Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
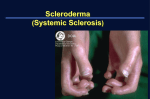
Joint Bone Spine 74 (2007) e1ee8 http://france.elsevier.com/direct/BONSOI/ Review Raynaud’s phenomenon Martine Gayraud* Internal Medicine Department, Institut Mutualiste Motnsouris, 42 boulevard Jourdan, 75014 Paris, France Received 2 November 2005; accepted 26 July 2006 Available online 4 December 2006 Abstract Vascular acrosyndromes constitute a common reason for physician visits. They are associated with connective tissue disease; for example, 90% of patients with scleroderma experience Raynaud’s phenomenon. The rheumatologist must strive to establish the diagnosis, to identify a potential underlying cause, and to prescribe effective treatment when the symptoms are incapacitating. Raynaud’s phenomenon is the acrosyndrome most commonly encountered by rheumatologists. The diagnosis of Raynaud’s phenomenon rests on clinical grounds. Nailfold capillaroscopy and immunological tests are useful chiefly for determining the cause. Calcium-channel antagonists are the treatment of reference for Raynaud’s phenomenon. Drugs introduced over the last few years for severe refractory forms include prostacyclin and its derivatives, endothelin receptor antagonists, and phosphodiesterase inhibitors. These drugs were developed as a result of new knowledge on the pathogenesis of Raynaud’s phenomenon. Acrocyanosis, which is extremely common, and erythromelalgia are the other main vascular acrosyndromes. Ó 2006 Elsevier Masson SAS. All rights reserved. Keywords: Raynaud’s phenomenon; Scleroderma; Calcium-channel antagonists 1. Definition In 1862, Maurice Raynaud described a paroxysmal phenomenon that included three phases: ischemia, with pallor of the digits due to vasoconstriction of the digital arteries, precapillary arteries, and cutaneous arteriovenous shunts; hyperemia with redness of the digits; and a return to normal (Fig. 1). Whereas the ischemic phase is required for the diagnosis, the hyperemic phase may be lacking. The abnormalities usually spare the thumb but involve most of the other digits, although they may start in a limited number of digits. The nose, ears, and tongue may be affected. The attack resolves within an hour after the end of cold exposure [2,3]. Raynaud’s phenomenon is associated with migraine and chest pain (usually from the chest wall, an association with spastic angina being controversial) [4]. 2. Epidemiology Raynaud’s phenomenon may be primary or secondary. It may occur as the first manifestation of an underlying disease, * Tel.: þ33 1 56 61 67 24; fax: þ33 1 56 61 67 29. E-mail address: [email protected] most notably scleroderma [1e3]. A 7-year study conducted in Caucasians in the United States showed baseline prevalences of 11% in women and 8% in men and incidences of 2.2% in women and 1.5% of men [5]. The rate of remission during the study period was 64% in both women and men [5]. Variations in prevalence occur across climates [6]. In a study of teenagers, the prevalence was 15% with a predominance in females [7]. The attacks occur when the ambient temperature drops below a cutoff, which is specific of each individual patient. The cutoff temperature may be relatively high, with attacks occurring even during the summer months. 3. Pathogenesis New insights into the pathogenesis of Raynaud’s phenomenon have led to the development of specific treatment approaches [8] (Fig. 2). Primary Raynaud’s phenomenon is related to functional alterations alone. Secondary Raynaud’s phenomenon, in contrast, also reflects structural microvascular abnormalities, most notably in patients with scleroderma or vibration injury [8,9]. Factors that promote vasoconstriction include a2-adrenoceptor overactivity, increased endothelin-1 production [10] 1297-319X/$ - see front matter Ó 2006 Elsevier Masson SAS. All rights reserved. doi:10.1016/j.jbspin.2006.07.002 e2 M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 α2 Adrenoceptor activity smooth muscle cells α blockers Selective α2c adrenoceptor blockade endothelin angiotensin II tyrosine kinase activity