Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
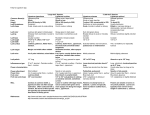
Arthritis & Rheumatism (Arthritis Care & Research) Vol. 57, No. 7, October 15, 2007, pp 1143–1150 DOI 10.1002/art.22994 © 2007, American College of Rheumatology ORIGINAL ARTICLE Safety and Efficacy of Ganoderma lucidum (Lingzhi) and San Miao San Supplementation in Patients With Rheumatoid Arthritis: A DoubleBlind, Randomized, Placebo-Controlled Pilot Trial EDMUND K. LI,1 LAI-SHAN TAM,1 CHUN KWOK WONG,1 WAI CHING LI,1 CHRISTOPHER W. K. LAM,1 SISSI WACHTEL-GALOR,2 IRIS F. F. BENZIE,3 YI XI BAO,3 PING CHUNG LEUNG,4 AND BRIAN TOMLINSON1 Objective. To examine the efficacy of popular Chinese herbs used in a traditional Chinese medicine (TCM) combination of Ganoderma lucidum and San Miao San (SMS), with purported diverse health benefits including antioxidant properties in rheumatoid arthritis (RA). Methods. We randomly assigned 32 patients with active RA, despite disease-modifying antirheumatic drugs, to TCM and 33 to placebo in addition to their current medications for 24 weeks. The TCM group received G lucidum (4 gm) and SMS (2.4 gm) daily. The primary outcome was the number of patients achieving American College of Rheumatology (ACR) 20% response and secondary outcomes included changes in the ACR components, plasma levels, and ex vivo–induced cytokines and chemokines and oxidative stress markers. Results. Eighty-nine percent completed the 24-week study. Fifteen percent in the TCM group compared with 9.1% in the placebo group achieved ACR20 (P > 0.05). Pain score and patient’s global score improved significantly only in the TCM group. The percentage, absolute counts, and CD4ⴙ/CD8ⴙ/natural killer/B lymphocytes ratio were unchanged between groups. CD3, CD4, and CD8 lymphocyte counts and markers of inflammation including plasma interleukin-18 (IL-18), interferon-␥ (IFN␥)–inducible protein 10, monocyte chemoattractant protein 1, monokine induced by IFN␥, and RANTES were unchanged. However, in an ex vivo experiment, the percentage change of IL-18 was significantly lower in the TCM group. Thirteen patients reported 22 episodes (14 in placebo group and 8 in TCM group) of mild adverse effects. Conclusion. G lucidum and San Miao San may have analgesic effects for patients with active RA, and were generally safe and well tolerated. However, no significant antioxidant, antiinflammatory, or immunomodulating effects could be demonstrated. KEY WORDS. Rheumatoid arthritis; Ganoderma lucidum; Cytokines. INTRODUCTION Ganoderma lucidum or lingzhi, which in Chinese means “herb of spiritual potency,” is one form of the mushroom ClinicalTrials.gov identifier: NCT00432484. 1 Edmund K. Li, FRCP(C), Lai-Shan Tam, MD, Chun Kwok Wong, PhD, Wai Ching Li, RN, Christopher W. K. Lam, PhD, Brian Tomlinson, FRCP: Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong; 2Sissi WachtelGalor, PhD: The Hong Kong Polytechnic University, Hong Kong; 3Iris F. F. Benzie, DPhil, Yi Xi Bao, PhD: Chongqing University of Medicine Science, Chongqing, China; 4Ping Chung Leung, DSc: The Institute of Chinese Medicine, Chinese University of Hong Kong, Hong Kong. Address correspondence to Edmund K. Li, FRCP(C), Department of Medicine & Therapeutics, Prince of Wales Hospital, New Territories, Shatin, Hong Kong. E-mail: edmundli@cuhk. edu.hk. Submitted for publication December 15, 2006; accepted in revised form April 18, 2007. Ganoderma lucida, which has been used to treat all forms of ailments, and is the oldest mushroom known to have been used in ancient Chinese medicine. Lingzhi allegedly has multiple health benefits for a broad range of conditions from arthritis to cancers, and has therefore attained an unparalleled reputation in the East as the ultimate herbal substance. From the spores of G lucidum, 6 highly oxygenated lanostane-type triterpenes have been isolated called ganoderic acid, which is the active ingredient. G lucidum is widely cultivated nowadays and is sold as raw material or lingzhi extracts in many Asian markets and Western health shops. In recent years, there has been an increasing number of reports of the biologic effects of G lucidum in the scientific literature. Many suggest that G lucidum has antioxidant properties as a free radical scavenger (1,2), indicating that some of the antioxidant components are well absorbed, resulting in a significant increase in the total antioxidant 1143 1144 power in the plasma as assessed by the ferric-reducing/ antioxidant power (FRAP) test (3). Other studies suggest that G lucidum can improve immunologic functions (4,5), with potential bidirectional effects exhibiting both immunoreactive and immunomodulatory activity. G lucidum was shown to inhibit histamine release from mast cells (6), to reduce