Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
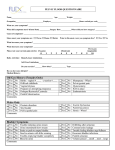
Urotherapy for childhood dysfunctional voiding and OAB Tuesday 14th February, 2012, 9.20-10.00am Urotherapy • Urotherapy means non-surgical, non-pharmacological treatment for LUT dysfunction. • Non-standardised term • Described as ‘rehabilitation of LUT’ • Involves • Education • Intervention • Life-style advice • Documentation • Support and encouragement ICCS slide library v1 2011 Aims of Urotherapy • Normalise bladder emptying • • • • • -> decreased bladder overactivity Normalise bladder filling Facilitate age-appropriate storage Facilitate optimal bowel function Normalise defaecation dynamics ICCS slide library v1 2011 Treatment: Goals • No more symptoms • urgency, wetness • No more signs • ↑PVR, high pdet, +ve EMG during voiding • Normalised flow curve • PFM relaxation during void • Normalised bladder capacity • No further episodes of UTI • Reduction in grade of VUR • Normal bowel function ICCS slide library v1 2011 Urotherapy: Patients • Significant morbidity without treatment in 40% children: • high detrusor pressure • destabilised micturition reflex • UTI • VUR • upper tract damage • constipation • hypocontractile detrusor • renal failure ICCS slide library v1 2011 Urotherapy: Patients • Collateral damage: • self-esteem • self-worth • isolation • confidence • socialization • QoL ICCS slide library v1 2011 Behavioural co-morbidities ......... “comorbid disorders interfere with treatment for enuresis/incontinence. Affected children show lower compliance and treatment results are lower. Therefore, children with incontinence should be screened for psychological disorders even in pediatric and urological settings. Children with a severe condition should be referred to the mental health service (child psychiatrists and child psychologists).An interdisciplinary approach is needed for optimal care in daytime wetting children.” • Kuhn et al. Journal of Urology, 182(4 Suppl), 1967-1972. ICCS slide library v1 2011 • Screening all children • A • L • T • E • R • N • A • T • I • V • E • History, observa6on, explora6on • Short screening ques6onnaires • Problem items/behaviours present? • NO • YES • Standard long ques6onnaires • Problem items/behaviours present? • Treatment of • enuresis/incon6nence only • NO • YES • Full child psychiatric/ psych assessment • Child psychiatric disorder present? • YES • Treatment of disorder • In addi6on to NE/incon6nence ICCS slide library v1 2011 • NO • Counselling in addi6on to • treatment of • enuresis/incon6nence Questionnaires • Short – Short screening instrument for psychological problems in enuresis. SSIPPE (Van Hoecke 2007) Validated. 13 items. Yes/no – Parental Questionnaire Enuresis/Urinary Incontinence (von Gontard 2003) Non-validated. 15 items. Yes/no • Standard long CBCL (Achenbach 1991) 113 items • QoL –generic, disease specific eg PinQ (Bower et al. 2006) • Other ICCS slide library v1 2011 Working with children • Education, education, education • Understand the pace of assessment and treatment is slower • Let the family know at the outset ‘this takes time’ • The child is your collaborator - in assessment and treatment • Treatment is not ‘done’ to the child – he/she participates • The child is the focus- not the problem • Understand different behaviours eg a withdrawn child, de-motivated child, • Offer structured choices, achievable goals. Set the child up for success not failure • Remove blame and guilt for every-one ICCS slide library v1 2011 Treatment Components Assessment Re-assessment Intervention ICCS slide library v1 2011 Education Motivation Removal of shame and blame • Put Documentation in place • BECAUSE • Chronicity • Motivation • Relapse • Ongoing assessment • Measure outcomes • PROGRESS NOTES • Child’s name___________________________ • Date of consultation_____________________ • Diagnosis______________________________ • Results • Test results______________________________________________________________ • ________________________________________________________________________ • Bladder diary • Voiding frequency □ <4/day □ 4-8/day □ > 8/day • Fluid intake _____________________________________________________________ • MVV_______ Ave.VV________1st am void____________O/N urine vol_____________ • Wetting • ______nights/week _______times/night □ damp □ wet □ flooded • ______days/week -------_______times/day □ damp □ wet □ flooded • Medications taken ________________________________________________________ • ________________________________________________________________________ • • Alarm diary • _____ dry nights/week Alarm __________times/night. ____________nights/week. • Time/s of alarm_________________ Waking to alarm YES NO With help YES NO • Size of wet patch □ small □ medium □ large • Problems________________________________________________________________ • Bowel diary • Bowel actions ________/day ________/week BSS ____________________________ • □ Self-initiated □ Sits • Soiling YES / NO □ Stain □ Scrape _________/day _________/week • Parent’s compliance □ good □ fair □ poor □ N/A • Child’s compliance □ good □ fair □ poor □ N/A • Progress overall __________________________________________________________ • ________________________________________________________________________ • Today’s Flow/scan pattern_______________ MFR_________ml/sec PVR_______ mls Urinalysis_________________________ • Further management/problems_________________________________________________ __________________________________________________________________________ • Further referrals_____________________________________________________________ • Name ICCS slide library v1 2011 Signature Treatment: Education • ? child’s understanding of bladder structure and function • Don’t assume child / parents understand LUT • Age-appropriate explanation of • anatomy • aetiology of specific dysfunction ICCS slide library v1 2011 Treatment: Education • What is not associated with disorder • laziness, naughtiness, dirtiness, low IQ • Attribute dysfunction to external factors • Establish prevalence in realistic context • Explore motivation • Establish child as co-investigator and collaborator ICCS slide library v1 2011 First-active bowel management • For 6 months minimum • Hygiene, correct wiping, containment ICCS slide library v1 2011 Treatment: “Standard Therapy” • Routine hydration • Regular, optimal voiding • Pelvic floor muscle awareness • +/- pharmacotherapy • +/- biofeedback training • +/- neuromodulation • +/- alternative / holistic intervention ICCS slide library v1 2011 “Standard Therapy” • Routine hydration • Often voluntary dehydration • Re-set high set-point for thirst • Drinks of 200mls +/- age -dependent • 5-6 / day • Dilutes concentrated (? irritating) urine • Avoid sugar and caffeine ICCS slide library v1 2011 “Standard Therapy” • Regular voiding: • Every 2-3 hours • May need vibrating alarm watch • Prevent over-distension (including overnight) • Re-establish sensory awareness • Minimised OAB activity -> leakage • Must be unopposed emptying ICCS slide library v1 2011 FROM THIS ICCS slide library v1 2011 TO THIS PFM Relaxation Let’s first identify • • • • Correct PFM action “lift” Co-contraction of lower Trans versus Abs, NOT Rectus Abs Lower chest breathing • From . Raizada ICCS slide library• v1 2011 V & Mittal RK. Pelvic floor anatomy and applied physiology. Gastroenterol Clin N Am. 2008,37: 493-509 Treatment: PF relaxation • Learn to contract and relax the PF muscles • Without valsalva / accessory muscles • Practice of correct recruitment +/- any form of biofeedback Therapist Palpation/observation Lower transversus abdominis Perineal body/lift Med’l border ischium Muscle balance between PFM and upper abdominals-observe breathing/abd’l action • Child palpation/observation • Self-palpation of PF or transverse abdominus • Watching abdomen in mirror and identifying rectus activity ICCS slide library v1 2011 PFM Relaxation • Pelvic floor muscle: awareness and relaxation • Sufficient awareness to practise correctly • Apply during initiation of void • Apply throughout void • Apply during defaecation ICCS slide library v1 2011 PFM Relaxation • Optimal voiding mechanics • Supported seating / squatting • Neutral lumbar spine • ? Foot position • Feet on stool; knees apart • Prevent urine entrapment • No pushing • Focused abdominal relaxation • Aim for a “waterfall” void • ? Double void • Poor lumbo-thoracic posture ICCS slide library v1 2011 PFM Relaxation • +/- biofeedback during voiding • Real time uroflow • Auditory feedback • EMG • Abdominal ultrasound • Post void ultrasound for residual volume ICCS slide library v1 2011 Use of TAUS PFM relaxation • PFM contraction • 5year-old girl • Bladder neck ‘lift” • SAGGITAL VIEW • Rectus abdominis • Transversus abdominis • Bladder neck ICCS slide library v1 2011 Use of TAUS Measure rectal diameter • Measurement of rectal diameter illustrated by Singh et al (2005) ICCS slide library v1 2011 FROM THIS ICCS slide