serotonin neuropeptides vasodilators - CGRP - VIP - Neurokinine A - Substance P nerve fibers CGRP Phosphodiesterase inhibitors Calcium-channel antagonists NO prostacyclin or resistance endothelial cells Endothelin-1 antagonists Angiotensin II receptor antagonists Selective serotonin reuptake inhibitors L arginine Transdermal NO Phosphodiesterase inhibitors Calcium-channel antagonists VASOCONSTRICTION VASODILATATION Intravascular mechanisms - platelet aggregation leukocyte activation erythrocyte deformation hyperviscosity Fibrinolytic agents, antiplatelet agents, smoking cessation Fig. 1. (a, b) Ischemic and hyperemic phases of Raynaud’s phenomenon. and tyrosine kinase overactivity in endothelial cells [11,12]. Furthermore, there is probably a role for angiotensin II and serotonin. The endothelium releases vasodilating substances such as nitric oxide (NO) and prostacyclin. L-arginine, which increases NO production, has been reported to improve Raynaud’s phenomenon [13]. Loss of nerve fibers supplying the capillaries leads to decreased production of vasodilating substances such as neuropeptides (calcitonin gene-related peptide, substance P, neurokinin A, neuropeptide Y, and vasointestinal peptide) whose effects are mediated by NO production. The role for intravascular alterations is less clear. 4. Identifying the cause Primary Raynaud’s phenomenon, also called Raynaud’s disease, is defined as Raynaud’s phenomenon with no identifiable underlying disease. A family history supports a diagnosis of Raynaud’s disease, particularly in younger individuals [14]. Among women with Raynaud’s phenomenon, 85% have the primary form and 15% the secondary form, whereas the distribution is balanced in men. Table 1 lists the diagnostic criteria for primary Raynaud’s phenomenon. The causes of secondary Raynaud’s phenomenon are listed in Table 2. In a study of 639 patients, 12.6% developed Fig. 2. Pathogenic mechanisms and therapeutic targets in Raynaud’s phenomenon. symptoms of an associated disease within 24 months [15]. Of 142 patients followed up for 12.4 years on average, 14.1% experienced progression to connective tissue disease [14]. Capillaroscopy, tests for antinuclear factor, and tests for inflammation should be performed routinely in patients with Raynaud’s phenomenon [9]. Capillaroscopy is crucial [16,17]. It consists in examination of the nailfold capillaries under a light microscope (10 to 300 magnification) with cold light illumination. Capillaroscopy is difficult to perform in patients who have pigmented thick skin (manual laborers). Nailfold capillaries are normally horizontal. Capillary enlargement, which is the most specific finding, occurs in three connective tissue diseases: scleroderma, mixed connective tissue disease, and dermatomyositis (Figs. 3, 4). The enlarged Table 1 Diagnostic criteria for primary Raynaud’s syndrome (Raynaud’s disease) Attacks triggered by exposure to cold and/or stress Symmetric bilateral involvement Absence of necrosis No detectable underlying cause Normal capillaroscopy findings Normal laboratory tests for inflammation Negative tests for antinuclear factors M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 e3 Table 2 Causes of secondary Raynaud’s phenomenon Prevalence CONNECTIVE TISSUE DISEASE DRUGS AND TOXIC AGENTS Systemic sclerosis CREST syndrome Mixed connective tissue disease SLE Sjögren’s syndrome Dermatomyositis 90e95% 100% 70e85% 10e30% 5e15% 15e35% b-Blockers (including those in ocular solutions) Ergot derivatives Cancer chemotherapy Cyclosporine Interferons a and b Exposure to vinyl polychloride Cocaine Smoking (probable) ENDOCRINE DISORDERS Hypothyroidism Pheochromocytoma Carcinoid syndrome TRAUMA (unilateral Raynaud’s) Vibration injury Ulnar aneurysm (hypothenar hammer syndrome) Repetitive stress injury (thoracic outlet syndrome) ARTERIAL DISEASE (often unilateral) Thromboangiitis obliterans Atheroma Peripheral embolism Vasculitides (giant-cell arteritis, Takayasu) HEMATOLOGICAL DISORDERS AND CANCER Cryoglobulinemia Cold agglutinin disease Myeloproliferative and lymphoproliferative disorders