Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
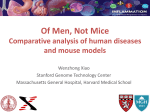
Hematologic Changes in Sepsis and Their Therapeutic Implications Richert E. Goyette, M.D.,1 Nigel S. Key, M.D.,2 and E. Wesley Ely, M.D., M.P.H.3 ABSTRACT The blood and bone marrow constitute the hematologic organ system. Unlike other organ systems, hematologic organs are distributed in space and provide for a variety of seemingly unrelated functions. The hematologic system has both cellular and fluid-phase elements. Cellular elements include erythrocytes, leukocytes, and platelets; fluid phase elements include coagulation factors, natural antithrombotics, and proteins of the fibrinolytic system. The most common abnormalities of the hematologic system in patients with sepsis are anemia, leukocytosis, thrombocytopenia, and activation of the hemostatic system. Dysfunction of the hematologic organ system is an early manifestation of severe sepsis and is seen in virtually all patients with this disease. In concert with alterations in the endothelium, hematologic changes reflect both the body’s reaction to an infectious insult as well as attempts to restore homeostasis. Dysfunction of the hematologic organ system can contribute to multiple organ dysfunctions and death. Recognizing these sepsis-associated changes and understanding the underlying pathophysiology are key to improving outcomes in patients with this deadly disease. KEYWORDS: Coagulation, erythrocytes, hematology, inflammation, leukocytes, platelets, sepsis Objectives: After reading this article, the reader should be able to: (1) recognize the blood and bone marrow as an organ system; (2) understand the key role played by the endothelium in the septic process; (3) discuss alterations in red blood cells, white blood cells, and platelets that occur in sepsis; and (4) describe the therapeutic implications of alterations in formed elements during sepsis. Accreditation: The University of Michigan is accredited by the Accreditation Council for Continuing Medical Education to sponsor continuing medical education for physicians. Credits: The University of Michigan designates this educational activity for a maximum of 1 category 1 credit toward the AMA Physician’s Recognition Award. S epsis with acute organ dysfunction (severe sepsis) is common, frequently fatal, and associated with significant use of health care resources. In the United States alone, there are more than 800,000 cases of severe sepsis each year.1 The mortality in patients with severe sepsis ranges from 28 to 50% or greater. Angus et al report that each organ dysfunction increases the mortality rate of severe sepsis by 20%. It has been estimated that with the increase in the elderly population, use of more invasive diagnostic and therapeutic interventions, Management of Shock; Editor in Chief, Joseph P. Lynch, III, M.D.; Guest Editors, Arthur P. Wheeler, M.D., Gordon R. Bernard, M.D. Seminars in Respiratory and Critical Care Medicine, volume 25, number 6, 2004. Address for correspondence and reprint requests: E. Wesley Ely, M.D., M.P.H., Center for Health Services Research, #6109 MCE, Vanderbilt University Medical Center, Nashville, TN 37232-8300. E-mail: [email protected]. 1Consultant, hematology and oncology, private practice, Knoxville, Tennessee; 2Department of Medicine, Division of Hematology, Oncology, and Transplantation, University of Minnesota Medical School, Minneapolis, Minnesota; 3Department of Medicine, Division of Allergy/Pulmonary/Critical Care Medicine and Center for Health Services Research and the VA Tennessee Valley Geriatric Research, Education, and Clinical Center (GRECC), all at the Vanderbilt University School of Medicine, Nashville, Tennessee. Copyright # 2004 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. 1069-3424,p;2004,25,06,645,659, ftx,en;srm00336x. 645 646 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 and increasing numbers of immunocompromised patients, the incidence of severe sepsis will increase at least 1.5% per year for the next 50 years. The hematologic organ system is a major element in the response to a septic insult and plays a pivotal role in the resolution phase of severe sepsis.2 Therefore, it is important for critical care specialists to be aware of the manifestations and consequences of hematologic dysfunction in patients with severe sepsis. THE HEMATOLOGIC ORGAN SYSTEM DEFINED Organ systems consist of anatomically and/or physiologically related components. Because the activity of most organ systems is focused on a single goal (e.g., gas exchange), the concept is easy to understand. Unlike the heart or the lungs, however, the hematologic system is diffuse, has both cellular and fluid phase elements, and serves a variety of unrelated functions. Consequently, its role as an organ system is often underappreciated. Cellular elements of the hematologic system originate in the bone marrow, transit the blood, and then either exit the body or are cleared by the reticuloendothelial system. Cellular elements include red blood cells, white blood cells, and platelets. Fluid-phase components include coagulation factors, natural anticoagulants, and proteins of the fibrinolytic system. Disparate physiological functions of the hematologic system include gas exchange, acid–base balance, innate and adaptive immunity, and hemostasis. Hematologic changes are almost universal in patients with severe sepsis. Although sepsis-associated hematologic changes can be beneficial, dysfunction, evidenced by alterations in the number of cells, the properties of cells, fluidity of the blood, and/or integrity of the vasculature, can contribute to both morbidity and mortality. THE ENDOTHELIUM Endothelial cell function is tightly integrated with the physiology of the hematologic system, and dysfunction plays a key role in many of the hematologic manifestations of sepsis. Therefore, a brief discussion of endothelial cell physiology is warranted before sepsis-related changes in the hematologic organ system are discussed. With 1011 endothelial cells and a surface area estimated to exceed 1,000 m2, the endothelium surpasses the skin as the largest organ in the body.3,4 The great majority of the endothelium is located in the microvasculature where the endothelial surface area per unit of blood volume is 2 to 3 thousand times greater than in the larger blood vessels.5 Endothelial dysfunction is a key element in the pathogenesis of severe sepsis. This may be secondary to the effects of endotoxin, proinflammatory cytokines, reactive oxygen species, or other substances on 2004 endothelial cells. For example, a single injection of endotoxin in rabbits produces desquamation of 25% of the aortic endothelial surface area within 5 days.6 Alternately, organisms such as Rickettsiae can directly infect endothelial cells and disrupt cellular homeostasis. Severe endothelial injury from a variety of etiologies can produce microvascular coagulopathy and acute organ dysfunction.7 Elevated circulating levels of the soluble (s) forms of thrombomodulin (TM), ICAM-1 (intercellular adhesion molecule-1), E-selectin, and von Willebrand factor (vWF) are frequently measured markers of endothelial dysfunction and injury.8 In children with septic shock, soluble TM levels are increased and the levels correlate with survival status and the extent of organ dysfunction.9 In a population of patients with sepsis, plasma levels of vWF, ICAM-1, and sE-selectin were significantly increased within 8 hours of the development of the acute respiratory distress syndrome (ARDS).10 Sepsis is associated with apoptosis of various cell types.11 In patients with severe sepsis, endothelial cell apoptosis may produce abnormalities in trafficking of blood cells into an infected focus, vasoregulation, and the antithrombosis–thrombosis balance that may contribute to the pathogenesis of septic manifestations such as multiple organ dysfunction, impaired microvascular blood flow, and inability of the body to restore homeostasis. ALTERATIONS OF THE ERYTHRON IN SEPSIS The erythron is the organ responsible for the production of erythrocytes. It is composed of committed red blood cell progenitors, developing erythrocytes, reticulocytes, and mature red blood cells. Mature red blood cells are anucleate, hemoglobin (Hb)-containing sacs, with enzyme systems necessary to maintain the integrity of the sac (red blood cell membrane) and prevent oxidative damage to the contents (Hb). Physiology The sole function of Hb is oxygen transport; when fully saturated, each gram of Hb can bind 1.39 mL of oxygen. Oxygen delivery is a critical physiological process that is a function of microcirculatory blood flow, oxygen concentration in the blood, and oxyhemoglobin dissociation. Because the absolute amount of oxygen physically dissolved in the blood is minimal, the arterial oxygen saturation (SaO2) essentially describes the oxygen that is bound to Hb. The oxygen affinity of Hb is a measure of the pO2 at which Hb is 50% saturated with oxygen (P50). In nonsmokers, the P50 is normally 26.6 mm Hg and varies with the concentration of 2,3-DPG (2,3diphosphoglycerate), temperature, and pH. The Hb concentration is a function of patient age, gender, race, activity level, and altitude above sea level. HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL Following puberty, Hb levels are 2.0 g/dL higher in men than in women, a difference that is a function of the physiological effects of testosterone on the