Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
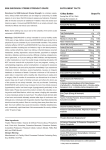
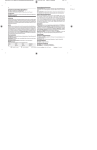
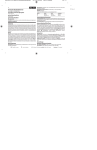
3 MUSC Medical Center Pharmacy Services Title: Adult Electrolyte Replacement - Pocket Reference Cards Policy number: D7 Origin date: Revised date: Review date: Distribution: P&P References: 6/98 Key Words: electrolyte, replacement, dosing, guidelines, magnesium, phosphorus, phosphate, potassium Purpose Statement: These cards are intended to provide general guidelines for magnesium (Mg)(d07_1.frm), phosphorus (P) (d07_2.frm), and potassium (K) (d07_3.frm) electrolyte replacement; to identify oral and parenteral products available at MUSC Medical Center for electrolyte replacement; and to specify appropriate units of electrolyte content in these products. Policies and Procedures: 1. The coordinator of Drug Information or his/her designee will be responsible for printing and distribution of the adult electrolyte replacement cards. 2. Additional copies may be obtained by calling the Drug Information Center at extension 2-3896. 3. The adult electrolyte replacement cards have been approved by MCIG (6/11/98), PLT (6/18/98), and P&T (6/30/98). 4. Updating of the adult electrolyte replacement cards will be done on an as needed basis by the coordinator of Drug Information or his/her designee. Approval for these revisions will be made by the coordinator of Drug Information. No further approval process will be needed for these revisions. 5. The cards will be distributed to the physicians, pharmacists, and adult inpatient nursing units at MUSC Medical Center. The cards will be available to other health care professionals at MUSC Medical Center as requested. 6. The adult electrolyte replacement cards will be included in the MUSC Medical Center Formulary. 3 Magnesium Replacement in Adults (d07_1.frm) The normal laboratory range for magnesium is 1.6 - 2.3 mg/dl. For mild hypomagnesemia (1.3 - 1.5 mg/dl),* oral agents may be used. Oral magnesium-containing agents available or on The Medical University of South Carolina Formulary of Accepted Drugs include: Table 1 - MAGNESIUM-CONTAINING ORAL PRODUCTS Product Name Elemental Magnesium Content Magnesium Oxide Tablet 400 mg (Mag-Ox 400®) 241.3 mg (20 mEq) Magnesium Gluconate Tablet 500 mg (Almora®; Magonate®) 27 mg (2 mEq) (Magtrate®) 29 mg (2 mEq) Magnesium Gluconate Liquid 1000 mg/5 ml (Magonate®) 54 mg /5 ml (4.5 mEq)/5 ml Magnesium Chloride Sustained Release Tablet (Slow-Mag®) 64 mg (5 mEq) 1000 mg Elemental Magnesium = 83.3 mEq = 41.1 mMol For moderate to severe hypomagnesemia (< 1.3 mg/dl or < 1.6 mg/dl with symptoms),* parenteral magnesium replacement is generally indicated. Table 2 - MAGNESIUM-CONTAINING INTRAVENOUS PRODUCT Product Name Magnesium Sulfate 50% - (4 mEq/ml) *Breakpoints arbitrarily assigned. Elemental Magnesium Content 97.6 mg/1 g MgSO4 (8 mEq)/1 g MgSO4 Use clinical judgment in interpretation for patient specific care. References 1. Alfrey AC. Normal and abnormal magnesium metabolism. In: Schrier RW., ed. Renal and electrolyte disorders, 5th ed, Philadelphia: Lippincott-Raven Publishers, 1997: 320-348. 2. Baumgartner TG. Magnesium. In: Baumgartner TG., ed. Clinical Guide to Parenteral Micronutrition, 3rd ed, Fujisawa USA, Inc., 1997: 157-180. 3. Elin RJ. Magnesium metabolism in health and disease. Dis Mon 1988; 34 (4): 161-218. 4. McEvoy GK, ed. AHFS Drug Information® 98. Bethesda, MD: American Society of Health-System Pharmacists, Inc., 1998: 1772-1775. 5. McLean RM. Magnesium and its therapeutic uses: a review. Am J Med 1994; 96: 63-76. 6. Olin BR, ed. Drug Facts and Comparisons. St. Louis, MO: Facts and Comparisons, Inc., 1998: 14-14a, 44-44b, 318. 7. Rude RK and Singer FR. Magnesium deficiency and excess. Ann Rev Med 1981; 32: 245-259. 