production of antibodies and suppress cytokine production, and to up-regulate adhesion molecules (7,8), but it was also found to activate mitogen-activated protein kinase and reduce cytotoxicity, oxidative damage, and apoptosis in some in vitro studies (7,9). Its growing popularity in patients with cancer may be supported by its suppressive effects of tumor growth in vitro (10 –13). Despite the large amount of scientific literature on G lucidum, we could find no published studies in the English language literature of its effects on inflammatory arthritic diseases. Clinical studies in general are limited, despite the widespread use of this product. Recently, there has been increased interest in the role of an enzyme, secretory phospholipase A2 (sPLA2), as a mediator in the inflammatory pathway in various types of arthritis including rheumatoid arthritis (RA) (14). This enzyme can serve as a critical modulator of cytokine-driven inflammation. In ex vivo synovial cell cultures, sPLA2 enhances tumor necrosis factor ␣ (TNF␣) induction of prostaglandin production, in part via increased expression of cyclooxygenase 2 and cytosolic phospholipase A2. Mononuclear cells from peripheral blood and synovial fluid of patients with RA respond to sPLA2 with enhanced release of TNF␣ and interleukin-6 (IL-6) (15). Selective inhibition of sPLA2 has yielded variable results in an adjuvant-induced arthritis model in rats (16). Its combined antioxidant, putative antiinflammatory properties and our preliminary unpublished data using an in vitro test system showing inhibition of the enzyme phospholipase A2 from bee venom and from hog pancreas suggest that G lucidum may have a role in the treatment of patients with RA. In addition to G lucidum, San Miao San (SMS; translated as Powder of Three Wonderful Drugs) is another herbal remedy that is of relevance and interest in RA. In traditional Chinese medicine (TCM), RA belongs to the category Bi Zheng, which is defined as a syndrome marked by arthralgia and dyskinesia of the joints and limbs due to attack of the meridians of the limbs by wind, dampness, and heat or cold pathogens. SMS is a traditional Chinese medicinal formula that has been used empirically to treat Bi Zheng for hundreds of years. It is composed of the herbs Rhizoma atractylodis (Cangzhu), Cotex phellodendri (Huangbai), and Radix achyranthes Bidentatae (Niuxi). In recent years, pharmacologic studies have confirmed antiinflammatory and pain-relieving properties of SMS in animal models, along with some preliminary clinical observations from the Chinese literature that reported that SMS had a therapeutic effect in the treatment of children with RA. Furthermore, use of the combination of SMS and G lucidum for the analgesic and antiinflammatory effects was a common practice according to the experts in TCM. They believed that this combination may have additive effects. The goal of this pilot study was to investigate the potential efficacy of a combined standard formulation of G Li et al lucidum and SMS as a therapeutic adjunct for patients with active RA. PATIENTS AND METHODS Patients. A total of 65 patients who fulfilled the American College of Rheumatology (ACR; formerly the American Rheumatism Association) 1987 revised criteria for the classification of RA (17) were recruited from the rheumatology outpatient clinic at the Prince of Wales Hospital, the teaching hospital of The Chinese University of Hong Kong. Patients taking disease-modifying antirheumatic drugs (DMARDs) including hydroxychloroquine, sulfasalazine, methotrexate, and leflunomide were eligible for inclusion if they were receiving a stable dose for at least 3 months before screening and remained on this regimen throughout the study. Patients receiving stable doses of one nonsteroidal antiinflammatory drug or prednisone in dosages up to 10 mg daily were also included. The dosage of methotrexate ranged between 12.5 and 17.5 mg/week with folic acid supplementation. All patients were instructed not to make any changes in their background therapies during the study. Intraarticular or pulse corticosteroids were not permitted during the study because they may inhibit phospholipase activities. Exclusion criteria were as follows: ⬍18 years of age, pregnancy, use of intraarticular corticosteroids within 4 weeks preceding the study, any severe chronic or uncontrolled comorbid disease, or wheelchair bound with restricted mobility. Ethical approval was obtained from the Ethics Committee at The Chinese University of Hong Kong. All patients gave written informed consent at the time of enrollment. In this 24-week randomized, double-blind, placebo-controlled trial, patients who met the inclusion and exclusion criteria were randomly assigned to receive either G