Cancers capillaries may be visible to the naked eye (Fig. 5). Digital ulcers may develop, making the diagnosis obvious to inspection (Figs. 6, 7). Joint lesions are common in patients who have digital ulcers. Fig. 3. Enlarged capillaries in a patient with scleroderma. Fig. 4. Capillaroscopic abnormalities (petechiae, edema, and capillary loop enlargement). Unilateral Raynaud’s phenomenon suggests an arterial lesion or an occupational injury [3,18,19]. Vibration injury occurs in workers who use jackhammers, chisels, rivet presses, drills, compacters, chain saws, buffers, or sanders. Longer exposure times and vibration frequencies in the 25e250 Hz range are associated with an increased risk of vibration injury [19]. Hypothenar hammer syndrome is related to dysplasia of the ulnar artery anterior to the superficial palmar arch. An aneurysm develops then undergoes thrombosis, and emboli are released. Construction workers, carpenters, metal workers, and mechanics are at highest risk. Hypothenar hammer syndrome has been reported in association with several sports (e.g., karate, mountain biking, hockey, and golf). Vascular Doppler ultrasound and angiography establish the diagnosis [18] (Fig. 8). Workers with hypothenar hammer syndrome are eligible for compensation (in France, Table 69 for salaried workers and number 29 for farmers). Thoracic outlet syndrome, which manifests chiefly as neurological symptoms, is associated with Raynaud’s phenomenon in 45% of cases. The link between vessel and nerve compression in the thoracic outlet and Raynaud’s phenomenon is unclear. When the diagnosis is suspected, a radiograph of the cervical spine and clavicles should be obtained to look for a cervical rib or elongated Fig. 5. Enlarged capillaries visible around the nails. M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 e4 Fig. 6. Digital ulcers in a patient with scleroderma. transverse process [20]. Arterial lesions due to mechanical factors or inflammatory disease (vasculitis or thromboangiitis obliterans (Fig. 9) manifest chiefly as symptoms of digital ischemia. Fig. 10 summarizes the diagnostic process. 5. Treatment Pharmacotherapy is usually unnecessary in patients with primary Raynaud’s phenomenon [21]. 5.1. Functional factors Exposure to cold should be avoided. Warm loose clothing with thermal gloves and socks is often sufficient. Appropriate clothing can often be found in mountain sports stores. Hand Fig. 8. Digital arteriogram: obstruction of the ulnar artery and interdigital arteries of the first and second rays. warmers are useful. Patients should not use medications or other substances that induce vasoconstriction, such as ergot derivatives, b-blockers, caffeine, and nasal vasoconstrictors [2,3,21]. Smoking cessation is essential in patients with thromboangiitis obliterans. 5.2. Medications (Fig. 2) 5.2.1. Calcium-channel antagonists Calcium-channel antagonists are the most widely used medications in patients with Raynaud’s phenomenon [2,3,21]. Fig. 7. Phalangeal tuft resorption in a patient with scleroderma. Fig. 9. Necrosis of the toes in a patient with thromboangiitis obliterans. M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 History: - Intermittent attacks - Ischemic phase - Triggered by cold and stress e5 Other acrosyndromes: - erythromelalgia - acrocyanosis - frostbite - carpal tunnel syndrome Raynaud's phenomenon - Drugs or toxic agents - Work-related exposures - Clinical evidence of connective tissue disease - Malignancy - Evidence of endocrine disease - Evidence of vascular disease (pulses, Allen's maneuver) - Antinuclear factors - Capillaroscopy Drugs Endocrine diseases Negative Positive Cryoglobulinemia Blood disorders Secondary Raynaud's phenomenon Evidence of connective tissue disease Immunologic workup X-rays hands and chest Proteinuria Capillary enlargement yes Raynaud's disease likely (2 years' follow-up required) no Scleroderma Mixed connective tissue disease Dermatomyositis Unilateral attacks Abnormalities of peripheral vessels X-rays chest, cervical spine Doppler Angiography AngioCT or MRI Echocardiography