Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
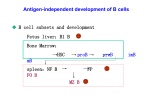
Birdshot Chorioretinopathy Long-term Manifestations and Visual Prognosis Aniki Rothova, MD, PhD,1 Tos T. J. M. Berendschot, PhD,1 Kiki Probst, MD,1 Bram van Kooij, MD,1 G. Seerp Baarsma, MD2 Purpose: To ascertain the clinical features and long-term visual prognosis of birdshot chorioretinopathy (BCR), and to identify patients at risk of visual loss. Design: Retrospective noncomparative case series. Participants: Fifty-five consecutive patients with HLA-A29 –positive BCR who were identified in ophthalmology departments of the University Medical Center of Utrecht and The Eye Hospital Rotterdam, of whom 37 were observed for at least 5 years. Intervention: A review of the medical and photographic and/or angiographic records of 55 patients with HLA-A29 –positive BCR. Main Outcome Measures: Numerous variables were compared, including age and gender distribution, onset and course of BCR, ocular manifestations, therapeutic strategies and their outcomes, complications, systemic diseases, visual acuity (VA), and features associated with poor visual outcome. Results: Loss of VA was gradual; the number of affected eyes with VA less than 20/200 increased from 9 of 108 (8%) at onset to 22 of 73 (30%) at 5 years and 19 of 49 (39%) at 10 years of follow-up. The cause of compromised VA was predominantly macular edema and macular atrophy (42 of 55 [76% of cases]). We found strong associations between the VA at onset and visual outcome after 5 and 10 years (P ⫽ 0.005 and P ⫽ 0.006, respectively). Mean VA at the 5-year follow-up was significantly lower if macular leakage was observed on angiography (P⬍0.001). No differences in annual loss of VA were observed between patients treated by standard therapeutic modalities and untreated patients. Conclusion: The visual prognosis of BCR in a spectrum of uveitis is poor, and the recommended therapeutic regimens have had no effect on long-term visual prognosis. New treatment strategies are needed for this blinding disorder. Ophthalmology 2004;111:954 –959 © 2004 by the American Academy of Ophthalmology. Birdshot chorioretinopathy (BCR) is a chronic intraocular inflammatory disease of unknown origin that is responsible for 1% to 2% of all uveitis cases.1– 4 The typical ocular features include bilateral vitreitis and multiple hypopigmented choroidal spots in the absence of severe anterior segment inflammation.5 Birdshot chorioretinopathy is strongly associated with HLA-A29 (98% in BCR, vs. 7% in the general population).5,6 Birdshot chorioretinopathy is predominantly considered to be an ocular disorder without systemic manifestations.5,7 Occasionally, systemic hypertension has been noted, and a small number of patients complained of hearing loss, vitiligo, and mood disorders.5,8 –10 The course of BCR is, in the majority of patients, chronic Originally received: April 28, 2003. Accepted: September 8, 2003. Manuscript no. 230274. 1 Uveitis Center, F. C. Donders Institute of Ophthalmology, University Medical Center of Utrecht, Utrecht, The Netherlands. 2 The Eye Hospital Rotterdam, Rotterdam, The Netherlands. Supported in part by the Dr. F. P. Fischer Foundation, Utrecht, The Netherlands. Correspondence to Aniki Rothova, MD, PhD, F. C. Donders Institute of Ophthalmology, University Medical Center, P.O. Box 85 500, 3508 GA Utrecht, The Netherlands. E-mail: [email protected]. 