erythron. African Americans have Hb levels that are 0.5 g/dL lower than Caucasians. A recumbent posture for 1 hour will result in a 6% decrease in HCT (hematocrit), with a return of the value to normal 15 minutes after resuming an upright posture. These changes are the result of postural fluid shifts between the intra- and extravascular components of the extracellular fluid space. Over time, altitude-dependent increases in erythropoiesis in individuals residing at 15,000 feet can produce a ‘‘normal’’ Hb that may be as much as 4 g/dL greater than that observed in healthy adults residing at sea level. Pathophysiology Alterations in the properties of individual red blood cells may contribute to the pathophysiology of sepsis. These alterations include abnormalities of oxygen carrying capacity and changes in red cell mechanical properties that may alter the rheology of the microcirculation. In addition, changes in the erythron can affect other components of the hematologic system. For example, the HCT level is inversely correlated with the bleeding time, a test that reflects both platelet function and microvascular integrity. ALTERATIONS IN OXYGEN CARRYING CAPACITY The capacity of the blood to carry oxygen can be impaired by changes in Hb’s oxygen affinity or its concentration or both. Fever and acidosis in patients with sepsis shift the oxygen dissociation curve to the right. As a consequence of the decreased oxygen affinity, red blood cells release oxygen to the tissues more readily. Increased levels of erythrocyte 2,3-DPG also favor oxygen release. Unfortunately, 2,3-DPG is depleted in banked blood and is not restored to normal levels for 6 to 12 hours following transfusion. Consequently, immediately following transfusion the Hb in transfused red blood cells fails to release oxygen as readily and at the same pO2 levels as Hb in metabolically intact erythrocytes. ALTERATIONS IN PROPERTIES OF ERYTHROCYTES In patients with sepsis, alterations in the mechanical properties of the red blood cells may impair microcirculatory blood flow, which may in turn decrease tissue oxygen delivery. Cellular deformability, the ability of a cell to change its shape in response to applied forces, is an important determinant of microcirculatory blood flow. Decreased red blood cell deformability occurs early in sepsis and has the potential to reduce blood flow and increase the time required for cells to transit the microcirculation.12 Alterations in the red blood cell membrane responsible for increased cellular rigidity probably include damage to membrane proteins from reactive oxygen species generated by inflammatory cells and ischemic tissues. Thus, in addition to its negative effect on oxygen delivery, decreased red blood cell deformability may contribute to organ dysfunction outside of the hematologic system. Although its clinical utility has not been established, altered red blood cell deformability has been proposed as a tool to detect sepsis before the appearance of more classical signs and symptoms.13 Experimentally, red blood cell aggregates that could impair microcirculatory blood flow have also been reported in sepsis.14 This tendency to form aggregates likely has a nonimmunologic etiology and may be a consequence of increased acute phase proteins such as fibrinogen that can decrease the erythrocytes’ negative charge (zeta potential), the electrical potential that promotes mutual red blood cell repulsion. Although the significance of red cell aggregates in sepsis pathophysiology is unclear, one laboratory manifestation of the decrease in erythrocyte zeta potential is an increased erythrocyte sedimentation rate (ESR). Clinical and Laboratory Manifestations Extravascular leak of fluids at the onset of sepsis has the potential to produce hemoconcentration. This situation can result in a relative erythrocytosis during the initial phase of sepsis. With time, however, the most common alteration in the erythron in patients with sepsis is anemia. Anemia results in a decrease in the oxygencarrying capacity of the blood. Although anemia can be identified by decreases in the number of erythrocytes or a fall in the HCT, the diagnosis is best established by the Hb concentration. This does not reflect superiority of one parameter or another; instead, the Hb concentration is preferred because it most closely reflects the blood’s oxygen carrying capacity. Diagnostic Considerations Apart from hemodilution, anemia may be the result of blood loss, decreased production (hypoproliferative anemia), or increased destruction (hemolytic anemia) of red blood cells. In most instances, therefore, the anemia in patients with sepsis is multifactorial in origin. BLOOD LOSS Anemia in patients with severe sepsis may be a consequence of bleeding. In most instances, the diagnosis and source of blood loss are readily apparent. The source of the anemia may be less evident in patients who become septic following major trauma with bleeding into the soft tissues of the thigh or the retroperitoneum, for example. Significant blood loss can also occur as a result of multiple phlebotomies necessary to obtain blood to diagnose and monitor patients with critical illnesses 647 648 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 2004 such as severe sepsis. It has been estimated that repeated phlebotomies result in a loss of 24 to 41 mL of blood daily.15–17 In a study of patients with arterial lines hospitalized in the intensive care unit (ICU), the mean blood loss was 944 mL.18 This is equivalent to almost 20% of the blood volume of a 70 kg man and contributed to transfusion requirements in this population. ANEMIA OF SYSTEMIC INFLAMMATION Patients with the systemic inflammatory response syndrome (SIRS) may be anemic. The anemia of systemic inflammation has also been called the anemia of chronic disease. However, the latter term is a misnomer because this syndrome can develop within days of the inciting event in patients with sepsis and other inflammatory disorders.19 Characteristic pathophysiological features of this hypoproliferative anemia include a reticuloendothelial block in iron transport, decreased sensitivity of the erythron to erythropoietin, and shortened red blood cell survival.20 It is tempting to speculate that because this cytokine-mediated process effectively sequesters iron required for microbial growth (as well as erythropoiesis), it may have evolved as a protective mechanism.21 The anemia is generally mild with Hb and HCT values of 8 g/dL and 24% or greater, respectively. The block in reticuloendothelial iron transport is significant enough in approximately one third of patients to produce microcytic red blood cell indices suggestive of iron deficiency. Other laboratory features include low serum iron and iron-binding capacity and increased serum ferritin. Multiorgan dysfunction in patients with severe sepsis can contribute to the onset or progression of the anemia of systemic inflammation. Figure 1 Peripheral blood smear from a patient with disseminated intravascular coagulation. Important manifestations include the presence of schistocytes (fragmented erythrocytes) and the relative absence of platelets. with underlying glucose-6-phosphate dehydrogenase (G6PD) deficiency (more common in those of Mediterranean or African descent) or an unstable hemoglobin. In addition, endogenous oxidants and acid metabolites produced during acute infection may contribute to hemolysis in susceptible patients. During the workup of suspected hemolysis in a patient with sepsis, it is important to bear in mind the possibility that a positive direct antiglobulin (Coombs’) test may be produced not only by autoantibodies but also by adsorption of certain antibiotics (e.g., cephalosporins) onto the surface of red blood cells. In most cases of severe sepsis, infection-associated hemolysis plays only a minor role in clinical manifestations and outcome. However, experimental evidence suggests that hemoglobinemia can increase lethality of endotoxemia through a tumor necrosis factor (TNF)-mediated mechanism.23 HEMOLYSIS Sepsis may precipitate disseminated intravascular coagulation (DIC) with hemolysis due to red blood cell fragmentation. Approximately 25% of patients with DIC will have clinical evidence of microangiopathic hemolysis manifested by the presence of schistocytes on their peripheral blood smear (Fig. 1). Although the clinical presentation is usually not that of severe sepsis, babesiosis, bartonellosis, leishmaniasis, and malaria can also be associated with a prominent hemolytic component. Clinically significant hemolysis can occur in patients with sepsis due to Clostridium perfringens or type B Haemophilus influenzae. In the former, intravascular hemolysis is due to the effects of bacterial lysolecithins that directly lyse red blood cell membranes. In the latter, polyribosyl ribosyl phosphate (PRP) from bacterial capsular polysaccharides is released during infection and binds to the red cell surface.22 Subsequently, these patients may develop antibodies to PRP, which may result in complement-mediated hemolysis. Treatment of infections with sulfonamides and other antibiotics can precipitate Heinz body hemolytic anemia in patients Treatment Considerations Critically ill patients typically receive multiple transfusions of packed red blood cells (PRBCs). In one study, 85% of patients hospitalized in the ICU for more than 1 week received blood transfusions (9.5 0.8 U per patient).24 These were not single-unit transfusions