Lupus Rheumatoid arthritis Sjögren's syndrome Polymyositis Work-related Embolism Vasculitides Atheroma Thoracic outlet syndrome Arteriovenous aneurysm Shunt for dialysis Fig. 10. Diagnosis of Raynaud’s phenomenon and investigations for an underlying cause. In addition to relieving vascular spasm, they decrease superoxide anion production by monocytes and limit the progression of endothelial lesions in patients with scleroderma [22,23]. A meta-analysis of 17 studies showed that calcium-channel antagonist therapy was associated with a 33% reduction in attack severity and with a reduction in the number of attacks from 5 to 2.8/week [24]. In 130 patients given nifedipine 30 mg b.i.d. for 1 year, the number of attacks decreased by 66%, and 15% of patients experienced adverse effects requiring discontinuation of the drug [25]. Similar results were obtained in patients who had Raynaud’s phenomenon associated with scleroderma [26]. Amlodipine is as effective as nifedipine, diltiazem is less effective, and verapamil has no effect [27]. Delayed-release once-daily formulations have been suggested based on their better safety profile. The dosage should be increased gradually until a response is achieved. Raynaud’s phenomenon often requires a higher dosage than hypertension (up to 60 mg of nifedipine or 20 mg of amlodipine). 5.2.2. Nitrate derivatives Evidence that nitrate derivatives administered transcutaneously may improve Raynaud’s phenomenon comes from only a small number of studies [3,28]. The gel is no longer marketed in France. A preparation containing 2 g of nitroglycerine per 100 g of vaseline and lanolin ointment with 18 g of lactose monohydrate can be used. e6 M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 5.2.3. a-Adrenoceptor antagonists Prazosine, which inhibits the a1-adrenoceptors, has been proved effective [3]. A selective inhibitor of the a2c-adrenoceptors, which play a pivotal role in vessel reactivity, was found to improve digital blood flow in patients with scleroderma who were exposed to cold temperatures [29]. used in a few patients to treat digital ulcers associated with severe Raynaud’s phenomenon (due to connective tissue disease or cancer) that was unresponsive to calcium-channel antagonists and ilomedin. Improvements were noted within a few days, and tolerance was good [46e48]. Similar results were obtained with tadalafil [49,50]. 5.2.4. Buflomedil and naftidrofuryl The effectiveness of these agents remains controversial, and the number of studies is small [3,30,31]. However, buflomedil is widely used in everyday practice. 5.2.8. Selective serotonin reuptake inhibitors Serotonin has vasoconstricting effects. This mediator is released by nerve terminals and by platelets undergoing activation. The selective serotonin reuptake inhibitor fluoxetine induced improvements in small studies. Fluoxetine (20 mg/ day) was significantly more effective than nifedipine (40 mg/ day) in decreasing attack frequency and severity, and the difference was particularly marked in the subgroup with primary Raynaud’s phenomenon [51]. 5.2.5. Prostaglandins Prostaglandins are potent vasodilating agents that also inhibit platelet aggregation, decrease leukocyte margination, and exert fibrinolytic effects [2,3]. Ilomedin, a synthetic analog of prostaglandin I2, has been evaluated in Raynaud’s phenomenon secondary to connective tissue disease [32e36]. The drug was given as 6-h infusions in doses of 0.5 to 2 ng/kg/min for 3 to 6 days [32]. In a study of 114 patients with scleroderma, ilomedin therapy decreased attack frequency and severity and improved skin healing, compared to a placebo [32]. The 0.5 ng/kg/min and 2 ng/kg/min dosages were similarly effective, and the lower dosage induced fewer side effects (headache, hot flashes, and gastrointestinal symptoms). Despite the short half-life of ilomedin, the beneficial effects lasted several weeks, suggesting endothelial and cellular effects in addition to the vasodilating effect [33]. In comparisons of ilomedin infusions to nifedipine per os in patients with scleroderma, ilomedin was at least as effective as nifedipine [34,35]. Oral prostaglandins have not been proved effective [36]. A placebo-controlled study of beraprost for 6e12 months in 107 patients with digital ulcers showed no difference in attack frequency or severity but revealed a trend toward decreased ulcer size [37]. 