954 © 2004 by the American Academy of Ophthalmology Published by Elsevier Inc. and progressive. The recommended treatment consists of symptomatic administration of anti-inflammatory drugs and prevention and/or treatment of complications.5,9,10 In the past, several studies with variable follow-up periods have attempted to assess the prognosis of BCR; however, the results were contradictory. We report on the long-term visual prognosis of BCR and on clinical manifestations associated with this disorder in a cohort of 55 patients. Patients and Methods We conducted a retrospective analysis of the medical records of 72 consecutive patients with clinical features of BCR who consulted the ophthalmologic department of the University Medical Center of Utrecht and The Eye Hospital Rotterdam between 1990 and 2001. All patients underwent a complete clinical examination and the standard screening protocol for uveitis, which included determination of the erythrocyte sedimentation rate, red and white blood cell counts, glucose levels, and serum angiotensin-converting enzyme levels; serologic tests for syphilis; and chest radiography. Of 72 patients with a clinical diagnosis of BCR, 7 were HLA-A29 negative, considered as a separate group, and not included in this series. Ten patients were observed for less than 1 year or were seen only once for a second opinion. In the present study we included 55 HLA-A29 –positive BCR patients observed ISSN 0161-6420/04/$–see front matter doi:10.1016/j.ophtha.2003.09.031 Rothova et al 䡠 Birdshot Chorioretinopathy Table 1. Visual Acuity Data over Time in Birdshot Chorioretinopathy (Affected Eyes) Follow-up Baseline (N ⫽ 108) 1 Year (N ⫽ 98) 2 Years (N ⫽ 77) 5 Years (N ⫽ 73) 10 Years (N ⫽ 49) Visual Acuity N % N % N % N % N % ⱕ20/200 20/200–20/60 Totalⱕ20/60 9 12 21 8 11 19 14 10 24 14 10 24 18 8 26 23 10 33 22 10 32 30 14 44 19 9 28 39 18 57 for at least 1 year, of whom 48 were observed for 2 years, 37 for at least 5 years, and 25 for 10 years. The clinical diagnosis of BCR was based on criteria formulated by Vitale—in short, bilateral disease characterized by multiple deep choroidal creamy-white lesions combined with vitreitis without snowbanking in eyes with the absence of severe anterior segment inflammation.5,7–12 All patients were HLA-A29 positive. Visual acuity (VA) was measured using the Snellen chart projection unit. The testing distance was 6 m. Legal blindness was defined as a best-corrected VA of the affected eye of ⱕ20/200.13 Visual outcome was defined as the optimal VA at the 5- and 10-year follow-ups (not the worst VA at any visit or at a nonstandardized follow-up point). We compared numerous variables, including gender and age distributions, clinical systemic and ocular features, laboratory data, therapeutic strategies and their outcomes, complications, and VA, as well as possible risk factors for visual loss. Cardiovascular disease was considered present in patients with myocardial infarction, treated angina pectoris, deep systemic thrombosis, and cerebrovascular accident. For purposes of this study, patients with systemic hypertension were also included. Three patients with a temporary rise in blood pressure due to systemic medications were excluded. The SPSS statistical software package (10.0.7; SPSS Inc., Chicago, IL) was used for data analysis. Because left and right eyes cannot be assumed to be independent, we performed statistical analyses for left eyes only, for right eyes only, for the mean of the left and right eyes, and for the better seeing eye. All choices led to the same conclusions. Here we present the analysis performed on the mean of the left and right eyes. These are also the values shown in the figures. Before analysis, VA was always transformed to logarithm of the minimum angle of resolution acuity. Logarithm of the minimum angle of resolution is defined as the 10-base logarithm of the VA. We used Student’s t test to evaluate the differences in visual outcome between categorical variables like gender and treatments used. Analysis of variance was used to study differences in VA between variables such as age at onset and time to diagnosis. A general linear model with repeated measurements was used to study the progression of VA. We used the Pearson correlation coefficient for calculation of the correlation between VA values at onset and those at follow-up points. Chi-square tests were used to study possible associations between categorical variables. P values of ⬍0.05 were