nor were they generally administered because of bleeding. Instead, patients were transfused a constant 2 to 3 units of PRBCs per week with approximately one third of the units administered in the absence of a clear indication. Packed red blood cells are prepared by differential centrifugation, which removes 80% of the plasma resulting in a volume and HCT of 350 mL and 60%, respectively. When transfused into a 70 kg adult, one unit of packed red blood cells will increase the Hb and HCT by 1 g/dL and 3%, respectively. Obviously, continued bleeding or aggressive fluid resuscitation will blunt this response. Until recently, many critical care specialists chose a relatively liberal transfusion strategy based upon the HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL assumption that a more normal oxygen-carrying capacity would benefit the recovery process.25 Despite its lifesaving benefits, however, transfusion of red blood cells is associated with several potential complications. In addition to alloimmunization and transmission of infectious disease, complications of particular importance in the ICU setting include acute hemolytic transfusion reactions, transfusion-related acute lung injury (TRALI), and nosocomial infections secondary to transfusionmediated immunomodulation.26 Hébert et al recently compared restrictive and liberal transfusion strategies in a population of critically ill subjects.27 They reported that a restrictive transfusion strategy with a Hb trigger of < 7 g/dL was as effective as a more liberal strategy that used a Hb of < 10 g/dL to trigger transfusion of red cells in patients without an acute coronary syndrome. However, the mortality benefit of this intervention remains to be confirmed by a large-scale, randomized clinical trial. One strategy to improve oxygen carrying capacity without transfusion is the administration of recombinant human erythropoietin (rHuEPO). Exogenous rHuEPO compensates for the body’s relatively blunted erythropoietic drive produced by the anemia of systemic inflammation. In a recent randomized controlled trial of critically ill patients, administration of 40,000 units of rHuEPO decreased the total number of transfused units of PRBCs by 19% compared with placebo.28 In addition, patients who received rHuEPO had higher Hb levels, despite receiving fewer transfusions than the control group. However the outcomes were similar between the groups, and a cost–benefit analysis of this strategy is not available at this time. The complex systems that balance tissue oxygen delivery with tissue oxygen demand are impaired and can produce tissue hypoxia in patients with sepsis and other critical illnesses. Given the importance of oxygen availability to the tissues, several randomized, controlled clinical trials have evaluated the role of increased global oxygen delivery (DO2). Surprisingly, trials of supranormal DO2 have reported conflicting results, with some showing decreased mortality, others showing no change, and one reporting increased mortality.29 Recently, Rivers et al reported that early goal-directed therapy (EGDT) consisting of standard measures to optimize the central venous pressure (CVP), mean arterial pressure (MAP), and urine output (UOP) plus treatment to increase central venous oxygen saturation (SCVO2) to 70% or greater significantly decreased mortality in patients with severe sepsis.30 Critical elements of the process included initial treatment for 6 or more hours in the emergency department, continuous monitoring of SCVO2, transfusions of PRBCs to a target HCT of at least 30%, and inotropic support with dobutamine if the SCVO2 remained < 70% despite optimized CVP, MAP, UOP, and HCT. Thus early identification and treatment of global tissue hypoxia despite stable vital signs with transfused red blood cells and other appropriate measures can help to restore the balance between oxygen delivery and oxygen demand. ALTERATIONS OF LEUKOCYTES IN SEPSIS Leukocyte alterations are common in patients with severe sepsis. In fact, white blood cells 12.0 109 /L, 4.0 109 /L, or a left shift with > 10 immature neutrophils (bands) are one of the four SIRS criteria employed to establish a diagnosis of sepsis in patients with infection.31 Pathophysiology and Background The initial response to a septic challenge is met by elements of the innate limb of the immune system. In humans, cellular effectors of innate immunity include neutrophils, monocytes/macrophages, natural killer (NK) cells, and platelets. Neutrophils play important roles by phagocytosing infectious organisms, crystalline material (e.g., uric acid), and immune complexes. Cytokines released during inflammation and infection promote migration of bands and mature neutrophils from the maturation-storage pool in the bone marrow into the circulation, whereas metamyelocytes are not released into the blood except in extreme circumstances. Following release, granulocytes randomly enter either the circulating or the marginating pools; the concentration of cells in each pool is approximately equal. A neutrophilic leukocytosis is an appropriate response to many types of infections. However, when the neutrophilic response is exaggerated, lysosomal enzymes and toxic oxygen metabolites released by the excess of inflammatory cells can damage host tissue adjacent to the inflammatory focus. Oxidants released from granulocytes may also inactivate tissue protease inhibitors and thereby contribute to injury of endothelial and parenchymal cells by allowing unchecked enzymatic activity of elastase, collagenase, and other matrix metalloproteinases. In addition, leukocyte counts in excess of 50 109 /L increase blood viscosity with the potential to impair microcirculatory blood flow. The monocyte/macrophage is the human analog of the invertebrate amoebocyte: an innate immune cell that is involved in response to pathogens, wound repair, and hemolymph clotting. By virtue of their ability to upregulate synthesis and release of cytokines such as tumor necrosis factor alpha (TNF-a), as well as expression of tissue factor (TF), monocytes provide one of the critical links between inflammation and coagulation. Monocytes originate in the bone marrow and then transit the peripheral blood to lodge in tissues as longlived macrophages, such as Kupffer’s cells and other reticuloendothelial elements. Monocytes possess pathogen-associated molecular pattern signaling 649 650 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 receptors such as toll-like receptors that are a key component of the innate immune system.32 Unlike the antigen receptors of B- and T-cells, these receptors are encoded in the germline and trigger an immediate effector function. Clinical and Laboratory Manifestations Neutrophilic leukocytosis is a common manifestation of sepsis. It appears to result from a combination of factors, including recruitment of mature neutrophils from the marginating pool into the circulating pool, mobilization of mature and developing neutrophils from the bone marrow, and eventually increased leukopoiesis. In most instances, the leukocytosis is moderate. Examination of the peripheral blood smear in patients with sepsis may show persistence of the primary granules that first appear at the stage of the promyelocyte (toxic granulation), residual blue-gray areas of ribonucleic acid (RNA)-rich cytoplasm (Döhle’s bodies), and cytoplasmic vacuoles (i.e., phagolysosomes, autophagic vacuoles). In some instances, intracellular bacteria can be identified in a stained buffy-coat smear. Neutropenia in patients with sepsis can be the result of depletion of bone marrow granulocyte precursors, a granulocytic ‘‘maturation arrest,’’ or migration of leukocytes into the infected focus in numbers in excess of the bone marrow’s ability to replace them in a timely fashion. Although neutropenia can occur in adult patients with severe sepsis, it is more common in the pediatric population.33 Diagnostic Considerations Sepsis may be the presenting manifestation of a primary hematologic disorder. For example, infection may be the first clue to the neutropenia of aplastic anemia, agranulocytosis, or acute leukemia. In most instances, the etiology of the white blood cell changes is obvious. For example, patients with aplastic anemia are pancytopenic, and the typical patient with sepsis will not have the circulating blasts, promyelocytes, myelocytes, or basophilia that may be variably present depending on the type of leukemia. LEUKEMOID REACTION A patient with sepsis may sometimes present with leukocyte counts in excess of 50 109/L. This extreme nonneoplastic leukocytosis is known as a leukemoid (leukemia-like) reaction. Although infection secondary to granulocyte dysfunction is uncommon in patients with chronic myelogenous leukemia (CML), patients with previously undiagnosed CML may also develop sepsis. In this case, it is important to differentiate a leukemoid reaction secondary to sepsis from CML in a septic patient. Clues from the initial examination and laboratory studies that are suggestive of coexistent CML 2004 include splenomegaly, granulocyte counts > 50 109 /L, basophilia, and the presence of small numbers of circulating blasts and promyelocytes. Additional laboratory studies are not usually required. However, unlike the septic patient who has a normal or elevated leukocyte alkaline phosphatase (LAP), decreased or absent stainable LAP is a feature of granulocytes in CML. Other laboratory studies that can establish