lucidum with SMS or placebo using a computer-generated list of random numbers in blocks of 5. The list was generated at the Institute of Chinese Medicine, The Chinese University of Hong Kong. Study medications were dispensed as sealed packages in consecutive numbers. A research nurse was responsible for dispensing study medications. The investigators, research nurse, and participants were not aware of the treatment assignments throughout the study. Treatment codes were only broken after completion of the study. Preparation of the extract. G lucidum and SMS were supplied as capsules, containing 4.0 gm of G lucidum extract, 2.4 gm of Rhizoma atractylodis (Cangzhu), 2.4 gm of Cotex phellodendri (Huangbai), and 2.4 gm of Radix achyranthes Bidentatae (Niuxi). Each patient took either 3 capsules twice daily as recommended by the TCM experts or identical-looking placebo. The compound used in this study was prepared in the Institute of Chinese Medicine at The Chinese University of Hong Kong. The herbal formula was constructed by combining G lucidum 35.7% and SMS, which comprises 3 Chinese herbs, namely, Rhizoma atractylodis 21.4%, Cortex phellodendri Chinensis 21.4%, and Radix achyranthes Bidentatae 21.4%. The herbal preparation was manufactured, San Miao San and Ganoderma lucidum in RA 1145 Table 1. Clinical and demographic data at baseline* Female sex Age, mean ⫾ SD years Duration of RA, median (IQR) years Rheumatoid factor positive Erosive disease Tender joints, median (IQR) Swollen joints, median (IQR) Physician’s global (VAS 0–10), mean ⫾ SD Patient’s global (VAS 0–10), mean ⫾ SD Pain (VAS 0–10), mean ⫾ SD ESR, median (IQR) mm/hour C-reactive protein, median (IQR) mg/liter HAQ, mean ⫾ SD Prednisolone Leflunomide Hydroxychloroquine Sulfasalazine Methotrexate Total no. of DMARDs 1:⬎1 Ganoderma lucidum ⴙ SMS (n ⴝ 32) Placebo (n ⴝ 33) 27 (84) 50 ⫾ 10 9.3 (4.8, 18.0) 24 (75) 25 (78) 2 (1, 5) 3 (2, 5) 4.5 ⫾ 1.5 6.0 ⫾ 2.6 5.2 ⫾ 2.4 41 (24, 71) 9.8 (3.0, 24.5) 1.2 ⫾ 0.8 3 (9) 10 (31) 7 (22) 8 (25) 22 (69) 19 (59):13 (41) 29 (88) 50 ⫾ 13 7.8 (5.5, 11.5) 23 (70) 25 (76) 3 (2, 4) 3 (2, 6) 4.5 ⫾ 1.6 5.7 ⫾ 2.4 5.0 ⫾ 2.5 45 (20, 75) 9.7 (3.0, 39.3) 1.2 ⫾ 0.8 3 (9) 13 (39) 5 (15) 4 (12) 22 (67) 21 (64):12 (36) * Values are the number (percentage) unless otherwise indicated. SMS ⫽ San Miao San; RA ⫽ rheumatoid arthritis; IQR ⫽ interquartile range; VAS ⫽ visual analog scale; ESR ⫽ erythrocyte sedimentation rate; HAQ ⫽ Health Assessment Questionnaire; DMARDs ⫽ disease-modifying antirheumatic drugs. packaged, and labeled by a factory in Hong Kong based on good manufacturing practice standard. The crude herbs were supplied in one batch from reputable suppliers and were kept and stored in a cool and dry place. Before the water extraction procedure, the crude herbs of G lucidum, Rhizoma atractylodes, Cortex phellodendri Chinensis, and Radix achyranthes Bidentatae were cleaned, washed, and cut into fragments no bigger than 6 cm in length. Rhizoma atractylodis was ground into powder below 100 mesh for later use. During the water extraction process, distilled water was added to macerate the herbs for 1 hour, and then the mixture was boiled at 100°C for 1 hour for the first extraction. There were 3 extractions in total. The second extraction involved adding distilled water and boiling at 100°C for 1 hour and the third extraction involved boiling for half an hour. After extraction, the liquid extract was concentrated at ⫺660 mm Hg and at 60°C and was spray dried to produce a powder extract. The dry extract powder was sieved and mixed with Rhizoma atractylodis powder. It was then encapsulated at 500 mg per capsule and polished and packaged in a clean room at 10 –20°C and 50% humidity. Placebo capsules, which were identical in appearance, contained starch and a coloring agent. Assessment of clinical response. All patients were evaluated at baseline and weeks 4, 8, 16, and 24. The following clinical and laboratory variables were assessed at each visit: number of tender joints and swollen joints, patient’s global assessment (using a 0 –10-cm visual analog scale [VAS]), physician’s global assessment (using a 0 –10-cm VAS), duration of morning stiffness, plasma C-reactive protein (CRP) level, concentration, and erythrocyte sedimentation rate (ESR). Primary outcome. The primary outcome was the number of patients who achieved the ACR 20% response, which is defined as having a 20% improvement in the 5 components including the number of tender and swollen joints and a 20% improvement in 3 of the 5 remaining core set measures: patient and physician global assessments; pain; disability as assessed by the Health Assessment Questionnaire (HAQ), which is an objective self-administered questionnaire that measures the functional disability