considered statistically significant. The approval of the local ethical committee was not needed for this retrospective study. Results In total, 26 females and 29 males were included in this study. All patients were Caucasian. Bilateral involvement was present in 54 of the patients; the remaining patient had undergone enucleation of one eye 10 years before the onset of BCR (due to uveal melanoma). One amblyopic eye with an optimal VA of 20/100 was not included in the analysis of visual outcome, which resulted in 108 affected eyes. Mean age at first presentation to the ophthalmologist with complaints of BCR was 53 years (median, 53; range, 23–75). Birdshot chorioretinopathy became manifest in patients above the age of 40 years in 46 of 55 (84%) patients. The average interval from presentation to the ophthalmologist to the diagnosis of BCR was 3 years (median, 2; range, 0 –20). At the onset of the disease, 9 of 108 (8%) affected eyes had a VA of less than 20/200; 12 of 108 (11%) had a VA of less than 20/60 but better than 20/200 (Table 1). None had a bilateral VA of less than 20/200, and 4 patients (7%) had a bilateral acuity of less than 20/60 (Table 2). Chorioretinal lesions adjacent to the optic disc (Fig 1) were noted in 19 of 47 (40%) patients. Visual acuity data over time are presented in Figures 2 and 3 and Tables 1 and 2. The decline of VA was gradual during the follow-up, and no changes between the initial and late periods were noted. Strong association between the VA at onset and visual outcome after 5 and 10 years was observed (P ⫽ 0.005 and P ⫽ 0.006, respectively; Fig 2). No difference in the progression of visual loss was identified between the eyes with good and poor outcomes (Fig 3). Also, no difference in visual outcome was found for gender, age at onset, time to diagnosis, and/or treatments used. At 5 years of follow-up, 22 of 73 (30%) affected eyes had a VA of ⱕ20/200, and 10 of 73 (14%) had one between 20/200 and 20/60 (Tables 1, 2). A bilateral VA of ⱕ20/200 was noted for 5 of 37 (14%) patients, and one between 20/200 and 20/60 was noted for Table 2. Visual Acuity Data over Time in Birdshot Chorioretinopathy (Patients with Bilateral Visual Loss) Follow-up Baseline (N ⫽ 55) 1 Year (N ⫽ 54) 2 Years (N ⫽ 39) 5 Years (N ⫽ 37) 10 Years (N ⫽ 25) Visual Acuity of Best Eye N % N % N % N % N % ⱕ20/200 20/200–20/60 Totalⱕ20/60 0 4 4 0 7 7 2 5 7 4 9 13 5 2 7 13 5 18 5 6 11 14 16 30 5 4 9 20 16 36 955 Ophthalmology Volume 111, Number 5, May 2004 Figure 1. Chorioretinal lesions adjacent to the optic disc in a patient with birdshot chorioretinopathy. 6 of 37 (16%). The cause of compromised VA was predominantly cystoid macular edema (CME) and/or retinochoroidal atrophy (specifically in 42 of 55 [76%] cases); the remaining cases were caused by glaucoma, retinal pucker, optic atrophy, and subretinal neovascularization. The mean VA at the 5-year follow-up was significantly lower if macular leakage on angiography was observed (P⬍0.001). Systemic immunosuppressive and immunomodulatory drugs were used in 36 of 55 cases (corticosteroids in 36; methotrexate in 6; cyclosporin A in 16; and miscellaneous in 7, including colchicine, plaquenil, azathioprine, nonsteroidal anti-inflammatory drugs, and infliximab). A combination of immunosuppressive drugs and corticosteroids was used in 25 cases, and corticosteroids alone in 11. Acetazolamide was given in 24 cases (in combination with anti-inflammatory drugs in 20 cases and as a monotherapy in 4). Fifteen patients had no systemic treatment. The annual loss of VA did not differ between the treated and untreated patients (Fig 4), and differences between specific types of treatments used or for the use of acetazolamide were not observed. The complications occurring at the 5-year follow-up are summarized in Table 3. Complications included CME in 31 of 37 patients (84%), cataract in 22 of 37 (60%), and glaucoma in 7 of 37 (19%). Visual fields (VFs) exhibited profound defects