5.2.6. Endothelin receptor antagonists Endothelin, which is released by endothelial cells, induces vasoconstriction. Endothelin receptor antagonists are approved for use in primary arterial hypertension and in arterial hypertension associated with scleroderma functional class III [38,39]. In a placebo-controlled study of bosentan 25 mg b.i.d., there were fewer new ulcers with the drug, and this effect was most noticeable in patients who had numerous ulcers at baseline [40]. Hand function improved, but there was no effect on healing of preexisting ulcers [40]. Other studies showed rapid ulcer healing, even in patients who were previously treated with ilomedin [41e44]. 5.2.7. Phosphodiesterase inhibitors The phosphodiesterase-5 inhibitor sildenafil increases guanosine monophosphate levels in vascular smooth muscle cells, inducing vasodilation. Sildenafil, which is used to treat erectile dysfunction, has been evaluated in primary and sclerodermaassociated pulmonary arterial hypertension [45]. The results showed that sildenafil improved Raynaud’s phenomenon. Sildenafil (12.5 to 150 mg once to three times a day) has been 5.2.9. Angiotensin II receptor antagonists Results obtained with angiotensin II receptor antagonists to treat Raynaud’s phenomenon have been inconclusive. Losartan 50 mg/day was better than nifedipine 40 mg/day in decreasing attack frequency and severity and also improved vascular parameters, most notably in patients who had primary Raynaud’s phenomenon [52]. 5.2.10. Fibrinolytic agents, anticoagulants, and platelet inhibitors The evidence is not sufficient to support the use of these medications. Controlled studies are needed to determine their role in Raynaud’s phenomenon. 5.2.11. Medications approved for use in France Nifedipine and ilomedin are approved for the treatment of Raynaud’ s phenomenon. Several vasodilating agents are approved as adjunctive treatments; they include buflomedil, naftidrofuryl, and dihydroergocriptine. Other medications are not approved for Raynaud’s phenomenon and should be used only when the condition is severe and refractory to the above-listed drugs, after a careful review of the literature. Ilomedin is costly and is reimbursed by the French healthcare system when used in hospitalized patients. The 3- to 6-day treatment duration is well-suited to 1-week hospitalization. 5.3. Nonpharmacological treatments The level of proof is inadequate to support the use of biofeedback, acupuncture, low-frequency laser therapy, cord stimulation, or sympathetic block [2,3,21,53]. Surgery is rarely appropriate, despite the introduction of thoracoscopy. Thoracoscopic sympathectomy induced rapid improvements, with healing of the ulcers within 1 month, but the recurrence rate was high (82%) [54]. Digital sympathectomy with periarterial denervation also carried a high recurrence rate and also induced postoperative complications in 37% of patients with scleroderma [55]. M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 Acknowledgments We are grateful to Professors Guillevin and Hachulla for allowing us to reproduce Figs. 1, 6, and 7. References [1] Carpentier PH. Définition et épidémiologie des acrosyndromes vasculaires. Rev Prat 1998;46:1641e6. [2] Block JA, Sequeira W. Raynaud’s phenomenon. Lancet 2001;357: 2042e8. [3] Wigley FM. Raynaud’s phenomenon. N Engl J Med 2002;347:1001e8. [4] O’Keefe ST, Tsapatsaris NP, Beetham WP. Increased prevalence of migraine and chest pain in patients with primary Raynaud’s disease. Ann Intern Med 1992;116:985e9. [5] Suter LG, Murabito JM, Felson DT, Fraenkel L. The incidence and natural history of Raynaud’s phenomenon in the community. Arthritis Rheum 2005;52:1259e63. [6] Olsen N, Nielsen SL. Prevalence of primary Raynaud phenomena in young females. Scand J Clin Lab Invest 1978;37:761e4. [7] Jones