library v1 2011 TO THIS Treatment OAB Pharmacotherapy • When to supplement standard therapy with anticholinergics: • Idiopathic OAB with no evidence of dysfunctional emptying • OAB with concurrent VUR or RUTI • Very small FBC • Properties: anti-muscarinic, local anaesthetic, SM relaxant • S/E: personality changes, headache, blurred vision, constipation, dry mouth, flushing Monitor bladder emptying and constipation ICCS slide library v1 2011 Treatment Pharmacotherapy • Other medications • alpha-blockers: for dysfunctional bladder neck; may be used when PFM retraining doesn’t improve PVR • Botulinum toxin A • Antibiotics Treatment of UTI (of course) Long-term prophylaxis in some children with recurrent UTIs due to residual urine ICCS slide library v1 2011 Recent review articles: • Barroso, U., Jr., Tourinho, R., Lordelo, P., Hoebeke, P., & Chase, J. (2011). Electrical stimulation for lower urinary tract dysfunction in children: A systematic review of the literature. Neurourology and Urodynamics. • De Gennaro, M., Capitanucci, M., Mosiello, G., & Zaccara, A. (2011). Current State of Nerve Stimulation Technique for Lower Urinary Tract Dysfunction in Children Journal of Urology, 185, 1571-1577. • Barroso, U., Jr., Hoebeke, P., Van Laeke, E., De Gennaro, M., Fox, J., & Chase, J. (2011). Electrical Stimulation for Lower Urinary Tract Dysfunction. Dialogues in Pediatric Urology, 32(4). 30 ICCS slide library v1 2011 Urotherapy Neuromodulation • Neuromodulation for OAB • Increases release of neurotransmitters à • ↓cholinergic activity • ↑ beta adrenergic activity (-> relax bladder vault) • VIP, serotonin • Inhibition of OAB: 5-10Hz • TENS –pudendal afferents, S2,3 foraminae, S3 dermatome • SANS/PTNS (20Hz) • Electro-acupuncture ICCS slide library v1 2011 Urotherapy Neuromodulation Contraction of detrusor: Intravesical stimulation Bladder pain Suprapubic or spinal Pelvic floor/sphincter strenthening Anorectal malformation Pelvic floor relaxation Not routinely used for sensory awareness ? Perineal / anal electrode Adjunctive- not stand-alone therapy Training in electrotherapeutics prerequisite for clinical use ICCS slide library v1 2011 Urotherapy Neuromodulation Efficacy • No known predictors of efficacy • Most studies pre/post intervention series • Sans- 50-80% improvement in clinical refractory OAB symptoms (De Gennaro M et al. 2004.,Hoebeke P et al 2002) • For OAB Tens -clinical changes: • • • • Significant decrease number wet episodes Significant decrease urge intensity Significant improvement in FVC parameters Significant improvement in U/D parameters • Electrical Stimulation for Lower Urinary Tract Dysfunction in Children. A Systematic Review of the Literature. Ubirajara Barroso J, Rafael Tourinho, Patrícia Lordêlo, Janet Chase, Piet Hoebeke Neurourol Urodyn 2011 (in press) ICCS slide library v1 2011 Urotherapy Neuromodulation Efficacy • • • • Hagstrom et al. report on RCT Tens refractory daytime urinary urge incontinence N=27 The active group had a significantly greater decrease in daily incontinence episodes compared to the sham treated group (p <0.01) • No change in MVV or AVV ? Changes related to sensory mechanisms • First line treatment (Lordelo et al) Hagstroem et al., 2009. J Urol, 182(4 Suppl): p. 2072-8. Lordelo et al. 2009 J Urology, 182(6), 2900-2904. ICCS slide library v1 2011 Urotherapy Neuromodulation Efficacy IVS - neurogenic and idiopathic detrusor underactivity -voiding was normalised in 85% effect long lasting in 72%; idiopathic > neurogenic (Gladh G et al 2003) Efficacy requires: patient co-operation preserved reflex arc compliant bladder active detrusor fibres total or partial integrity of PFM innervation (Fall & Lindstrom 1991) • Gladh, G., Mattsson, S., & Lindstrom, S. (2003). Neurourology and Urodynamics, 22(3), 233-242 • Fall, M., & Lindstrom, S. (1991).Urologic Clinics of North America, 18(2), 393-407. ICCS slide library v1 2011 Urotherapy Neuromodulation neurogenic bladder • Different outcome measures – difficult to collate studies • Some improved bladder storage • Some improved emptying • Minimal improvement in continence • 1 RCT using IFT - with significant improvement in all UDS parameters except for maximum bladder capacity and significant improvement in continence in treatment group ( Kajbafzadeh et al 2009) • Kajbafzadeh et al. (2009).Urology, 74(2), 324-329. ICCS slide library v1 2011 Urotherapy Neuromodulation Bowel Sacral Tens –clinically bowel sensation improves but not studied • RCT -Transcutaneous