in all of 27 patients tested, and furthermore, 44% (12 of 27) showed unexpected central and/or peripheral VF remnants only. In the majority of patients, retinal vascular abnormalities were observed (attenuated retinal vessels in 83%, irregular veins in 72%, and arteriovenous filling time on fluorescein angiography longer than 10 seconds in 46% of patients). Lesions adjacent to the optic disc developed over the years in 25 of 35 (71%). Patients with this anomaly had lower VA at the 2- and 5-year follow-ups than those without (P ⫽ 0.02 and P ⫽ 0.03, respectively). (Sub)retinal neovascularization developed in 5 of 37 (14%) patients observed for at least 5 years. Of the 37 HLA-A29 –positive patients with BCR assessed at the 5-year follow-up, 1 had biopsy-proven sarcoidosis, 7 (19%) reported previous skin malignancy (1 had melanoma, and 6 had basal cell carcinoma), 1 had had a uveal melanoma in the past, and 6 had malignancies of various origins (mamma, lung, prostate, and bladder). Cardiovascular disease was present in 21 of 37 (58%) patients (including systemic hypertension in 17 of 37 [46%]). Of 37 patients with completed 5-year follow-up, 18 (49%) had cardiovascular disease present during the 5-year follow-up period. Of those, 8 developed bilateral VA loss, in contrast to 3 of 19 in those without cardiovascular disease during follow-up (P ⫽ 0.06). A bilateral VA of ⱕ20/200 was present in 4 of 6 patients with pre-existent cardiovascular disease, in contrast to 1 of 14 without cardiovascular disease (P ⫽ 0.04). Discussion This study reports on the visual prognosis of patients suffering from BCR and describes progressive loss of central VA over the years, caused predominantly by CME and/or Figure 2. Visual acuity (VA) data over time in birdshot chorioretinopathy, mean for all and divided according to baseline VA. Log Mar ⫽ logarithm of the minimum angle of resolution. 956 Rothova et al 䡠 Birdshot Chorioretinopathy Figure 3. Visual acuity (VA) data over time in birdshot chorioretinopathy, divided according to visual outcome at 10 years of follow-up. LogMar ⫽ logarithm of the minimum angle of resolution. macular atrophy. This process was not reversed by the anti-inflammatory treatments used. In addition, a high prevalence of vascular disease and skin malignancy was noted in BCR, a disease so far considered a purely ocular disorder. Long-term visual prognosis of BCR was repeatedly reported to be poor: 16% of BCR patients in Europe and 22% of BCR patients in the United States developed a VA of ⱕ20/200.7,10,12 Our series disclosed legal blindness (a bilateral VA of ⱕ20/200) in 14% and 20% of patients (after 5- and 10-year follow-ups, respectively), which is in concordance with previous literature. In contrast, legal blindness was reported to occur in 4% of all patients with uveitis.3 Of all the eyes in our study affected with BCR, 57% developed visual impairment (an acuity of ⱕ20/60), in contrast to 35% in a general uveitis population.3 The major cause of visual loss in uveitis was thought to be CME, and the frequent occurrence of CME in BCR (84%, vs. 30% in all with uveitis) might explain this excessive loss of vision.3 The prevalence of CME in BCR was previously reported in about half of patients, less than the 84% noted in our patients.5,7,12 The higher frequency found in this series might be explained by a uniform follow-up of 5 years in all of our patients. General characteristics of BCR noted in the previous reports included Caucasian race, middle age at onset, and bilateral ocular involvement, which is in concordance with our series.5,7,10,12 The slight female predominance (60%) described in previous studies was not noted by us (no gender preference found in this report). A prevalence of (sub)retinal neovascularization was previously reported in approximately 6% to 13%; in our series it was 14%.10,12,14 –17 Various studies have shown that BCR usu- Figure 4. Visual acuity data over time in birdshot chorioretinopathy and the use of systemic immunomodulatory and immunosuppressive treatment (corticosteroids, cyclosporin A, and methotrexate). LogMar ⫽ logarithm of the minimum angle of resolution. 