8. Schultz NJ and Chitwood-Dagner KK. Body electrolyte homeostasis. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach., 3rd ed, Stamford, CT: Appleton & Lange, 1997: 1126-1130. 9. Whang R. Clinical disorders of magnesium metabolism. Comprehensive Therapy 1997; 23 (3): 168-173. 10. Whang R, Hampton EM, Whang DD. Magnesium homeostasis and clinical disorders of magnesium deficiency. Ann Pharmacotherap 1994; 28: 220-226. For further information on electrolyte product or nutritional replacement, please contact FIRSTDOSE Pharmacy (#792-2179) or Nutrition Services (#792-4100). prepared 6/98 T.Seo, Pharm.D. Table 3 - MAGNESIUM REPLACEMENT IN ADULTS Indication Dose Mild Hypomagnesemia (1.3 - 1.5 mg/dl) Magnesium Oxide 400 mg tablet without Symptoms 1-2 tablets po QD-QID, as tolerated Magnesium Gluconate 500 mg tablet 1-2 tablets po QD-QID, as tolerated Magnesium Chloride SR tablet 1-2 tablets po QD-BID, as tolerated Moderate to Severe Hypomagnesemia (< 1.3 mg/dl or < 1.6 mg/dl with Symptoms) Magnesium Sulfate 1-2 g IV, up to q6hrs as needed Magnesium Sulfate Usual 4-6 g IV/day Not to exceed 12. 5 g in 12 hrs Severe Hypomagnesemia (< 1.3 mg/dl) with Lifethreatening Symptoms (e.g., arrhythmias) Magnesium Sulfate 2 g IV push over 1 min (diluted to 10 ml in NS); then 0.5 mEq/kg LBM IV infusion over 5-6 hrs; then 0.5 mEq/kg LBM IV infusion over 17-18 hrs; then (on days 2-5), 0.5 mEq/kg LBM/day divided in maintenance IV fluids. Keep 10 ml Calcium Gluconate or Calcium Chloride 10% IV on hand when administering magnesium as IV bolus. (LBM = lean body mass) Empiric dosing recommendations are for adults with normal organ function and are not meant to replace clinical judgment for individual patient care. Oral dosing ranges may differ from manufacturers’ labeling for chronic magnesium supplementation. Clinical Practice Points • Serum magnesium levels may not reflect total body magnesium content since only about 1 - 2 % of magnesium is distributed in extracellular fluid. • Replacement over 3 to 5 days may be necessary to replete total magnesium stores. • Maintenance doses may be necessary in patients with continued magnesium losses. • Caution should be taken in patients with renal impairment. These patients may require lower doses (e.g., 50 % of normal dose) and more frequent monitoring. • Oral magnesium product intake may be limited by diarrhea. • Magnesium-Aluminum combination antacid products (e.g., Maalox®; Mylanta®) are generally not recommended for oral magnesium replacement due to Al+3 content (which may accumulate in renal impairment and may bind phosphate, with potential to promote additional magnesium loss). • For more rapid replacement than provided by oral administration, use parenteral route. • Do not exceed intravenous infusion rate of 150 mg/min MgSO4 (rapid intravenous bolus may cause flushing, sweating, or sensation of warmth). • Dilute intravenous solutions to concentrations < 200 mg/ml (20%) MgSO4 prior to intravenous administration to minimize risk of pain and venosclerosis (e.g., IVPB 2-4 g MgSO4/50-100 ml NS or D5W). • Intramuscular (IM) administration of MgSO4 should be reserved for situations in which peripheral venous access is not readily obtainable since this route of administration may be painful, often requires multiple punctures, and offers no therapeutic advantage over intravenous administration. 3 Phosphorus Replacement in Adults (d07_2.frm) The normal laboratory range for phosphorus is 2.5 - 4.5 mg/dl. For mild to moderate hypophosphatemia (1 - 2.4 mg/dl), oral agents may be used. Oral phosphate-containing agents available or on The Medical University of South Carolina Formulary of Accepted Drugs include: Table I - PHOSPHATE-CONTAINING ORAL PRODUCTS Product Name Phosphorus Content Sodium Phosphate Oral Solution 18 g with Sodium Bisphosphate 48 g /100 ml (Fleet Phospho-Soda®) 90 ml 4.15 mMol /ml 110 mg (4. 