electrical stimulation using IFC increased bowel motility, decreased bowel transit time, pain and soiling and improved physical QoL in children with STC. • Daily home-based IFT further improved defaecation frequency • Pilot study IFT lumbo-sacral placement of electrodes–sig >se def’n no, improvement in abd’l pain • SN implantation – children with bladder and bowel dysfunction, constipation • improved in 12 of 15 patients (80%) • 7 (41%) had resolution • Clarke et al. 2009J Pediatr Surg, 44: 408 • Ismail et al. 2009 J Pediatr Surg, 44: 2388 • Humphreys et al. 2006 J Urology, 176(5), 2227-2231 • Roth et al. 2008 J Urology, 180(1), 306-311 (discussion 311). ICCS slide library v1 2011 Neuromodulation: Summary • • • • Positive role for neuromodulation in children with LUTD Adjunctive to other intervention No known predictors of efficacy Understanding of electrotherapeutics is a prerequisite for clinical use • Neuromodulation of the bowel shows promise ICCS slide library v1 2011 Urotherapy Clean intermittent catherisation • The friend of the upper tracts • Assist in bladder emptying • Assist in reducing high detrusor pressures • Can be introduced through stoma • Very young children can learn to use • Essential with neurogenic bladder, earlier commencement -> better protection • Bladder underactivity, ↑PVR, recurrent UTI, wetting • Prevent overdistension day and night ICCS slide library v1 2011 Urotherapy Urethro-vaginal reflux • Post-void dampness • 24 hours of reverse toileting ie facing wall/cistern -may be diagnostic • Teach the child to void with anterior pelvic tilt • Knees well apart • So urinary stream directed down, not back • Increasing IAP ie. cough at end of voiding will help vagina empty • Mattsson, S. and G. Gladh Pediatrics, 2003. 111(1): p. 136-9. ICCS slide library v1 2011 Urotherapy Troubleshooting • Specifics of problems • Strategies to change situation in future • Action by child • Action by teacher / parent / other • Who needs to facilitate change • Contact with teacher • Containment advice in key situations ICCS slide library v1 2011 Urotherapy : Review • “.. frequent follow-up with emotional support and encouragement .. important components of intervention” (Longstaffe et al 2000) • Irrespective of treatment success • How frequent: depends on • Type of intervention • Feedback / measures needed • Child’s motivation ICCS slide library v1 2011 Urotherapy Outcome Measures • Realistic and achievable • improved hydration: e.g. finish drink bottle • regular voiding • completion of FVC / bowel diary • use of watch alarm • Unambiguous: • Quantified • Precise: e.g. wet patch or dried wet patch • Validated and reliable • LOOK AT ICCS WEBSITE ICCS slide library v1 2011 Urotherapy Efficacy • Evaluate by resolution of symptoms • Incontinence episodes / pads used • Urge episodes • UTI • Faecal soiling • Psychological effects and QoL • Resolution of signs • Bladder emptying efficiency (incl. PVR) • Bladder wall changes • Dyssynergic voiding pattern • Grade of VUR ICCS slide library v1 2011 Urotherapy approaches are significantly better than historical results utilising anticholinergic medication alone Urotherapy effective in decreasing urinary tract infections, improving constipation, and decreasing the need for intervention in patients with vesicoureteral reflux • Bauer et al.1980. Urologic Clinics of North America, 7(2), 321–361. • De Paepe et al. 1998) British Journal of Urology, 81(Suppl 3), 109–113. • Herndon, C. D., Decambre, M., & McKenna, P. H. 2001Journal of Urology, 166(5), 1893–1898. • McKenna, L. S., & McKenna, P. H. 2004 Journal of Wound, Ostomy and Continence Nursing, 31(6), 351–356. • McKenna, P. H., & Herndon, C. D. 2000 Curr Opin Urol 10(6): 599-606. Current Opinion in Urology, 10(6), 599–606. • van Gool, J. D., & Vijverberg, M. A.1992 Scandinavian Journal of Urology and Nephrology, 141(Suppl), 93–103. ICCS slide library v1 2011 For how long? • Till symptoms or signs have resolved • Till the child is happy • Till the family is happy • Till the bladder is “normal” as you can make it • Till the upper tracts are at least risk • Bowel function is normal or actively managed • AND if there is likely to be change/deterioration you will know about it because of recall appointments ICCS slide library v1 2011 • C AIRNS CONVENTION CENTRE -‐ AUSTRALIA • The Joint Mee7ng of the • Interna7onal Children’s Con7nence Society and the Con7nence Founda7on of Australia • Sep or Oct 2014 • Serious Business in Australia’s Most Stunning Location