of patients with RA (18); and an acute-phase reactant, ESR or CRP level (19). Secondary outcomes. Secondary outcomes included changes in the ACR components including tender and swollen joint count, physician’s and patient’s global assessment, HAQ score, and ESR or CRP level. The other laboratory investigations included measurements of the total antioxidant power of plasma by the FRAP assay and plasma ascorbic acid concentration. Both were simultaneously measured by the FRASC (20), a modified version of the FRAP assay (US patented) (21). The MultiTEST IMK Kit with TruCOUNT tubes (Becton Dickinson, San Jose, CA) and the lyse/no-wash method were used for the assessment of the ratio and absolute counts of CD4⫹ (T helper lymphocytes), CD8⫹ (T suppressor lymphocytes and cytotoxic T lymphocytes), natural killer (NK) cells, and B lymphocytes in EDTA whole blood samples using a 4-color FASCalibur flow cytometer (Becton Dickinson). The concentration in EDTA level and the ex vivo levels of induced cytokines and chemokines were measured after treatment with lipopolysaccharide (25 g/ ml) or phytohemagglutinin (5 g/ml) for 24 hours for interferon-␥ (IFN␥)–inducible protein 10 (IP-10), monocyte chemoattractant protein 1, monokine induced by IFN␥, 1146 Li et al Table 2. Changes in the American College of Rheumatology (ACR) core set variables and antioxidant levels after 6 months of either Ganoderma lucidum plus SMS or placebo* Ganoderma lucidum (n ⴝ 28) Variables ACR core set Tender joints, median (IQR) Swollen joints, median (IQR) Physician’s global (VAS 0–10) Patient’s global (VAS 0–10) Pain (VAS 0–10) ESR, median (IQR) mm/hour C-reactive protein, median (IQR) mg/liter HAQ Antioxidant levels FRAP value, moles/liter Serum ascorbic acid levels, moles/liter Placebo (n ⴝ 30) Baseline 6 months Baseline 6 months 2 (1, 5) 3 (2, 5) 4.3 ⫾ 1.5 5.7 ⫾ 2.5 4.9 ⫾ 2.3 40 (22, 50) 9.2 (3.0, 22.2) 1.2 ⫾ 0.8 2 (0, 4) 4 (2, 6) 4.8 ⫾ 2.2 4.7 ⫾ 2.6† 3.9 ⫾ 2.5† 33 (19, 56) 11.3 (3.0, 15.5) 1.3 ⫾ 0.7 2 (2, 3) 3 (2, 6) 4.5 ⫾ 1.7 5.4 ⫾ 2.3 4.8 ⫾ 2.4 44 (18, 76) 9.8 (3.0, 33.0) 1.1 ⫾ 0.8 1 (0, 6) 4 (2, 8) 4.8 ⫾ 2.5 4.8 ⫾ 2.5 4.5 ⫾ 2.3 42 (32, 75) 13.3 (5.1, 20.7) 1.2 ⫾ 0.7 942 ⫾ 213 46.5 ⫾ 16.0 960 ⫾ 188 48.1 ⫾ 20.8 956 ⫾ 137 51.1 ⫾ 23.1 969 ⫾ 212 46.1 ⫾ 18.7 * Values are the mean ⫾ SD unless otherwise indicated. FRAP ⫽ ferric-reducing/antioxidant power test; see Table 1 for additional definitions. † P ⬍ 0.05. RANTES, IL-8, IL-6, and IL-18 at baseline, and were measured by cytometric bead array using flow cytometry or enzyme-linked immunosorbent assay at 8 and 24 weeks after treatment (22). Assessment of adverse reactions. At each visit, patients were asked if there were any adverse effects. When an adverse event was claimed, the timing relative to the administration of the drugs was noted. Blood pressure, blood cell count, serum creatinine, and liver function test results were recorded before study entry and at each visit during the study. Statistical analysis. Comparisons between the group treated with G lucidum and SMS and the placebo group for demographic and clinical characteristics were performed using chi-square tests, Student’s t-test, or Mann-Whitney U tests where appropriate. Comparisons before and after treatment in each group were assessed using paired t-tests or Wilcoxon’s signed rank test as appropriate. All hypotheses were 2-tailed, and P values less than 0.05 were considered significant. Analyses were performed using SPSS for Windows, version 10.0 (SPSS, Chicago, IL). RESULTS The demographic features of the 65 patients are shown in Table 1. There were no significant differences between the 2 groups. A total of 58 patients (89.2%) completed the 24-week study, with premature termination occurring in 3 patients in the placebo group (2 due to inefficacy as defined when patients required increased doses of drugs or a change in the drugs, and 1 due to emigration) and 4 patients in the G lucidum and SMS group due to inefficacy Table 3. Percentage change and absolute counts of lymphocyte subsets after treatment with Ganoderma lucidum plus San Miao San and placebo* Ganoderma lucidum (n ⴝ 28) Immune markers % of T lymphocyte (CD3⫹) Absolute counts of T cell (CD3⫹; cells/l) % of Ts and CTL (CD8⫹) Absolute counts of Ts and CTL (CD8⫹; cells/l) % of Th (CD4⫹) Absolute counts of Th cells (CD4⫹; cells/l) Absolute counts of lymphocytes (cells/l) % of NK cells Absolute counts of NK cells % of B cells Absolute counts of B lymphocytes Ratio of Th/Ts and CTL Placebo (n ⴝ 30) % change at 8 weeks % change at 24 weeks % change at 8 weeks % change at 24 weeks ⫺0.59 ⫾ 0.86 5.83 ⫾ 4.05 ⫺2.57 ⫾ 1.64 3.27 ⫾ 4.46 ⫺1.19 ⫾ 1.34 ⫺2.59 ⫾ 3.59 ⫺2.27 ⫾ 2.14 ⫺4.03 ⫾ 3.67 0.30 ⫾ 1.50 15.39 ⫾ 4.49 ⫺0.25 ⫾ 1.73 14.90 ⫾ 5.01 1.76 ⫾ 1.39 1.45 ⫾ 4.06 ⫺1.12 ⫾ 