the diagnosis of CML but are rarely required on an emergent basis include identification of the Philadelphia chromosome by cytogenetic analysis or fluorescent in situ hybridization, or the presence of the bcr-abl fusion oncogene, the Philadelphia chromosome’s molecular equivalent. Treatment Considerations White blood cell changes of sepsis resolve with effective therapy of the primary disorder. Although the use of hematopoietic growth factors such as granulocytecolony-stimulating factor (G-CSF) or granulocyte macrophage-colony-stimulating factor (GM-CSF) to activate leukocytes and increase their numbers is theoretically attractive, particularly for patients with sepsis and neutropenia, there is no evidence that this approach improves outcomes.34 ALTERATIONS OF PLATELETS IN SEPSIS Thrombocytopenia is a frequent accompaniment of critical illness and is commonly employed in clinical trials of severe sepsis therapies as a marker of hematologic organ system dysfunction.35,36 In the ICU setting, platelet counts < 100,000/mm3 (< 100 109/L) are identified in 20 to 40% of patients.37–39 In a study of an ICU population, sepsis was identified as a major risk factor for thrombocytopenia.37 Platelet counts in critically ill patients are also related to prognosis independent of the Simplified Acute Physiology Score II (SAPS II) and Acute Physiology and Chronic Health Evaluation II (APACHE II) severity scores. In addition, a blunted rise in previously depressed platelet counts is associated with poorer outcomes in acutely ill patients.40 Pathophysiology and Background Megakaryocytes are derived from multipotential hematopoietic progenitor cells. Acting under the influence of thrombopoietin (TPO) and other cytokines, such as stem cell factor, interleukin (IL)-3, IL-6, IL-11, and erythropoietin, progenitor cells progressively differentiate into promegakaryoblasts and mature megakaryocytes.41 Platelet formation results from a combination of budding of platelets from the megakaryocytes’ surface, release of platelets from small preformed regions of the mature megakaryocyte, and by formation of proplatelets, long filaments of megakaryocyte cytoplasm.42 HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL Proplatelets enter the circulation and progressively fragment to yield individual platelets. In a healthy adult, the normal platelet count is 150,000 to 450,000/mm3 (150–450 109 /L). Clinical and Laboratory Manifestations Sepsis-associated thrombocytopenia is multifactorial in origin. In experimental models of sepsis, platelets adhere to activated endothelium in multiple organs.43,44 Following adhesion, activated platelets may either dislodge and return to the circulation or release their granule contents and undergo irreversible aggregation with viscous metamorphosis. Inflammatory mediators and bacterial products such as endotoxin can contribute to sepsis-associated thrombocytopenia by enhancing platelet reactivity and adhesivity.45 Phagocytosis of platelets by reticuloendothelial elements may also contribute to the cytopenias of sepsis. Microscopy of bone marrow aspirates of patients with sepsis often demonstrates hemophagocytic histiocytes.46 In a prospective study of 50 patients with sepsis and thrombocytopenia, hemophagocytosis was identified in 32 patients (64%). This process appears to be a function of elevated levels of macrophage-colony-stimulating factor and is correlated with the presence and extent of multiorgan dysfunction.47 However, a cause and effect relationship has not been demonstrated. Instead, hemophagocytosis of platelets may represent a mechanism through which nonpathogenic immunoglobulin bound to bacterial products on the surface of platelets is cleared.46 In some patients with sepsis, however, antibodies to specific platelet antigens such as GP IIb/IIIa or GP Ib/IX have been detected.48 Because similar antibodies have been implicated in the pathogenesis of immune thrombocytopenic purpura (ITP), these autoantibodies may contribute to sepsis-associated thrombocytopenia in some patients. Other Diagnostic Considerations HEPARIN-INDUCED THROMBOCYTOPENIA Critically ill patients, including those with severe sepsis, are often exposed to heparin administered for thromboprophylaxis or to maintain patency of indwelling lines or to coat vascular catheters. Although the prophylactic value of unfractionated heparin and its low-molecular weight derivatives has in general a very favorable benefit– risk profile, even minimal amounts of these drugs may induce heparin-induced thrombocytopenia (HIT) that may be mistaken for the thrombocytopenia of sepsis. Although thrombocytopenia can also be induced by other drugs (e.g., quinidine), HIT is unique because the thrombocytopenia can be associated with significant morbidity and mortality resulting from thrombosis. Two types of HIT have been identified. Type I HIT presents 1 to 4 days following heparin exposure in 10 to 20% of patients.49 The disorder is transient, non–immune mediated, and reversible despite ongoing heparin exposure. In general, patients with type I HIT are asymptomatic and platelet counts do not drop below 100 109 /L. On the other hand, type II HIT is a potentially fatal disorder that is associated with significant morbidity that may be confused with thrombotic DIC in a patient with severe sepsis. As an immune-mediated clinicopathological syndrome, it typically develops 5 to 14 days after heparin exposure—a time interval that can be as short as several hours in patients who have been recently exposed to the drug. Type II HIT develops in 1 to 5% of patients treated with unfractionated heparin, and in a much lower proportion of patients exposed to low molecular weight heparin (LMWH). Thrombocytopenia is more severe with platelet counts below 60 109 /L (although usually not below 20 109 /L) and unlike type I HIT, the thrombocytopenia persists for days after heparin has been discontinued. Paradoxically, bleeding in patients with HIT II is rare. Instead, 50% of patients present with arterial and venous thrombosis that may be isolated or develop in multiple vessels. The mortality and limb loss rate from amputation in patients with HIT II have each been estimated to be as high as 30%. Pathophysiologically, HIT II results from antibodies, predominantly immunoglobulin G (IgG), that develop in response to an antigen formed by a complex between platelet factor-4 (PF-4) and heparin. Binding of antibody to the PF-4-heparin complex induces platelet aggregation with thrombocytopenia and platelet activation with release of platelet microparticles, which are believed to be responsible for the thrombotic diathesis.50 When clinically suspected, HIT II should be treated accordingly. However, the diagnosis requires subsequent laboratory confirmation, preferably with both a functional assay of serotonin release from normal donor platelets exposed to patient plasma in the presence of heparin, and an assay for the presence of the PF-4heparin antibody; for example, by enzyme-linked immunosorbent assay (ELISA). In practice, the ELISA assay (which has a moderately high sensitivity with low specificity) is widely used as a screening test, whereas the ‘‘gold standard’’ serotonin release assay is offered by relatively few laboratories. Treatment of confirmed cases of HIT II (with or without confirmed thrombosis) should include cessation of all heparin and administration of a direct thrombin inhibitor such as lepirudin or argatroban by continuous infusion. In Canada and Europe, danaparoid is another alternative agent that may be used. LMWH should be avoided because antibodies can cross-react with the PF-4–LMWH complex. Warfarin anticoagulation should be avoided until the platelet count has recovered to at least > 100 109 /L on antithrombin therapy because the drug may diminish circulating protein C levels in the short term, which may 651 652 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 in turn exacerbate the procoagulant state and result in venous limb gangrene.51 PSEUDOTHROMBOCYTOPENIA Pseudothrombocytopenia should be suspected when a low platelet count is reported by the clinical laboratory in a patient without clinical manifestations of thrombocytopenia or when other organ dysfunctions are absent. Artifactually low platelet counts may be due to several causes. They include platelet aggregation in finger-stick samples, giant platelets not recognized as thrombocytes by automated cell counters, platelet satellitosis, or platelet clumping. The latter is produced by the presence of anticoagulant-dependent platelet agglutinins.52 Although it is most commonly seen with EDTA, platelet clumping can also occur with other anticoagulants. HYPOPROLIFERATIVE THROMBOCYTOPENIA The bone marrow of some patients with severe sepsis and thrombocytopenia may be hypocellular with decreased numbers of megakaryocytes. Several processes can be responsible for hypoproliferative thrombocytopenia. For example, it may be a consequence of the effects of cytokines, drug-induced injury, preexisting disease, or an acute folic acid deficiency. OTHER CAUSES Thrombocytopenia due to accelerated platelet destruction may be due to immunologic or nonimmunologic causes in infected patients. Immunologic disorders producing thrombocytopenia can be autoimmune (e.g., collagen vascular disorders, drugs, etc.) or alloimmune (e.g., posttransfusion purpura). Nonimmunologic etiologies include microangiopathic disorders such as DIC and thrombotic thrombocytopenic purpura (TTP). Treatment Considerations As the platelet count progressively falls below 150 109 /L, the risk of bleeding increases; however, platelet counts above 60 109 /L enable patients to withstand most minor hemostatic challenges. Risk–benefit assessment should be employed when considering the administration of anticoagulants or drugs that impair platelet function when counts are less than 30 109 /L. Platelet counts below 20 109 /L can be accompanied by petechiae, ecchymoses, epistaxis, and serious internal bleeding. The relationships between platelet count and bleeding risk are largely derived from observations of patients with untreated acute leukemia in the early 1960s.53,54 Although no clear threshold for bleeding was identified, the percentage of days in which patients experienced thrombocytopenia-associated hemorrhage rose steadily after platelet counts dropped below a range of 20 109 /L to 50 109 /L. This ‘‘trigger’’ for prophylactic platelet transfusions of 20 109 /L was widely 2004 incorporated into clinical practice for patients with and without malignancy. Since that time, and due to the more accurate automated methods of determining platelet count and subsequent risk of spontaneous bleeding, most clinicians now use a threshold of < 10 109 /L to trigger prophylactic platelet transfusion in a nonbleeding, nonseptic patient with hypoproliferative thrombocytopenia. However, platelet counts of 15 to 20 109 /L are recommended in patients with concomitant fever or infection.55 During the study of treatment of patients with severe sepsis with activated protein C, the safety data were generated with platelet counts maintained above 30 109 /L. WATCHFUL WAITING A septic patient with a low absolute risk for thrombocytopenic bleeding with a stable platelet count of 20 109 /L may be carefully observed. However, other risk factors commonly associated with sepsis such as fever, increased platelet consumption, a declining platelet count, renal failure, and/or treatment with drugs that inhibit platelet function or an anticoagulant warrant prophylactic platelet transfusion. PLATELET TRANSFUSIONS Platelet transfusions remain the ‘‘gold standard’’ for the treatment of clinically significant thrombocytopenia. However, their use is associated with several complications, including pyrogenic reactions, allergic reactions, and disease transmission.56 In fact, the risk of transmission of viral diseases is the same as that associated with transfusion of a single unit of PRBCs (in the case of a single donor platelet pheresis unit) or five to eight donor exposures (in the case of pooled random donor platelets). One unit of platelets contains the number of platelets in a unit of fresh whole blood in a volume of 50 mL. In the absence of a consumptive process (e.g., fever, DIC, bleeding, or alloimmunization) or sequestration (e.g., splenomegaly), one unit of platelets should increase the platelet count by 10 109 /L/m2 ( 7 109 /L in a 70 kg adult). A pheresis pack contains the equivalent of 6 to 10 units of platelets, and is obtained from a single donor by platelet pheresis. In general, one platelet pheresis pack will increase the platelet count of a stable 70 kg adult by 60 109 /L. ALTERATIONS OF THE HEMOSTATIC SYSTEM IN SEPSIS Pathophysiology and Background The coagulopathy of sepsis results from the effects of cytokines, bacterial products, and in some cases, direct endothelial cell injury. In addition to the thrombocytopenia described earlier, hemostatic changes of sepsis-induced coagulopathy include prothrombotic HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL manifestations and impairment of the body’s natural fibrinolytic potential. ACTIVATION OF PROCOAGULANT PATHWAYS The initial step in the coagulopathy of sepsis involves activation of the tissue factor pathway of coagulation (formerly known as the ‘‘extrinsic pathway’’). Tumor necrosis factor and IL-1 are believed to play a crucial role in the activation of coagulation during sepsis. Animal models of sepsis have established that enhanced TF expression occurs in vivo, and that blockade of its procoagulant activity prevents the development of coagulopathy, organ dysfunction, and death.57–60 The primary role of the contact pathway in sepsis is probably to activate fibrinolysis and generate vasoactive kinins.61,62 Although multiple cytokines (TNFa, IL-1a, IL1-b, IL-6, IL-8) and endotoxin itself are capable of upregulating TF synthesis by endothelial cells and monocytes in vitro, it has not been established that these cells are the dominant source of TF in vivo. Endotoxin and cytokineinduced activation of endothelial cell TF synthesis ia another possibility, although detectable expression of TF was limited to splenic endothelium in animals dying from Escherichia coli sepsis.63 While inhibitors targeted at enzymes ‘‘downstream’’ from TF/VIIa (such as factor Xa and thrombin) are capable of inhibiting the coagulopathic response, they do not prevent organ damage or death.64 Laboratory changes associated with this prothrombotic diathesis include elevated levels of prothrombin (PT) fragment F1.2 and increased concentrations of thrombin-antithrombin (TAT) complexes. PT fragment F1.2 is a peptide that is cleaved when PT is converted to thrombin; elevated plasma levels of PT fragment F1.2 are evidence of a prothrombotic diathesis. Increased TAT complexes result from binding and inactivation of thrombin by circulating antithrombin. Because D-dimers are formed by plasmin-mediated cleavage of cross-linked fibrin, elevated levels of Ddimer also support the presence of enhanced intravascular activation of the coagulation system. receptor (EPCR) and circulating protein S, protein C is converted to its active form and exerts several antiinflammatory, antithrombotic, and profibrinolytic properties. Levels of protein C decrease 12 hours (median) before the onset of the clinical symptoms of severe sepsis and septic shock and are low in more than 90% of patients with severe sepsis.65,66 The Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial demonstrated that treatment with recombinant human APC (rhAPC), drotrecogin alfa (activated), significantly decreases all-cause 30-day mortality in patients with severe sepsis.33 Failure of clinical trials to demonstrate that either AT or TFPI can improve outcomes in patients with severe sepsis suggests that drotrecogin alfa (activated) not only possesses antithrombotic properties but also modulates endothelial cell function—a property supported by experimental evidence.67,68 TNF-a and IL-1 have been shown to downregulate endothelial TM and EPCR expression in vitro. EPCR, which binds to protein C, enhances thrombinTM dependent activation of protein C. Whether impairment of protein C activation on the endothelial cell surface actually occurs in vivo during sepsis has only recently been studied, but the data do not allow a firm conclusion to be drawn. In meningococcemia, decreased immunohistochemical expression of TM and EPCR in the microvasculature of purpuric skin biopsy specimens has been demonstrated. These findings were interpreted to indicate that protein C activation is impaired, a conclusion supported by in vivo data in two patients treated with protein C concentrate.69 However, a recent post hoc analysis of data from the PROWESS study, in which the ratio of plasma concentrations of zymogen protein C to APC was measured in individuals with severe sepsis, suggested that the ability to activate protein C may be quite variable.70 Some individuals had no apparent defect in protein C activation because their elevated APC levels mirrored the plasma levels of thrombin (measured indirectly as F1.2). Others had lower APC levels than expected for the F1.2 levels, likely indicative of a relative failure to activate protein C.71 DOWNREGULATION OF ANTICOAGULANT PATHWAYS The body possesses several natural antithrombotic proteins that modulate hemostasis and help to localize coagulation to areas of tissue injury. They include antithrombin (AT), tissue factor pathway inhibitor (TFPI), and activated protein C (APC). Antithrombin inactivates several serine proteases formed during coagulation and is the substrate required for heparin to exert its anticoagulant activity. TFPI first binds and inactivates factor Xa; subsequently, the TFPI-Xa complex inhibits factor VIIa within the factor VIIa/ TF complex. Protein C is a vitamin K-dependent zymogen synthesized in the liver. APC is formed from protein C by thrombin bound to TM, an endothelial cell transmembrane protein. In concert with the endothelial protein C INHIBITION OF FIBRINOLYSIS Inhibition of fibrinolysis promotes persistence of microvascular clots, a consequence that may significantly impair oxygen delivery and lead to organ dysfunction. Experimental animal and human models of sepsis have demonstrated an early and transient activation of fibrinolysis, probably due to release of plasminogen activators, followed by prolonged inhibition. This inhibition is probably explained by a sustained TNFa, IL-1, and lipopolysaccharide-mediated stimulation of plasminogen activator inhibitor-1 (PAI-1) synthesis by endothelium and monocytes, and is independent of the coagulation response. In meningococcemia, higher PAI-1 levels have been shown to correlate with the 653 654 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 development of septic shock rather than meningitis, and a higher risk of death. Furthermore, PAI-1 levels are at least partly genetically