8 mEq) Na /ml Sodium Phosphate Enema 6 g with Sodium Bisphosphate 16 g /100 ml (Fleet Enema®) 133 ml 1.38 mMol /ml 37 mg (1. 6 mEq) Na /ml 164 mg (7. 1 mEq) Na & Potassium and Sodium Phosphate Powder 8 mMol 7. 1 mEq K per packet (Neutra-Phos®) Packet Potassium Phosphate Powder (Neutra-Phos K®) Packet 8 mMol 14. 25 mEq K per packet 1 mMol Phosphate = 31 mg Elemental Phosphorus For severe hypophosphatemia (< 1 mg/dl ,< 2 mg/dl if TPN is to be started, or < 2.5 mg/dl with symptoms), parenteral phosphate replacement is generally indicated. Injectable phosphate is available as potassium phosphate (4.4 mEq K /3 mMol phosphate) and sodium phosphate (4 mEq Na /mMol phosphate). Table 2 - PHOSPHATE-CONTAINING INTRAVENOUS PRODUCTS Product Name Potassium Phosphate Sodium Phosphate Phosphorus Content 15 mMol phosphate and 22 mEq K /5 ml 15 mMol phosphate and 20 mEq Na /5 ml References 1. Brooks MJ and Melnick G. The refeeding syndrome: an approach to understanding its complications and preventing its occurrence. Pharmacotherapy 1995;15 (6):713-726. 2. Kingston M and Badawi A. Treatment of severe hypophosphatemia. Crit Care Med 1985;13:16-18. 3. Knoechel JP. The pathophysiology and clinical characteristics of severe hypophosphatemia. Arch Intern Med 1977; 137:203-220. 4. Lentz RD, Brown DM, Kjellstrand CM. Treatment of severe hypophosphatemia. Ann Intern Med 1978; 89: 941944. 5. Lloyd CW and Johnson CE. Management of hypophosphatemia. Clin Pharm 1988;7:123-128. 6. Olin BR, ed. Drug Facts and Comparisons. St. Louis, MO: Facts and Comparisons, Inc., 1998: 12-12a,48-48a. 7. Perreault MM, Ostrop NJ, Tierney MG. Efficacy and safety of intravenous phosphate replacement in critically ill patients. Ann Pharmacother 1997;31:683-688. 8. Popovtzer MM, Knochel JP, Kumar R. Disorders of calcium, phosphorus, vitamin D, and parathyroid hormone activity. In: Schrier RW, ed. Renal and electrolyte disorders, 5th ed, Philadelphia: Lippincott-Raven Publishers, 1997: 241-319. 9. Rosen GH, Boullata JI, O’Rangers EA, et al. Intravenous phosphate repletion regimen for critically ill patients with moderate hypophosphatemia. Crit Care Med 1995;23:1204-1210. For further information on electrolyte product or nutritional replacement, please contact FIRSTDOSE Pharmacy (#792-2179) or Nutrition Services (#792-4100). prepared 6/98 T.Seo, Pharm.D. Table 3 - PHOSPHATE REPLACEMENT IN ADULTS* Indication Dose Mild to moderate hypophosphatemia (1 - 2.4 K Phosphate or Na Phosphate mg/dl) without symptoms 0.16 mMol phosphate/ kg IV over 6 hours Neutra-Phos® or Neutra-Phos K® 1-2 packets po BID-QID, as tolerated Dilute each packet in 75 ml water Fleet Phospho-Soda® 5-15 ml po BID-TID, as tolerated Dilute each dose in 120 ml water Severe Hypophosphatemia (< 1 mg/dl, <2 mg/dl if TPN is to be started, or < 2.5 mg/dl with symptoms) Maximum phosphate dose K Phosphate or Na Phosphate Usual 0.2 - 0.24 mMol phosphate/kg IV over 6 hours 0.24 mMol phosphate/ kg over 6 hours Usually not > than 45 mMol phosphate/24 hrs Normal daily dose (after phosphorus level returns to normal) 0.14 - 0.4 mMol phosphate/kg over 24 hours Includes dietary intake of phosphorus Empiric dosing recommendations are for adults with normal organ function and are not meant to replace clinical judgment for individual patient care. Oral dosing ranges may differ from manufacturers’ labeling for phosphorus supplementation. Use ideal body weight (IBW) for dosing if total body weight is > than 20% over IBW. *Note: Replacement dose is in addition to routine daily dose of 0.14 - 0.4 mMol phosphorus/kg/day Clinical Practice Points • It may be difficult to assess total body phosphorus deficit since < 1 % of phosphorus is distributed in