1.93 ⫺0.73 ⫾ 4.67 0.12 ⫾ 1.73 5.96 ⫾ 4.38 6.64 ⫾ 4.18 1.01 ⫾ 4.92 12.26 ⫾ 7.76 7.64 ⫾ 6.82 13.89 ⫾ 8.26 3.86 ⫾ 3.79 ⫺0.40 ⫾ 2.13 ⫺1.34 ⫾ 4.51 ⫺1.33 ⫾ 3.69 2.86 ⫾ 6.15 3.36 ⫾ 8.75 9.51 ⫾ 6.77 6.52 ⫾ 7.97 3.86 ⫾ 3.78 0.82 ⫾ 1.99 14.59 ⫾ 4.63 13.94 ⫾ 4.14 1.39 ⫾ 4.98 17.02 ⫾ 7.65 4.21 ⫾ 4.19 18.35 ⫾ 5.07 5.21 ⫾ 3.03 ⫺3.17 ⫾ 2.30 1.81 ⫾ 3.84 ⫺0.23 ⫾ 3.74 4.91 ⫾ 7.90 5.20 ⫾ 8.02 8.89 ⫾ 5.58 8.15 ⫾ 6.49 5.21 ⫾ 3.04 * Values are the mean ⫾ SEM. % change ⫽ [(parameter at week 8 or week 24 ⫺ parameters at baseline)/(parameter at baseline)] ⫻ 100. There were no significant differences in the changes between groups. Ts ⫽ T suppressor lymphocytes; CTL ⫽ cytotoxic T lymphocyte; NK ⫽ natural killer cells. San Miao San and Ganoderma lucidum in RA 1147 Table 4. Percentage change in the plasma concentration of cytokines and chemokines after treatment with either Ganoderma lucidum plus SMS or placebo* Ganoderma lucidum ⴙ SMS (n ⴝ 28) Parameters Cytokines IL-18 Chemokines IP-10 MCP-1 MIG RANTES IL-8 Placebo (n ⴝ 30) % change at 8 weeks % change at 24 weeks % change at 8 weeks % change at 24 weeks ⫺1.88 (⫺9.18, 17.11) ⫺3.11 (⫺14.01, 16.33) ⫺2.61 (⫺15.22, 28.8) 4.74 (⫺21.11, 30.28) ⫺25.33 (⫺32.55, 7.65) 1.85 (⫺7.18, 16.89) ⫺1.95 (⫺32.05, 24.81) 207.36 (0.81, 676.96) 0.00 (⫺31.68, 108.33) ⫺2.85 (⫺16.82, 17.95) 1.44 (⫺20.61, 37.48) 14.48 (⫺11.90, 43.03) 3.44 (⫺67.21, 273.33) ⫺2.5 (⫺32.20, 100.35) 1.95 (⫺29.51, 16.96) 10.20 (⫺8.04, 59.77) 2.28 (⫺12.69, 32.83) 236.45 (21.07, 714.68) 0.0 (⫺26.46, 66.37) 5.26 (⫺17.17, 66.18) 13.26 (⫺10.94, 52.01) 2.06 (⫺14.43, 65.58) ⫺18.28 (⫺66.61, 218.81) 15.70 (⫺21.71, 94.17) * Values are the median (interquartile range). % change ⫽ [(parameter at week 8 or week 24 ⫺ parameters at baseline)/(parameter at baseline)] ⫻ 100. There were no significant differences in the changes between groups. IL-18 ⫽ interleukin-18; IP-10 ⫽ interferon-␥–inducible protein 10; MCP-1 ⫽ monocyte chemotactic protein 1; MIG ⫽ monokine induced by interferon-␥; IL-8 ⫽ interleukin-8; see Table 1 for additional definitions. that occurred at 8 weeks in 3 patients and at 12 weeks in the other patient. At week 24, the ACR20 response in the placebo group and the G lucidum and SMS group was not significantly different (9.1% and 15.6%, respectively; P ⬎ 0.05) and there were no significant differences at earlier time points. Patients in the G lucidum and SMS group who completed the trial had significant improvement in the pain score from week 4, and this was maintained at week 24 (mean ⫾ SD score 4.9 ⫾ 2.3 at baseline, 4.1 ⫾ 2.3 at week 4, 4.1 ⫾ 2.3 at week 16, and 3.9 ⫾ 2.5 at week 24; P ⱕ 0.05). In addition, the patient’s global assessment also improved significantly at week 4 and was also maintained at week 24 (mean ⫾ SD score 5.7 ⫾ 2.5 at baseline, 5.3 ⫾ 2.5 at week 4, 4.8 ⫾ 2.6 at week 8, 4.7 ⫾ 2.4 at week 16, and 4.7 ⫾ 2.6 at week 24; P ⬍ 0.05). Other ACR components remained unchanged in both groups (Table 2). There were no changes in FRAP and serum ascorbic acid levels after treatment in both groups (Table 2). The plasma concentration of cytokines and chemokines showed no significant differences between groups before or after treatments and no significant differences after treatment. The percentage, absolute counts, and ratio of CD4⫹/CD8⫹/NK/B lymphocytes were unchanged between groups. CD3, CD4, and CD8 lymphocyte counts were unchanged (all P ⬎ 0.05) (Table 3). However, the plasma levels of IL-18, IP-10, and IL-8 showed a declining trend in patients treated with G lucidum and SMS at week 8 and week 24, although the differences did not reach statistical significance (Table 4). In ex vivo experiments, the percentage change of IL-18 was significantly lower in the G lucidum and SMS group (Table 5). There were 22 episodes of adverse events reported by 13 patients, with 14 episodes occurring in patients receiving placebo and 8 occurring in the G lucidum and SMS group (Table 6). There were no reports of severe adverse reactions in any patients. DISCUSSION Despite claims that the extracts are of benefit to many conditions including various types of arthritis, our study is the first clinical trial to examine the effects of a combination of G lucidum and SMS in patients with RA. Our findings indicate that these compounds may have analge- Table 5. Ex vivo production of IL-6, IL-18, and chemokines upon stimulation with phytohemagglutinin and lipopolysaccharide for 24 hours* Ganoderma lucidum ⴙ SMS (n ⴝ 28) Cytokines IL-6 IL-18 Chemokines IP-10 MCP-1 MIG RANTES IL-8 Placebo (n ⴝ 30) % change at 8 weeks % change at 24 weeks % change at 8 weeks % change at 24 weeks ⫺1.64 (⫺46.86, 116.57) ⫺28.89 (⫺80.25, 111.01) ⫺27.67 (⫺77.68, 20.38) ⫺62.89 (⫺77.76, 65.87)† 0.80 (⫺30.82, 41.31) ⫺16.99 (⫺56.38, 88.57) ⫺43.53 (⫺92.42, 55.71) ⫺11.26 (⫺40.43, 57.95) ⫺11.60 (⫺41.29, 89.38) ⫺36.68 (⫺61.94, 26.24) ⫺42.62 (⫺89.53, 634.59) 13.86 (⫺62.12, 242.87) 14.49 (⫺80.62, 146.49) 7.06 (⫺23.93, 94.29)† ⫺41.95 (⫺66.12, 16.76) ⫺34.11 (⫺73.49, 185.26) ⫺11.45 (⫺74.74, 176.18) ⫺4.88 (⫺64.36, 57.88) ⫺18.18 (⫺61.51, 29.38) ⫺2.99 (⫺63.54, 90.08) 10.03 (⫺75.24, 73.66) 6.7 (⫺34.76, 105.03) 12.92 (⫺59.83, 462.77) ⫺41.53 (⫺83.22, 19.94) ⫺25.90 (⫺70.94, 46.36) ⫺43.59 (⫺81.19, ⫺10.46) 0.32 (⫺40.63, 68.09) ⫺32.09 (⫺94.56, 86.69) * Values are the median (interquartile range). % change ⫽ [(parameter at week 8 or week 24 ⫺ parameters at baseline)/(parameter at baseline)] ⫻ 100. IL-6 ⫽ interleukin-6; IL-18 ⫽ interleukin-18; IP-10 ⫽ interferon-␥–inducible protein 10; MCP-1 ⫽ monocyte chemotactic protein 1; MIG ⫽ monokine induced by interferon-␥; IL-8 ⫽ interleukin-8; see Table 1 for additional definitions. † P ⬍ 0.05 by Mann-Whitney U test versus placebo group. 1148 Li et al Table 6. Adverse events in patients treated with either Ganoderma lucidum plus SMS or placebo* Adverse events Ganoderma lucidum ⴙ SMS (n ⴝ 32) Placebo (n ⴝ 33) GI upset Palpitations Irregular period Insomnia Polyuria Headache Sweating Rash Total 4 0 0 1 0 1 2 0 8 5 3 3 1 1 0 0 1 14 * GI ⫽ gastrointestinal; see Table 1 for additional definitions. sic effects but do not appear to have any antioxidant or antiinflammatory properties. The dosage of G lucidum at 4 gm daily was recommended by practitioners of TCM, although the effective dose is not really known. Dosages of 0.5–1 gm daily have been recommended for health maintenance, 2–5 gm for chronic health conditions, and up to 15 gm daily for serious illness. The recommended G lucidum dosage in the Pharmacopoeia of the People’s Republic of China is 6 –12 gm (23). We chose a lower dose in the combination treatment based on the suggestion of the local TCM practitioner and in consideration of safety aspects because the patients were taking other medications and it is not known if interactions might occur. It is possible that higher doses may have a more beneficial effect. The toxic dose of G lucidum is also not clear but the median lethal dosage has been estimated to be between 10 and 21 gm/kg, and very high dosages (up to 38 gm/kg) have been tested in animal experiments (24,25), indicating the extracts are very safe. For SMS, the recommended dosage was 2.4 gm daily for each component, and higher dosages of up to 10 gm daily have been reported without any adverse effects in the Chinese literature. The data on the appropriate doses of SMS are more uncertain, and for both SMS and G lucidum, there are no useful biologic markers of their activity that can be measured in relation to dose and the active ingredients have not been fully characterized. The combination of SMS and G lucidum for the analgesic and antiinflammatory effects is a common practice according to our Chinese medicine colleagues. Combination was chosen based on the advice from a local Chinese medical practitioner, and our preliminary data using an in vitro test system demonstrated that G lucidum significantly inhibits the enzyme phospholipase A2 from bee venom and from hog pancreas. The lack of efficacy in terms of an antiinflammatory or immunomodulating effect in our study may be due to a number of causes. First, in retrospect, it would be useful to demonstrate in an experimental animal model that G lucidum alone and/or in combination with SMS has an inhibitory effect on phospholipase A2 in the blood and in the synovial fluid at various concentrations. The addition of SMS to G lucidum may not cause any additional inhibitory activity against phospholipase A2. Second, as- suming the compounds do inhibit phospholipase A2, it is also possible that the concentration of the active ingredient of G lucidum or SMS in the blood or synovial fluid at the current dose was insufficient to inactivate phospholipase A2 in synovial fluid. It has been shown previously that the concentration of phospholipase A2 in RA synovial fluid exceeded that in plasma (26). It is possible that the concentrations of G lucidum and SMS achieved in the RA synovial tissue and the synovial fluid were insufficient to achieve adequate inhibition of phospholipase A2. Currently, there is no information on the absorption and systemic distribution of the active ingredients of G lucidum in humans. Pharmacokinetics and pharmacodynamic assessments of G lucidum and SMS components and a dosefinding study of G lucidum would be desirable in future studies. Finally, potential interactions between G lucidum or SMS with other DMARDs should be addressed. In this study, significant analgesic effects were seen and the mixture was well tolerated. The mechanisms of the analgesic effects are unknown and deserve further study. Despite a