and bronchoscopy confirmed the diagnosis of broncholithiasis, which, while rare, also should be considered in any patient with postobstructive pneumonia. 378 References 1. Arrigoni MG, Bernatz PE, Donoghue FE. Broncholithiasis. J Thorac Cardiovasc Surg. 1971;62:231-237. 2. Dixon GF, Donnerberg RL, Schonfeld SA, Whitcomb ME. Advances in the diagnosis and treatment of broncholithiasis. Am Rev Respir Dis. 1984;129:1028-1030. 3. Olson EJ, Utz JP, Prakash UB. Therapeutic bronchoscopy in broncholithiasis. Am J Respir Crit Care Med. 1999;160:766-770. 4. Conces DJ Jr, Tarver RD, Vix VA. Broncholithiasis: CT features in 15 patients. AJR Am J Roentgenol. 1991;157:249-253. 5. Meyer M, O’Regan A. Images in Clinical Medicine. Broncholithiasis. N Engl J Med. 2003;348:318. 6. Lin CS, Becker WH. Broncholith as a cause of fatal hemoptysis. JAMA. 1978;239:2153. 7. Studer SM, Heitmiller RF, Terry PB. Mediastinal abscess due to passage of a broncholith. Chest. 2002;121:296-297. 8. Kefri M, Dyke S, Copeland S, Morgan CV Jr, Mehta JB. Hemoptysis and hematemesis due to a broncholith: granulomatous mediastinitis. South Med J. 1996;89:243-245. 9. Doud JR, Bakhos M, McCabe MA, Garrity ER Jr. Bronchial dehiscence associated with a large broncholith in a lung transplant recipient. Chest. 1992;102:1273-1274. 10. Miks VM, Kvale PA, Riddle JM, Lewis JW Jr. Broncholith removal using the YAG laser. Chest. 1986;90:295-297. 11. Shin MS, Ho KJ. CT fluid bronchogram: observation in postobstructive pulmonary consolidation. Clin Imaging. 1992;16:109-113. Vol. 5, No. 7 n July/August 2005