determined, with higher values identified in individuals homozygous for the 4G/4G polymorphism of the PAI-1 gene.72,73 These clinical observations agree with in vitro experiments using cultured cell lines, in which basal and inducible levels of PAI-1 are higher in cell lines expressing this polymorphism. A similar observation regarding the prognostic relevance of inhibited fibrinolysis in nonmeningococcal sepsis has been presented.74 Clinical and Laboratory Manifestations A sepsis-associated coagulopathy is a sign of dysfunction of the hematologic organ system. In the Ibuprofen in Sepsis Trial, a coagulopathy with elevated levels of Ddimer and decreased levels of protein C was almost universal in patients with severe sepsis (Fig. 2).66 The coagulopathy in patients with this disease is linked to endothelial cell dysfunction and fibrin deposition, pathological processes that contribute to multiple organ system dysfunction and death. For example, involvement of the pulmonary vasculature is a prominent pathological manifestation of pulmonary dysfunction in patients with severe sepsis and ARDS.75,76 The first manifestations occur at the level of the endothelial cell and include increased capillary permeability. Diffuse alveolar damage subsequently follows and bronchoalveolar lavage at this time demonstrates the presence of procoagulants and decreased fibrinolytic activity. Vascular lesions correlate with the temporal phase of diffuse alveolar damage and include thrombotic, fibroproliferative, and obliterative changes. 2004 sepsis. Therefore, it may be important to differentiate sepsis-associated coagulopathy from overt DIC. Although there is no single clinical manifestation or laboratory value that is diagnostic of overt DIC, the following changes are reasonably consistent with the diagnosis: (1) presence of a disorder that is known to be linked with DIC (such as severe sepsis), (2) mucocutaneous bleeding and dysfunction of one or more organ systems, and (3) ongoing consumption of platelets and coagulation factors. The first two criteria are detected by clinical examination, whereas the third will be manifest as thrombocytopenia and/or prolongation of one or more global tests of coagulation. On behalf of the International Society of Thrombosis and Haemostasis, Taylor et al have proposed a scoring system for the diagnosis of DIC77 (Table 1). This system utilizes the features already described to provide a DIC score; values 5 are characteristic of DIC. Currently, the prognostic value of this system is undergoing prospective validation. SEVERE LIVER DISEASE Severe liver disease can produce alterations in the hemostatic system that can resemble sepsis coagulopathy or DIC. In fact, in the absence of clinical features it is difficult to differentiate the two disorders with hemostatic assays alone. Patients with severe liver disease may have hematologic changes similar to those of severe sepsis including anemia, thrombocytopenia, and elevated PT and aPTT values. Results of factor VII and VIII functional assays can assist in the differential diagnosis. Metabolic alterations in severe liver disease usually result in a low level of factor VII and increased concentrations of factor VIII. Because factor VIII is consumed during clotting, patients with severe sepsis and a coagulopathy, on the other hand, are more likely to have decreased concentrations of factor VIII.78,79 Diagnostic Considerations DISSEMINATED INTRAVASCULAR COAGULATION Thrombocytopenia, prolongation of the PT and/or activated partial thromboplastin time (aPTT) or any combination thereof is common in patients with severe General Treatment Considerations In the absence of bleeding, patients with severe sepsisassociated coagulopathy can simply be monitored. In most instances, once the infection is controlled the Figure 2 Coagulopathy is common in patients with severe sepsis. Note that elevated D-dimers and decreased levels of protein C are present in the great majority of patients with the disease. Classical markers of disseminated intravascular coagulation occur in only 20% of patients with the disease. (Illustration courtesy of the National Initiative in Sepsis Education.) HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL Table 1 Scoring Criteria for Overt Disseminated Intravascular Coagulation73 Does the patient have severe sepsis or another disorder known to be associated with DIC?. If so, proceed to scoring global coagulation test results and calculate score Parameter Score PLATELET COUNT 0 > 100,000/mm3 (> 100 109 /L) 1 3 2 9 < 100,000/mm (< 100 10 /L) 3 9 < 50,000/mm (< 50 10 /L) ELEVATED MARKER OF FIBRIN DEGRADATION* 0 No increase 1 Moderate increase Strong increase 2 PROLONGED PROTHROMBIN TIME 0 < 3 seconds 1 > 3 seconds and < 6 seconds 2 > 6 seconds FIBRINOGEN CONCENTRATION 0 > 100 mg/dL (> 1.0 g/L) 1 < 100 mg/dL (< 1.0 g/L) *D-dimers, fibrin split products (FSPs), fibrin degradation products (FDPs). Scores of 5 or more are compatible with overt DIC and should be followed on a daily basis. Scores < 5 are suggestive of nonovert DIC or another disorder and should be repeated in the next 1–2 days or as clinically indicated. abnormal laboratory parameters return toward normal. In patients who are bleeding despite active treatment of their infection, a careful examination should be conducted to rule out a discrete and correctable anatomic lesion (e.g., peptic ulcer) as the cause of the bleed. If bleeding is from multiple sites, treatment is that of DIC and is generally subdivided into three general areas: (1) treatment of the primary disease, (2) platelets and coagulation factor replacement, and (3) antithrombotics. Platelet transfusions are often used to maintain the platelet count above 20 109 /L, though the risk of spontaneous bleeding in the absence of anticoagulants usually occurs at platelet counts below 10 to 20 109 /L. Platelets should be administered to patients with thrombocytopenia who are bleeding. Low-dose unfractionated heparin has been used in the past to interrupt the vicious cycle of accelerated activation of coagulation, thrombosis, and factor depletion in patients with DIC. However, its efficacy has not been demonstrated in large-scale, randomized clinical trials.80 Fibrinolytic inhibitors are also not recommended in patients with severe sepsis and DIC because they may convert a hemorrhagic form of DIC to a microvascular thrombotic form with worsened end organ perfusion. Drotrecogin Alfa (Activated) Treatment-Related Considerations Practice guidelines from the Surviving Sepsis Campaign, an international collaboration of professional societies whose members are involved in the treatment of severe sepsis, have recently strongly endorsed the administration of drotrecogin alfa (activated) to patients with severe sepsis at high risk of death.81 Consequently, we will briefly review hematologic issues related to drotrecogin alfa (activated) administration. BLEEDING As an antithrombotic agent, drotrecogin alfa (activated) is associated with an increased risk of bleeding. In the PROWESS trial, serious bleeding was reported in 2.0% of placebo recipients and 3.5% of subjects who were treated with the drug.35 Risk factors for bleeding include platelet counts < 30 109 /L; concomitantly administered medications that increase the risk of bleeding such as GP IIb/IIIa inhibitors, oral anticoagulants, therapeutic (not thromboprophylactic) doses of heparin; surgical interventions; and other disorders that increase the risk of bleeding in any candidate for systemic anticoagulation or thrombolysis. Importantly, the increased rate of bleeding in patients treated with drotrecogin alfa (activated) is primarily procedure-related and predominantly develops during drug infusion. Because of its short halflife, there is no significant residual drug effect if the infusion is temporarily interrupted 2 hours prior to any surgical procedure. The decision as to when to restart the infusion should be based upon the nature of the procedure and assessment of the patient.82 Cases of intracranial hemorrhage, a potentially life-threatening complication, are rare and are most often associated with platelet counts < 30 109 /L or meningitis. USE IN PATIENTS WITH DIC A study by Aoki et al reported that low-dose rhAPC corrected the clinical and laboratory abnormalities in patients with DIC more effectively than unfractionated heparin.83 The 28-day all-cause mortality rates in patients treated with APC and heparin were 20.4% and 40%, respectively (p < 0.05). In addition, patients treated with APC had significantly less bleeding (p ¼ 0.009). Joyce et al performed a retrospective subgroup analysis to determine the effect of drotrecogin alfa (activated) in patients with severe sepsis and DIC.84 Treatment with drotrecogin alfa (activated) produced a 42% reduction in the relative risk of death compared with placebo (95% confidence interval: 58 to 19). USE IN THE ELDERLY The incidence of sepsis and associated mortality increases significantly with age. As pointed out by Ely et al, there are age-related inflammatory and coagulopathic changes that may increase vulnerability of older patients to sepsis-associated hematologic changes and adverse outcomes.85 Advancing age is accompanied by both prothrombotic and impaired fibrinolytic activity. In a comparative study of healthy centenarians with healthy 655 656 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 adult controls, hypercoagulability could be identified in the very elderly