lack of clinical antiinflammatory effects in our patients, the elevated ex vivo production of IP-10, a CXC chemokine for activated T cells and NK cells during inflammatory reactions, is of interest (22). The precise explanation for the elevated IP-10 production is unclear but this may reflect an immunoactivation effect of G lucidum. However, an elevated level of the proinflammatory cytokine IL-18 (478 pg/ml) was detected in patients with RA before treatment, a level much higher than that in healthy individuals (normal range 83–195 pg/ml) (27). Increased IL-18 has been associated with RA (28), nephrotic syndrome (29), systemic lupus erythematosus (30), and asthma (31). The significantly lower IL-18 ex vivo production seen in patients after treatment with G lucidum and SMS may suggest potential beneficial effects for patients with RA. Alternatively, this may imply a reduced induction of IL-18 at the local inflammatory sites in the patients with RA treated with G lucidum and SMS. Not withstanding the limitations of clinical trials with Chinese herbal medicines, and despite the large number of in vitro studies, we believe this is the first report of G lucidum use in humans with RA. There are 2 reports describing a reduction of herpes zoster pain in 9 patients (32,33), another report on healthy volunteers demonstrating a lack of impairment of hemostatic function (34) despite in vitro studies suggesting that G lucidum might impair hemostasis, and one study demonstrating improvement of symptoms in patients with neurasthenia (35). Our study represents the first clinical trial that explores the efficacy of these 2 herbs in a combination that is commonly used in TCM for the treatment of rheumatic disease. The results of this study do not support the clinical importance of G lucidum as an antiinflammatory agent via the inhibitory effects of phospholipase A2, and are consistent with the recent finding in a much larger double-blind, placebo-controlled study of treatment with a selective inhibitor of a secretory phospholiase A2 in patients with RA (15). Nonetheless, the significant lowering of the proinflammatory cytokine IL-18 in patients seen after treatment (36) and the analgesic properties without any demonstra- San Miao San and Ganoderma lucidum in RA 1149 ble adverse side effects are noteworthy and deserve further study. 16. AUTHOR CONTRIBUTIONS Dr. Edmund Li had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study design. Edmund Li, Tam, Tomlinson, Wachtel-Galor, Benzie, Leung. Acquisition of data. Edmund Li, Wai Ching Li, Tam, Wong, Lam. Analysis and interpretation of data. Edmund Li, Tam. Manuscript preparation. Edmund Li, Tomlinson. Statistical analysis. Tam. Assessment of cytokine and cellular measurement. Wong, Lam, Bao. REFERENCES 1. Zhu M, Chang Q, Wong LK, Chong FS, Li RC. Triterpene antioxidants from Ganoderma lucidum. Phytother Res 1999; 13:529 –31. 2. Wachtel-Galor S, Tomlinson B, Benzie IF. Ganoderma lucidum (“Lingzhi”), a Chinese medicinal mushroom: biomarker responses in a controlled human supplementation study. Br J Nutr 2004;91:263–9. 3. Wachtel-Galor S, Szeto YT, Tomlinson B, Benzie IF. Ganoderma lucidum (‘Lingzhi’): acute and short-term biomarker response to supplementation. Int J Food Sci Nutr 2004;55:75– 83. 4. Bao XF, Wang XS, Dong Q, Fang JN, Li XY. Structural features of immunologically active polysaccharides from Ganoderma lucidum. Phytochemistry 2002;59:175– 81. 5. Kim RS, Kim HW, Kim BK. Suppressive effects of Ganoderma lucidum on proliferation of peripheral blood mononuclear cells. Mol Cells 1997;7:52–7. 6. Tasaka K, Akagi M, Miyoshi K, Mio M, Makino T. Antiallergic constituents in the culture medium of Ganoderma lucidum. I. Inhibitory effect of oleic acid on histamine release. Agents Actions 1988;23:153– 6. 7. Lei LS, Lin ZB. Effect of Ganoderma polysaccharides on T cell subpopulations and production of interleukin 2 in mixed lymphocyte response. Yao Xue Xue Bao 1992;27: 331–5. 8. Haak-Frendscho M, Kino K, Sone T, Jardieu P. Ling Zhi-8: a novel T cell mitogen induces cytokine production and upregulation of ICAM-1 expression. Cell Immunol 1993;150: 101–13. 9. Lai KN, Chan LY, Tang SC, Leung JC. Ganoderma extract prevents albumin-induced oxidative damage and chemokines synthesis in cultured human proximal tubular epithelial cells. Nephrol Dial Transplant 2006;21:1188 –97. 10. Hu H, Ahn NS, Yang X, Lee YS, Kang KS. Ganoderma lucidum extract induces cell cycle arrest and apoptosis in MCF-7 human breast cancer cell. Int J Cancer 2002;102: 250 –3. 11. Sliva D, Sedlak M, Slivova V, Valachovicova T, Lloyd FP, Ho NW. Biologic activity of spores and dried powder from Ganoderma lucidum for the inhibition of highly invasive human breast and prostate cancer cells. J Altern Complement Med 2003;9:491–7. 