957 Ophthalmology Volume 111, Number 5, May 2004 Table 3. Ocular Complications of Birdshot Chorioretinopathy (at 5 Years of Follow-up) Cystoid macular edema Cataract Glaucoma* (Sub)retinal neovascularization† Extensive visual defect (n ⫽ 28)‡ N ⴝ 37 % 31 22 7 (4)⫹1 11 84 60 19 14 39 *An additional 2 patients had ocular hypertension. † Four with subretinal and 1 with retinal neovascularization. ‡ Central and/or peripheral rest. ally remains active for approximately 10 to 12 years, and after that the active inflammation slowly declines, resulting in atrophic changes of the retina and optic disc.5,10,11,18 One study reported a self-limiting course in 20%.10 Although some authors argued that BCR is most severe during the first 2 to 4 years of activity and, in consequence, requires most aggressive treatment in this initial period of the disease, others report on a prolonged course with frequent remissions.19 Our findings favor the observation of chronic activity with a gradual visual loss over years.20 To date, no strong evidence exists with which to answer questions about the effectiveness of immunosuppressive medications in treating visual loss from BCR.5,7,9,10,12 The recommended treatment includes systemic and local steroids, cytotoxic and immunomodulatory agents, and their diverse combinations, and exact indications for treatment are not well defined.5,7,9,10,12,20 –22 Loss of VA (⬍20/40) and/or severe inflammation seen on fluorescein angiography were the usual indications for systemic anti-inflammatory treatment. It was recommended not to treat patients with a VA of higher than 20/40.9,10 Our results indicate that a more aggressive approach might be justified in view of the poor prognosis, especially in those with macular edema. Undoubtedly it is important to treat BCR (as all intraocular inflammations) during active inflammation, because the treatment of quiescent old scars is pointless.7 Intermittent treatment of exacerbations did not prevent visual loss.20 Whether the treatment of BCR during an early disease period is crucial for visual outcome is, however, not known. Visual complaints of BCR patients might seem out of proportion to the measured VA.5,10 Birdshot chorioretinopathy patients complain frequently of not having useful vision outside, abnormal color vision, and reading difficulties. Therefore, central VA alone is not the only parameter for treatment efficacy; VF examinations and electroretinogram might be extremely helpful parameters when assessing the degree of visual impairment and development of the disease. Visual fields and electroretinograms were pathologic even in BCR patients with full central acuity.10,20,23–25 In general, BCR occurs in healthy individuals, but cardiovascular disease (specifically, systemic hypertension) was previously noted in 20% to 23%.10,12,14 In our series, the prevalence of hypertension was 46% at the 5-year follow-up, compared with an estimated lifetime prevalence of 44%.26 In the Dutch population older than 55 years, 31% to 39% suffer from hypertension.27,28 We suggest that the 958 presence of cardiovascular disease—specifically, hypertension—might negatively influence visual prognosis in BCR patients. But the questions of whether the presence of cardiovascular disease really affects the long-term visual outcome of patients with BCR and whether its control can reduce retinal complications cannot be answered with our retrospective data. In our patients, 7 of 35 (20%) reported skin malignancies (6 with basal cell carcinoma and 1 with skin melanoma). One additional BCR patient had uveal melanoma. He had developed BCR in his only eye 10 years after his other eye was enucleated because of malignant melanoma of the choroid. Basal cell carcinoma is the most common malignancy in