extracellular fluid and distribution may be affected by patient’s pH, blood glucose concentration, and insulin availability. • Caution should be taken in patients with renal impairment. These patients may require lower doses and more frequent monitoring. • Caution in patients with low serum calcium levels, as phosphorus replacement products may promote hypocalcemia. • Caution in patients with elevated serum calcium levels. Calcium-phosphorus solubility products > 60 - 70 mg2/dl2 may produce calcium-phosphate soft tissue depositions. • Oral phosphorus product intake may be limited by diarrhea. • Fleet Enema® may be given orally for phosphorus replacement. • Cow’s milk contains approximately 0.029 mMol Phosphorus per ml. • Note K or Na content in phosphorus replacement products. • Commercial injections are mixtures of monobasic and dibasic salt forms. To avoid confusion, order and dispense in terms of mMol of phosphorus. • No greater than 30 mMol K Phosphate/dosing unit for ICUs/8W or 15 mMol K Phosphate/dosing unit for all other floors will be dispensed (per MUSC intravenous potassium policy) (e.g., 15-30 mMol K Phosphate /250-500 ml NS or D5W). • A minimum of 4 to 6 hours infusion is required for parenteral phosphate. Risks of rapid IV infusion include hypocalcemia, hypotension, muscular irritability, calcium deposits, renal function deterioration, and hyperkalemia (from K content in K phosphate). 3 Potassium Replacement in Adults (d07_3.frm) The normal laboratory range for potassium is 3.6 - 5 mMol/L. For mild to moderate hypokalemia (2.5 - 3.5 mMol/L)*, oral agents may be used. Oral potassium-containing agents available or on The Medical University of South Carolina Formulary of Accepted Drugs include: Table 1 - POTASSIUM-CONTAINING ORAL PRODUCTS Product Name Elemental Potassium Content Potassium Chloride Controlled Release Tablet (Ten-K®) 10 mEq (750 mg potassium chloride) (K-Dur 20 mEq®) 20 mEq (1500 mg potassium chloride) Potassium Chloride Powder (K-Lor 20 mEq®) 20 mEq (1500 mg potassium chloride) Potassium Chloride Liquid 10% 1.333 mEq /ml (Available also as unit dose cups: 20 mEq/15 ml; 30 mEq/22.5 ml; 40 mEq/30 ml) Potassium Bicarbonate Effervescent Tablet (K-Lyte®) 25 mEq (with 2100 mg citric acid) Potassium chloride 13.4 mEq/g salt; Potassium bicarbonate 10 mEq/g salt; Potassium citrate 9.8 mEq/g salt # mMol/L serum potassium = # mEq/L serum potassium For severe hypokalemia (< 2.5 mMol/L or < 3.6 mMol/L with symptoms),* parenteral potassium replacement is generally indicated. Table 2 - POTASSIUM-CONTAINING INTRAVENOUS PRODUCTS Product Name Potassium Chloride Potassium Acetate *Breakpoints arbitrarily assigned. Elemental Potassium Content 2 mEq /ml 2 mEq /ml; 4 mEq /ml Use clinical judgment in interpretation for patient specific care. References 1. Bear RA and Neil GA. A clinical approach to common electrolyte problems: 2. potassium imbalances. Can Med Assoc J 1983;129:28-31. 2. Kruse JA and Carlson RW. Rapid correction of hypokalemia using concentrated intravenous potassium chloride infusions. Arch Intern Med 1990;150:613-617. 3. Mandal AK. Hypokalemia and hyperkalemia. Med Clin N Amer 1997;81(3):611-639. 4. McEvoy GK, ed. AHFS Drug Information® 98. Bethesda, MD: American Society of Health-System Pharmacists, Inc., 1998:2140-2145. 5. Olin BR, ed. Drug Facts and Comparisons. St. Louis, MO: Facts and Comparisons, Inc., 1998:15-16c, 42-42c, 171c. 6. Saggar-Malik AK and Cappuccio FP. Potassium supplements and potassium-sparing diuretics: a review and guide to appropriate use. Drugs 1993;46(6):986-1008. 7. Schultz NJ and Chitwood-Dagner KK. Body electrolyte homeostasis. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds. Pharmacotherapy: A Pathophysiologic Approach., 3rd ed, Stamford, CT: Appleton & Lange, 1997:1113-1120. 