by significant increases in coagulation factor VIIa, activation peptides of factors IX and X, F1.2, and TAT complexes.86 These changes are accompanied by a balanced and significant increase in fibrinolytic activity reflected in elevated D-dimers and plasmin– antiplasmin complexes. These hemostatic alterations may be linked to increased frailty and functional impairment in the elderly.87 Further activation of the hemostatic system of the aged can be produced by bacterial products released during sepsis. Yamamoto et al have demonstrated experimentally that with age there is enhanced lipopolysaccharide signaling.88 The result may be increased levels of inflammatory cytokines and upregulation of the PAI1 gene. When the hemostatic alterations of advanced age are coupled with the coagulopathy of sepsis, the elderly population is placed at significant increased risk for mortality. Ely et al evaluated the short- and long-term outcomes of drotrecogin alfa (activated) therapy of 386 adult PROWESS enrollees aged 75 years and older with severe sepsis.85 Subjects treated with drotrecogin alfa (activated) had absolute risk reductions in 28-day and in-hospital mortality of 15.5% and 15.6%, respectively (for both), compared with placebo recipients (p ¼ 0.002). Long-term follow-up data indicated that survival rates for patients treated with drotrecogin alfa (activated) recipients were significantly higher over a 2-year period (p ¼ 0.02). The incidences of serious bleeding events during the 28-day study period were 3.9% and 2.2% (p ¼ 0.34), slightly higher than the overall PROWESS population. However, there was no interaction between age and bleeding rates (p ¼ 0.97). Presumably as a result of the drug’s antithrombotic properties, elderly patients treated with drotrecogin alfa (activated) had significantly fewer thrombotic events than controls (p ¼ 0.019). In the presence of a favorable benefit/risk profile, this study supports the use of the drug in the elderly at high risk of death when the patient, family, and health care team have chosen aggressive care. 2004 Because drotrecogin alfa (activated) inactivates coagulation factors Va and VIIIa, treatment has been shown to prolong the aPTT by a mean of 7 seconds. The PT tests the tissue factor and final common pathways of coagulation. Inactivation of factor Va by the drug can lead to a prolongation of the PT. However, in the PROWESS enrollees, a median of only 1 second separated the placebo and intervention groups. Therefore, the PT cannot be expected to be an accurate surrogate of drug effect. In the PROWESS trial, drotrecogin alfa (activated) benefited patients with normal and depressed levels of protein C. Following treatment with the drug, levels of zymogen protein C increased in PROWESS enrollees, reflecting restoration of homeostasis. Antithrombin is consumed during the coagulopathy of sepsis. Treatment with drotrecogin alfa (activated) also increased levels of this natural antithrombotic protein. However, clinical benefit from drotrecogin alfa (activated) was seen even in subjects with normal baseline AT activity. Thus there is no scientific basis to assay protein C or AT levels to stratify patients for treatment or to monitor therapy. The antithrombotic properties of drotrecogin alfa (activated) produce significant improvements in sepsis-associated elevations of the markers of intravascular thrombin generation such as concentrations of PT fragment F1.2 and TAT complexes. Analogously therefore, routine assay of these substances is not indicated or clinically useful. CONCLUSIONS The hematologic organ system is a central player in the clinical manifestations of sepsis, sepsis pathophysiology, and recovery from sepsis. Identification of hematologic organ dysfunction in a patient with two or more SIRS criteria and infection indicates that the diagnosis is severe sepsis. Knowledge of the hematologic manifestations of sepsis can improve diagnosis and therapy of patients with this common and frequently fatal disorder. FINANCIAL SUPPORT EFFECT OF DROTRECOGIN ALFA (ACTIVATED) ON TESTS OF HEMOSTASIS There is no need to monitor drotrecogin alfa (activated) therapy with tests of hemostasis including protein C assays. However, because both the sepsis coagulopathy and the drug can alter routine tests of hemostasis, relevant drug-related effects on coagulation parameters are briefly described.82 Drotrecogin alfa (activated) has no direct effect on platelet counts; however, because the drug restores homeostasis, treatment can be accompanied by decreased platelet consumption and restoration of platelet counts into the normal range. The aPTT tests the contact (intrinsic) and final common pathways of coagulation. Dr. Ely is a recipient of the Paul Beeson Faculty Scholar Award from the Alliance for Aging Research. He is a recipient of a K23 from the National Institute of Health (#AG01023–01A1) and is the Associate Director of Research for the VA Tennessee Valley Geriatric Research and Education Clinical Center (GRECC). No other external funding was provided. REFERENCES 1. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303–1310 HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL 2. Aird WC. The hematologic system as a marker of organ dysfunction in sepsis. Mayo Clin Proc 2003;78:869–881 3. Sporn L, Huber P. Endothelial cell biology. In Colman RW, Hirsh J, Marder VJ, Clowes AW, George JN, eds. Hemostasis and Thrombosis. Philadelphia: Lippincott: Williams & Wilkins; 2001 4. Hack CE, Zeerleder S. The endothelium in sepsis: source of and a target for inflammation. Crit Care Med 2001; 29(7 Suppl):S21–S27 5. Esmon CT. The normal role of activated protein C in maintaining homeostasis and its relevance to critical illness. Crit Care 2001;5:S7–12 6. Leclerc J, Pu Q, Corseaux D, et al. A single endotoxin injection in the rabbit causes prolonged blood vessel dysfunction and a procoagulant state. Crit Care Med 2000;28:3672–3678 7. Vincent JL. Microvascular endothelial dysfunction: a renewed appreciation of sepsis pathophysiology. Crit Care 2001;5: S1–S5 8. Reinhart K, Bayer O, Brunkhorst F, Meisner M. Markers of endothelial damage in organ dysfunction and sepsis. Crit Care Med 2002;30(5 Suppl):S302–S312 9. Krafte-Jacobs B, Brilli R. Increased circulating thrombomodulin in children with septic shock. Crit Care Med 1998;26: 933–938 10. Moss M, Gillespie MK, Ackerson L, Moore FA, Moore EE, Parsons PE. Endothelial cell activity varies in patients at risk for the adult respiratory distress syndrome. Crit Care Med 1996;24:1782–1786 11. Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med 2003;348:138–150 12. Baskurt OK, Gelmont D, Meiselman HJ. Red blood cell deformability in sepsis. Am J Respir Crit Care Med 1998;157: 421–427 13. Langenfeld JE, Livingston DH, Machiedo GW. Red cell deformability is an early indicator of infection. Surgery 1991; 110:398–403; discussion 403–404 14. Baskurt OK, Temiz A, Meiselman HJ. Red blood cell aggregation in experimental sepsis. J Lab Clin Med 1997;130: 183–190 15. van Iperen CE, Gaillard CA, Kraaijenhagen RJ, Braam BG, Marx JJ, van de Wiel A. Response of erythropoiesis and iron metabolism to recombinant human erythropoietin in intensive care unit patients. Crit Care Med 2000;28:2773–2778 16. Zimmerman JE, Seneff MG, Sun X, Wagner DP, Knaus WA. Evaluating laboratory usage in the intensive care unit: patient and institutional characteristics that influence frequency of blood sampling. Crit Care Med 1997;25:737–748 17. Vincent JL, Baron JF, Reinhart K, et al. Anemia and blood transfusion in critically ill patients. JAMA 2002;288:1499– 1507 18. Smoller BR, Kruskall MS. Phlebotomy for diagnostic laboratory tests in adults: pattern of use and effect on transfusion requirements. N Engl J Med 1986;314:1233–1235 19. Olivares M, Walter T, Osorio M, Chadud P, Schlesinger L. Anemia of a mild viral infection: the measles vaccine as a model. Pediatrics 1989;84:851–855 20. Krantz SB. Pathogenesis and treatment of the anemia of chronic disease. Am J Med Sci 1994;307:353–359 21. Andrews NC. Disorders of iron metabolism. N Engl J Med 1999;341:1986–1995 22. Shurin SB, Anderson P, Zollinger J, Rathbun RK. Pathophysiology of hemolysis in infections with Hemophilus influenzae type b. J Clin Invest 1986;77:1340–1348 23. Su D, Roth RI, Levin J. Hemoglobin infusion augments the tumor necrosis factor response to bacterial endotoxin (lipopolysaccharide) in mice. Crit Care Med 1999;27:771–778 24. Corwin HL, Parsonnet KC, Gettinger A. RBC transfusion in the ICU: is there a reason? Chest 1995;108:767–771 25. Gazmuri RJ, Shakeri SA. Blood transfusion and the risk of nosocomial infection: an underreported complication? Crit Care Med 2002;30:2389–2391 26. Goodnough LT, Brecher ME, Kanter MH, AuBuchon JP. Transfusion medicine: first of two parts–blood transfusion. N Engl J Med 1999;340:438–447 27. Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999;340:409–417 28. Corwin HL, Gettinger A, Pearl RG, et al. Efficacy of recombinant human erythropoietin in critically ill patients: a randomized controlled trial. JAMA 2002;288:2827–2835 29. Russell JA. Adding fuel to the fire: the supranormal oxygen delivery trials controversy. Crit Care Med 1998;26:981–983 30. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001;345:1368–1377 31. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992;101:1644–1655 32. Medzhitov R, Janeway C Jr. Innate immunity. N Engl J Med 2000;343:338–344 33. Funke A, Berner R, Traichel B, Schmeisser D, Leititis JU, Niemeyer CM. Frequency, natural course, and outcome of neonatal neutropenia. Pediatrics 2000;106(1 Pt 1):45–51 34. Root RK, Lodato RF, Patrick W, et al. Multicenter, doubleblind, placebo-controlled study of the use of filgrastim in patients hospitalized with pneumonia and severe sepsis. Crit Care Med 2003;31:367–373 35. Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001;344:699–709 36. Warren BL, Eid A, Singer P, et al. Caring for the critically ill patient: high-dose antithrombin III in severe sepsis: a randomized controlled trial. JAMA 2001;286:1869–1878 37. Baughman RP, Lower EE, Flessa HC, Tollerud DJ. Thrombocytopenia in the intensive care unit. Chest 1993; 104:1243–1247 38. Stephan F, Hollande J, Richard O, Cheffi A, MaierRedelsperger M, Flahault A. Thrombocytopenia in a surgical ICU. Chest 1999;115:1363–1370 39. Vanderschueren S, De Weerdt A, Malbrain M, et al. Thrombocytopenia and prognosis in intensive care. Crit Care Med 2000;28:1871–1876 40. Nijsten MW, ten Duis HJ, Zijlstra JG, Porte RJ, Zwaveling JH, Paling JC. The TH: blunted rise in platelet count in critically ill patients is associated with worse outcome. Crit Care Med 2000;28:3843–3846 41. Long MW. Thrombopoietin stimulation of hematopoietic stem/progenitor cells. Curr Opin Hematol 1999;6:159–163 42. Cramer EM. Megakaryocyte structure and function. Curr Opin Hematol 1999;6:354–361 43. Shibazaki M, Kawabata Y, Yokochi T, Nishida A, Takada H, Endo Y. Complement-dependent accumulation and 657 658 SEMINARS IN RESPIRATORY AND CRITICAL CARE MEDICINE/VOLUME 25, NUMBER 6 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. degradation of platelets in the lung and liver induced by injection of lipopolysaccharides. Infect Immun 1999;67:5186–5191 Tsujikawa A, Kiryu J, Yamashiro K, et al. Interactions between blood cells and retinal endothelium in endotoxic sepsis. Hypertension 2000;36:250–258 Salat A, Murabito M, Boehm D, et al. Endotoxin enhances in vitro platelet aggregability in whole blood. Thromb Res 1999; 93:145–148 Stephan F, Thioliere B, Verdy E, Tulliez M. Role of hemophagocytic histiocytosis in the etiology of thrombocytopenia in patients with sepsis syndrome or septic shock. Clin Infect Dis 1997;25:1159–1164 Francois B, Trimoreau F, Vignon P, Fixe P, Praloran V, Gastinne H. Thrombocytopenia in the sepsis syndrome: role of hemophagocytosis and macrophage colony-stimulating factor. Am J Med 1997;103:114–120 Stephan F, Cheffi MA, Kaplan C, et al. Autoantibodies against platelet glycoproteins in critically ill patients with thrombocytopenia. Am J Med 2000;108:554–560 Brieger DB, Mak KH, Kottke-Marchant K, Topol EJ. Heparin-induced thrombocytopenia. J Am Coll Cardiol 1998;31:1449–1459 Warkentin TE, Hayward CP, Boshkov LK, et al. Sera from patients with heparin-induced thrombocytopenia generate platelet-derived microparticles with procoagulant activity: an explanation for the thrombotic complications of heparininduced thrombocytopenia. Blood 1994;84:3691–3699 Warkentin TE, Elavathil LJ, Hayward CP, Johnston MA, Russett JI, Kelton JG. The pathogenesis of venous limb gangrene associated with heparin-induced thrombocytopenia. Ann Intern Med 1997;127:804–812 Berkman N, Michaeli Y, Or R, Eldor A. EDTA-dependent pseudothrombocytopenia: a clinical study of 18 patients and a review of the literature. Am J Hematol 1991;36:195–201 Gaydos LA, Freireich EJ, Mantel N. The quantitative relation between platelet count and hemorrhage in patients with acute leukemia. N Engl J Med 1962;266:905–909 Rinder HM, Arbini AA, Snyder EL. Optimal dosing and triggers for prophylactic use of platelet transfusions. Curr Opin Hematol 1999;6:437–441 Drews RE. Critical issues in hematology: anemia, thrombocytopenia, coagulopathy, and blood product transfusions in critically ill patients. Clin Chest Med 2003;24:607–622 Triulzi D. Optimizing Platelet Transfusion Therapy. Baltimore, MD: Institute for Transfusion Medicine; 1997 Osterud B, Bjorklid E. The tissue factor pathway in disseminated intravascular coagulation. Semin Thromb Hemost 2001;27:605–617 Taylor FB Jr, Chang A, Ruf W, et al. Lethal E. coli septic shock is prevented by blocking tissue factor with monoclonal antibody. Circ Shock 1991;33:127–134 Creasey AA, Chang AC, Feigen L, Wun TC, Taylor FB Jr, Hinshaw LB. Tissue factor pathway inhibitor reduces mortality from Escherichia coli septic shock. J Clin Invest 1993;91:2850– 2860 Taylor FB, Chang AC, Peer G, Li A, Ezban M, Hedner U. Active site inhibited factor VIIa (DEGR VIIa) attenuates the coagulant and interleukin-6 and -8, but not tumor necrosis factor, responses of the baboon to LD100 Escherichia coli. Blood 1998;91:1609–1615 Pixley RA, De La Cadena R, Page JD, et al. The contact system contributes to hypotension but not disseminated intravascular coagulation in lethal bacteremia: in vivo use of 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 2004 a monoclonal anti-factor XII antibody to block contact activation in baboons. J Clin Invest 1993;91:61–68 van der Poll T, de Jonge E, Levi M. Regulatory role of cytokines in disseminated intravascular coagulation. Semin Thromb Hemost 2001;27:639–651 Drake TA, Cheng J, Chang A, Taylor FB Jr. Expression of tissue factor, thrombomodulin, and E-selectin in baboons with lethal Escherichia coli sepsis. Am J Pathol 1993;142:1458–1470 Taylor FB Jr, Chang AC, Peer GT, et al. DEGR-factor Xa blocks disseminated intravascular coagulation initiated by Escherichia coli without preventing shock or organ damage. Blood 1991;78:364–368 Mesters RM, Helterbrand J, Utterback BG, et al. Prognostic value of protein C concentrations in neutropenic patients at high risk of severe septic complications. Crit Care Med 2000; 28:2209–2216 Yan SB, Helterbrand JD, Hartman DL, Wright TJ, Bernard GR. Low levels of protein C are associated with poor outcome in severe sepsis. Chest 2001;120:915–922 Yan SB, Dhainaut JF. Activated protein C versus protein C in severe sepsis. Crit Care Med 2001;29(7 Suppl):S69–S74 Cheng T, Liu D, Griffin JH, et al. Activated protein C blocks p53-mediated apoptosis in ischemic human brain endothelium and is neuroprotective. Nat Med 2003;9:338–342 Faust SN, Levin M, Harrison OB, et al. Dysfunction of endothelial protein C activation in severe meningococcal sepsis. N Engl J Med 2001;345:408–416 Dhainaut JF, Yan SB, Margolis BD, et al. Drotrecogin alfa (activated) (recombinant human activated protein C) reduces host coagulopathy response in patients with severe sepsis. Thromb Haemost 2003;90:642–653 Liaw P, Ferrell G, Loeb M, Foley R, Weitz J, Esmon CT. Patients with sepsis vary markedly in their ability to generate activated protein C [abstract]. Blood 2001;98:445a Hermans PW, Hibberd ML, Booy R, et al. 4G/5G promoter polymorphism in the plasminogen-activator-inhibitor-1 gene and outcome of meningococcal disease. Meningococcal Research Group. Lancet 1999;354:556–560 Westendorp RG, Hottenga JJ, Slagboom PE. Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococcal septic shock. Lancet 1999;354:561–563 Raaphorst J, Johan Groeneveld AB, Bossink AW, Erik Hack C. Early inhibition of activated fibrinolysis predicts microbial infection, shock and mortality in febrile medical patients. Thromb Haemost 2001;86:543–549 Tomashefski JF Jr. Pulmonary pathology of the adult respiratory distress syndrome. Clin Chest Med 1990;11:593–619 Hasegawa N, Husari AW, Hart WT, Kandra TG, Raffin TA. Role of the coagulation system in ARDS. Chest 1994;105: 268–277 Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost 2001;86:1327–1330 Mammen EF. Coagulation abnormalities in liver disease. Hematol Oncol Clin North Am 1992;6:1247–1257 Clarke BJ, Sridhara S, Woskowska Z, Blajchman MA. Consumption of plasma factor VII in a rabbit model of nonovert disseminated intravascular coagulation. Thromb Res 2002;108:329–334 Feinstein DI. Diagnosis and management of disseminated intravascular coagulation: the role of heparin therapy. Blood 1982;60:284–287 HEMATOLOGIC CHANGES IN SEPSIS/GOYETTE ET AL 81. Dellinger RP, Carlet JM, Masur H, et al. Surviving sepsis campaign management guidelines committee. Surviving sepsis campaign guidelines for management of severe sepsis and septic shock. Crit Care Med 2004;32:858–873 82. Laterre PF, Heiselman D. Management of patients with severe sepsis, treated by drotrecogin alfa (activated). Am J Surg 2002;184(6A Suppl):S39–S46 83. Aoki N, Matsuda T, Saito H, et al. A comparative doubleblind randomized trial of activated protein C and unfractionated heparin in the treatment of disseminated intravascular coagulation. Int J Hematol 2002;75:540–547 84. Joyce D, Yan B, Basson BR, et al. Disseminated intravascular coagulation in severe sepsis patients treated with recombinant human activated protein C [abstract]. Blood 2001;98:445a 85. Ely EW, Angus DC, Williams MD, Bates B, Qualy R, Bernard GR. Drotrecogin alfa (activated) treatment of older patients with severe sepsis. Clin Infect Dis 2003;37:187– 195 86. Mari D, Mannucci PM, Coppola R, Bottasso B, Bauer KA, Rosenberg RD. Hypercoagulability in centenarians: the paradox of successful aging. Blood 1995;85:3144–3149 87. Cohen HJ, Harris T, Pieper CF. Coagulation and activation of inflammatory pathways in the development of functional decline and mortality in the elderly. Am J Med 2003;114:180–187 88. Yamamoto K, Shimokawa T, Yi H, et al. Aging accelerates endotoxin-induced thrombosis: increased responses of plasminogen activator inhibitor-1 and lipopolysaccharide signaling with aging. Am J Pathol 2002;161:1805–1814 659