Caucasians, with a lifetime risk of 30%.29 The prevalence of basal cell carcinoma in the general population is approximately 38/100 000 to 300/100 000 person-years, but the data on prevalence of basal cell carcinoma in our age population are missing, so that the prevalence of skin malignancy in the general population cannot be compared with our BCR sample.29 Malignant melanoma of the skin reaches 4/100 000 per year to 12/100 000 per year.29,30 The combination of the 2 rare diseases (melanoma and BCR) might be coincidental, but also might be related due to a yet unknown factor. In both diseases, autoimmune reactions against human ocular tissues were reported.31–37 The clinical association between melanoma and uveitis was noticed in melanomatous swine and occasional patients.31,32,38,39 The exact role of HLA-A29 in the pathogenesis of BCR has not yet been identified; the etiologic hypotheses favor the inducement of autoimmune reactions against human ocular antigens after the contact of foreign microorganisms or other substances with HLA-A29.35 Interestingly, the MAGE genes (a group of genes that encode for antigenic, tumorspecific peptides, which are recognized by a clone of cytotoxic T-lymphocytes derived from the patient bearing the tumor) are presented by HLA-A29 molecules on human melanoma.40 At present, no randomized controlled trials have been conducted to study the efficacy of early treatment in BCR. However, no strong evidence to date exists with which to answer the question of whether late immunosuppressive treatment is effective in treating visual loss from BCR. Despite the limitations of the retrospective nature of this study, we have provided an up-to-date description of the clinical manifestations, course, and prognosis of BCR. These data might be of value when advising and treating patients with this ocular disorder of poor visual prognosis. References 1. Ryan SJ, Maumenee AE. Birdshot retinochoroidopathy. Am J Ophthalmol 1980;89:31– 45. 2. Smit RL, Baarsma GS, de Vries J. Classification of 750 consecutive uveitis patients in the Rotterdam Eye Hospital. Int Ophthalmol 1993;17:71– 6. 3. Rothova A, Suttorp-van Schulten MS, Treffers WF, Kijlstra A. Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol 1996;80:332– 6. 4. Rodriguez A, Calonge M, Pedroza-Seres M, et al. Referral Rothova et al 䡠 Birdshot Chorioretinopathy 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. patterns of uveitis in a tertiary eye care center. Arch Ophthalmol 1996;114:593–9. Vitale AT. Birdshot chorioretinopathy. In: Foster CS, Vitale AT, eds. Diagnosis and Treatment of Uveitis. Philadelphia: WB Saunders Co.; 2002:731– 41. Baarsma GS, Priem HA, Kijlstra A. Association of birdshot retinochoroidopathy and HLA-A29 antigen. Curr Eye Res 1990;9:63– 8. Levinson RD, Gonzales CR. Birdshot retinochoroidopathy: immunopathogenesis, evaluation, and treatment. Ophthalmol Clin North Am 2002;15:343–50. Priem HA, Kijlstra A, Noens L, et al. HLA typing in birdshot chorioretinopathy. Am J Ophthalmol 1988;105:182–5. Nussenblatt RB, Whitcup SM, Palestine AG. Uveitis: Fundamentals and Clinical Practice. St. Louis: Mosby-Year Book Inc.; 1996:325–33. Gasch AT, Smith JA, Whitcup SM. Birdshot retinochoroidopathy. Br J Ophthalmol 1999;83:241–9. Opremcak EM. Birdshot retinochoroiditis. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology: Basic Sciences. Philadelphia: WB Saunders Co.; 1994:475– 80. Priem HA, Oosterhuis JA. Birdshot chorioretinopathy: clinical characteristics and evolution. Br J Ophthalmol 1988;72:646 – 59. Kraut JA, McCabe CP. The problem of low vision. Definitions and common problems. In: Albert DM, Jacobiec FA, eds. Principles and Practice of Ophthalmology: Basic Sciences. Philadelphia: WB Saunders Co.; 1994:3664 – 6. Priem H. Vascular manifestations in birdshot chorioretinopathy [in French]. Bull Soc Belge Ophtalmol 1989;230:41– 8. Soubrane G, Coscas G, Binaghi M, et al. Birdshot retinochoroidopathy and subretinal new