8. Stanaszek WF and Romankiewicz JA. Current approaches to management of potassium deficiency. DICP 1985;19:176-185. 9. Whang R, Whang DD, Ryan MP. Refractory potassium repletion: a consequence of magnesium deficiency. Arch Intern Med 1992;152:40-45. 10. Zull DN. Disorders of potassium metabolism. Emer Med Clin N Amer 1989;7(4):771-793. For further information on electrolyte product or nutritional replacement, please contact FIRSTDOSE Pharmacy (#792-2179) or Nutrition Services (#792-4100). prepared 6/98 T.Seo, Pharm.D. Table 3 - POTASSIUM REPLACEMENT IN ADULTS Indication Dose ORAL REPLACEMENT* Potassium Chloride Serum potassium 2.5 - 3.5 mMol/L without Usual 20-40 mEq po BID-QID, as tolerated Symptoms Mix each powder with at least 120 ml of cold water or juice Dilute KCl 10% liquid in cold water or juice to improve palatability K-Lyte® Effervescent Tablet Usual 25 mEq po BID-TID, as tolerated Dissolve each tablet in 90-120 ml of cold water INTRAVENOUS REPLACEMENT** Serum potassium > 2.5 mMol/L KCl IV infusion, up to 200 mEq/day in divided doses Refer to MUSC IV potassium policy for maximum concentrations and infusion rates Serum potassium < 2.5 mMol/L KCl IV infusion, up to 400 mEq/day in divided doses Refer to MUSC IV potassium policy for maximum concentrations and infusion rates Empiric dosing recommendations are for adults with normal organ function and are not meant to replace clinical judgment for individual patient care. *Note: In mild, asymptomatic cases (serum K > 3 mMol/L), increase in dietary K may be sufficient. Oral dosing ranges may differ from manufacturers’ labeling for chronic potassium supplementation. Usual prophylactic potassium doses are 20 - 30 mEq/day, divided into 2 - 3 doses as tolerated. **The patient’s response, as determined by measurement of serum potassium concentration and ECG monitoring following the initial 40 - 60 mEq infused, should indicate the subsequent infusion rate required. Clinical Practice Points • Serum potassium levels may not reflect total body potassium content since only about 2% of potassium is distributed in extracellular fluid. • Factors which promote 8 cellular uptake of K include: alkalosis, insulin, glucose, #-adrenergic agonists, and aldosterone. Acidosis and #-adrenergic antagonists impair cellular uptake. • During K depletion, serum K initially 9 by .1 mMol/L for each 100-200 mEq total body stores lost; however, serum K falls more slowly after it reaches .2 mMol/L. • Replacement over several days may be necessary to replete total potassium losses. • In hypomagnesmic states, potassium wasting may occur. Serum magnesium levels and replacement may be necessary to address refractory hypokalemia. • KCl is usually the salt of choice in potassium replacement, since the Cl- ion is required to correct hypochloremia which frequently accompanies potassium deficiency. • Alkalinizing salts of potassium (e.g., acetate, bicarbonate) are preferred in instances where metabolic acidosis exists concurrently with potassium depletion. • Potassium prophylaxis may be indicated to prevent hypokalemia in patients who would be at particular risk if hypokalemia were to develop (e.g., patients on digoxin with cardiac arrhythmias; hepatic cirrhosis with ascites; aldosterone excess with normal renal function; potassium-losing nephropathy; chronic diarrhea conditions). • Factors which may predispose to overcompensation with resultant hyperkalemia incl: 9 renal function, diabetes mellitus, acidosis, and potassium-sparing medications (e.g., K-sparing diuretics, ACE Inhibitors, Angiotensin II Receptor blockers). • • Note: salt substitute products (e.g., Adolph’s®, Morton®, Nu-Salt®) contain a significant amount of potassium (e.g., 56 - 68 mEq /5 g product). Refer to phosphorus replacement guidelines for K Phosphate product information.