12. Wang SY, Hsu ML, Hsu HC, Tzeng CH, Lee SS, Shiao MS, et al. The anti-tumor effect of Ganoderma lucidum is mediated by cytokines released from activated macrophages and T lymphocytes. Int J Cancer 1997;70:699 –705. 13. Yuen JW, Gohel MD. Anticancer effects of Ganoderma lucidum: a review of scientific evidence. Nutr Cancer 2005; 53:11–7. 14. Bomalaski J, Clark M. Phospholipase A2 and arthritis. Arthritis Rheum 1993;36:190 – 8. 15. Bradley JD, Dmitrienko AA, Kivitz AJ, Gluck OS, Weaver AL, Wiesenhutter C, et al. A randomized, double-blinded, place- 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. bo-controlled trial of LY333013, a selective inhibitor of group II secretory phospholipase A2, in the treatment of rheumatoid arthritis. J Rheumatol 2005;32:417–23. Garcia Pastor P, de Rosa S, de Giulio A, Paya M, Alcaraz M. Modulation of acute and chronic inflammatory processes by cacospongionolide B, a novel inhibitor of human synovial phospholipase A2. Br J Pharmacol 1999;126:301–11. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315–24. Koh ET, Seow A, Pong LY, Koh WH, Chan L, Howe HS, et al. Cross cultural adaptation and validation of the Chinese Health Assessment Questionnaire for use in rheumatoid arthritis. J Rheumatol 1998;25:1705– 8. Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M, Fried B, et al. The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. Arthritis Rheum 1993;36:729 – 40. Benzie I, Strain JJ. Ferric reducing/antioxidant power assay: direct measure of total antioxidant activity of biological fluids and modified version for simultaneous measurement of total antioxidant power and ascorbic acid concentration. Methods Enzymol 1999;299:15–27. Benzie I, Strain J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: the FRAP assay. Anal Biochem 1996;239:70 – 6. Tang NL, Chan PK, Wong CK, To KF, Wu AK, Sung YM, et al. Early enhanced expression of interferon-inducible protein-10 (CXCL-10) and other chemokines predicts adverse outcome in severe acute respiratory syndrome. Clin Chem 2005;51:2333– 40. Compiled by the State Pharmacopoeia Commission of P. R. China. Parmacopoeia of the People’s Republic of China. Beijing; Chemical Industry Press: 2000. Chiu SW, Wang ZM, Leung TM, Moore D. Nutritional value of Ganoderma extract and assessment of its genotoxicity and antigenotoxicity using comet assays of mouse lymphocytes. Food Chem Toxicol 2000;38:173– 8. Chang R. Effective dose of Ganoderma in humans. In: Buchanan PK, Hseu RS, Moncalvo JM, editors. Proceedings of the Contributed Symposium 59A, B of the 5th International Mycological Congress. Taipei; 1994. p. 101–13. Pruzanski W, Vadas P, Stefanski E, Urowitz M. Phospholipase A2 activity in sera and synovial fluids in rheumatoid arthritis and osteoarthritis: its possible role as a proinflammatory enzyme. J Rheumatol 1985;12:211– 6. Wong CK, Ho CY, Li EK, Tam LS, Lam CW. Elevated production of interleukin-18 is associated with renal disease in patients with systemic lupus erythematosus. Clin Exp Immunol 2002;130:345–51. Sato M, Takemura M, Shinohe R, Koishi H, Morita T, Seishima M. Clinical significance of serum IL-18 determination in rheumatoid arthritis. Rinsho Byori 2004;52:109 –14. In Japanese. Matsumoto K, Kanmatsuse K. Elevated interleukin-18 levels in the urine of nephrotic patients. Nephron 2001;88: 334 –9. Wong CK, Ho CY, Li EK, Lam CW. Elevation of proinflammatory cytokine (IL-18, IL-17, IL-12) and Th2 cytokine (IL-4) concentrations in patients with systemic lupus erythematosus. Lupus 2000;9:589 –93. Wong CK, Ho CY, Ko FW, Chan CH, Ho AS, Hui DS, et al. Proinflammatory cytokines (IL-17, IL-6, IL-18 and IL-12) and Th cytokines (IFN-␥, IL-4, IL-10 and IL-13) in patients with allergic asthma. Clin Exp Immunol 2001;125:177– 83. Hijikata Y, Yamada S. Effect of Ganoderma lucidum on postherpetic neuralgia. Am J Chin Med 1998;26:375– 81. Hijikata Y, Yasuhara A, Sahashi Y. Effect of an herbal formula containing Ganoderma lucidum on reduction of herpes zoster pain: a pilot clinical trial. Am J Chin Med 2005;33:517–23. 1150 34. Kwok Y, Ng KF, Li CC, Lam CC, Man RY. A prospective, randomized, double-blind, placebo-controlled study of the platelet and global hemostatic effects of Ganoderma lucidum (Ling-Zhi) in healthy volunteers. Anesth Analg 2005;101: 423– 6. 35. Tang W, Gao Y, Chen G, Gao H, Dai X, Ye J, et al. A randomized, double-blind and placebo-controlled study of a Gano- Li et al derma lucidum polysaccharide extract in neurasthenia. J Med Food 2005;8:53– 8. 36. Xi Bao Y, Kwok Wong C, Kwok Ming Li E, Shan Tam L, Chung Leung P, Bing Yin Y, et al. Immunomodulatory effects of lingzhi and san-miao-san supplementation on patients with rheumatoid arthritis. Immunopharmacol Immunotoxicol 2006;28:197–200.