vessels. Br J Ophthalmol 1983; 67:461–7. Brucker AJ, Deglin EA, Bene C, Hoffman ME. Subretinal choroidal neovascularization in birdshot retinochoroidopathy. Am J Ophthalmol 1985;99:40 – 4. Barondes MJ, Fastenberg DM, Schwartz PL, Rosen DA. Peripheral retinal neovascularization in birdshot retinochoroidopathy. Ann Ophthalmol 1989;21:306 – 8. Rothova A, Van Schooneveld MJ. The end stage of birdshot retinochoroidopathy [letter]. Br J Ophthalmol 1995;79: 1058 –9. Fuerst DJ, Tessler HH, Fishman GA, et al. Birdshot retinochoroidopathy. Arch Ophthalmol 1984;102:214 –9. Oh KT, Christmas NJ, Folk JC. Birdshot retinochoroiditis: long term follow-up of a chronically progressive disease. Am J Ophthalmol 2002;133:622–9. LeHoang P, Cassoux N, George F, et al. Intravenous immunoglobulin (IVIg) for the treatment of birdshot retinochoroidopathy. Ocul Immunol Inflamm 2000;8:49 –57. Vitale AT, Rodriguez A, Foster CS. Low-dose cyclosporine therapy in the treatment of birdshot retinochoroidopathy. Ophthalmology 1994;101:822–31. Hirose T, Katsumi O, Pruett RC, et al. Retinal function in birdshot retinochoroidopathy. Acta Ophthalmol (Copenh) 1991;69:327–37. 24. Priem HA, De Rouck A, De Laey JJ, Bird AC. Electrophysiologic studies in birdshot chorioretinopathy. Am J Ophthalmol 1988;106:430 – 6. 25. de Courten C, Herbort CP. Potential role of computerized visual field testing for the appraisal and follow-up of birdshot chorioretinopathy. Arch Ophthalmol 1998;116:1389 –91. 26. Wolf-Maier K, Cooper RS, Banegas JR, et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA 2003;289:2363–9. 27. van Rossum CT, van de Mheen H, Witteman JC, et al. Prevalence, treatment, and control of hypertension by sociodemographic factors among the Dutch elderly. Hypertension 2000;35:814 –21. 28. Klungel OH, de Boer A, Paes AH, et al. Cardiovascular diseases and risk factors in a population-based study in The Netherlands: agreement between questionnaire information and medical records. Neth J Med 1999;55:177– 83. 29. Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol 2002;146(suppl 61):1– 6. 30. Coebergh JW, Neumann HA, Vrints LW, et al. Trends in the incidence of non-melanoma skin cancer in the SE Netherlands 1975-1988: a registry-based study. Br J Dermatol 1991;125: 353–9. 31. Albert DM, Sober AJ, Fitzpatrick TB. Iritis in patients with cutaneous melanoma and vitiligo. Arch Ophthalmol 1978;96: 2081– 4. 32. Sober AJ, Haynes HA. Uveitis, poliosis, hypomelanosis, and alopecia in a patient with malignant melanoma. Arch Dermatol 1978;114:439 – 41. 33. Cui J, Bystryn JC. Melanoma and vitiligo are associated with antibody responses to similar antigens on pigment cells. Arch Dermatol 1995;131:314 – 8. 34. Heaton JM, Mills RP. Sensorineural hearing loss associated with birdshot retinochoroidopathy. Arch Otolaryngol Head Neck Surg 1993;119:680 –1. 35. Nussenblatt RB, Mittal KK, Ryan S, et al. Birdshot retinochoroidopathy associated with HLA-A29 antigen and immune responsiveness to retinal S-antigen. Am J Ophthalmol 1982; 94:147–58. 36. de Smet MD, Yamamoto JH, Mochizuki M, et al. Cellular immune responses of patients with uveitis to retinal antigens and their fragments. Am J Ophthalmol 1990;110:135– 42. 37. Jobin D, Thillaye B, de Kozak Y, et al. Severe retinochoroidopathy: variations of humoral and cellular immunity to Santigen in a longitudinal study. Curr Eye Res 1990;9(suppl): 91– 6. 38. Feeney-Burns L, Alspaugh M, Burns RP, Gao CL. Uveitis in melanomatous swine: lack of evidence for humoral immune melanocyte destruction. Invest Ophthalmol Vis Sci 1985;26: 551– 60. 39. Chang MA, Fournier G, Koh HK, et al. Ocular abnormalities associated with cutaneous melanoma and vitiligo-like leukoderma. Graefes Arch Clin Exp Ophthalmol 1986;224:529 –35. 40. Luescher IF, Romero P, Kuznetsov D, et al. HLA photoaffinity labeling reveals overlapping binding of homologous melanoma-associated gene peptides by HLA-A1, HLA-A29, and HLA-B44. J Biol Chem 1996;271:12463–71. 959