GT, Herrick AL, Woodham SE, Baildam E, Macfarlane GI, Silman AJ. Occurrence of Raynaud’s phenomenon in children aged 1215 years. Arthritis Rheum 2003;48:3518e23. [8] Herrick AL. Pathogenesis of Raynaud’s phenomenon. Rheumatology 2005;44:587e96. [9] Flavahan NA, Flavahan S, Mitra S, Chotani MA. The vasculopathy of Raynaud’s phenomenon and scleroderma. Rheum Dis Clin North Am 2003;29:275e91. [10] Mayes MD. Endothelin and endothelin receptor antagonists in systemic rheumatic disease. Arthritis Rheum 2003;48:1190e9. [11] Furspan PB, Chatterjee S, Mayes MD, Freedman RR. Coolinginduced contraction and protein tyrosine kinase activity of isolated arterioles in secondary Raynaud’s phenomenon. Rheumatology 2005; 44:488e94. [12] Furspan PB, Chatterjee S, Freedman RR. Increased tyrosine phosphorylation mediates the cooling-induced contraction and increased vascular reactivity of Raynaud’s disease. Arthritis Rheum 2004;50:1578e85. [13] Generini S, Seibold JR, Matucci-Cerinic M. Estrogens and neuropeptides in Raynaud’s phenomenon. Rheum Dis Clin North Am 2005;31:177e86. [14] Planchon B, Pistorius MA, Beurrier P, de Faucal P. Primary’s Raynaud’s phenomenon. Age of onset and pathogenesis in a prospective study of 424 patients. Angiology 1994;45:677e86. [15] Ziegler S, Brunner M, Eigenbauer E, Minar E. Long-term outcome of primary’s Raynaud’s phenomenon and its conversion to connective tissue disease: a 12-year retrospective patient analysis. Scand J Rheumatol 2003;32:343e7. [16] Manmarino E, Pasqualini L, Fedeli F, Scricciolo V, Innocente S. Nailfold capillaroscopy in the screening and diagnosis of Raynaud’s phenomenon. Angiology 1994;45:37e42. [17] Cutolo M, Grassi W, Matucci-Cerinic M. Raynaud’s phenomenon and the role of capillaroscopy. Arthritis Rheum 2003;48:3023e30. [18] Hatron PY, Frimat P, Hachulla E. Phénomènes de Raynaud d’origine professionnelle. Rev Prat 1998;48:1653e8. [19] Boillat MA, Thorens B. Acrosyndromes et maladies professionnelles: épidémiologie et prévention de la maladie des engins vibrants. Rev Med Suisse Romande 1992;112:405e7. [20] Hachulla E, Gillard J, Duquesnoy B. Clinique du syndrome de la traversée cervico-thoraco-brachiale. Rev Med Int 1999;5(Suppl):464e7. [21] Belch JJ, Ho M. Pharmacotherapy of Raynaud’s phenomenon. Drugs 1996;52:682e95. [22] Allanore Y, Kahan A. Treatment of systemic sclerosis. Joint Bone Spine 2006;73:363e8. [23] Allanore Y, Borderie D, Lemarechal H, Ekindjian OG, Kahan A. Acute and sustained effects of dihydropyridine-type calcium channel antagonists on oxidative stress in systemic sclerosis. Am J Med 2004;116: 595e600. e7 [24] Thompson AE, Pope JE. Calcium channel blockers for primary’s Raynaud’s phenomenon: a metaanalysis. Rheumatology 2005;44:145e50. [25] Raynaud’s Treatment Study Investigators. Comparison of sustained-release nifedipine and temperature biofeedback for treatment of primary Raynaud’s phenomenon. Results from a randomized clinical trial with 1-year follow-up. Arch Intern Med 2000;160:1101e8. [26] Thompson AE, Shea B, Welch V, Fenlon D, Pope JE. Calcium-channel blockers for Raynaud’s phenomenon in systemic sclerosis. Arthritis Rheum 2001;44:1841e7. [27] Hummers LK, Wigley FM. Management of Raynaud’s phenomenon and digital ischemic lesions in scleroderma. Rheum Dis Clin North Am 2003;29:293e313. [28] The LS, Manning J, Moore T, Tully MP, O’Reilly D, Jayson MIV. Sustained-release transdermal glyceryl trinitrate patches as treatment for primary and secondary Raynaud’s phenomenon. Br J Rheumatol 1995;34:636e41. [29] Wise RA, Wigley FM, White B, Leatherman G, Zhong J, Krasa H, et al. Efficacy and tolerability of a selective a2c-adrenergic receptor blocker in recovery from cold-induced vasospasm in scleroderma patients. Arthritis Rheum 2004;50:3994e4001. [30] Le Quintrec P, Lefebvre ML. Double-blind placebo-controlled trial of buflomedil in the treatment of Raynaud’s phenomenon: six-month followup. Angiology 1991;42:289e95. [31] Davinroy M, Mosnier M. Evaluation clinique en double-insu du naftidrofuryl dans le phénomène de Raynaud. Sem Hop Paris 1993;69:1322e6. [32] Wigley FM, Wise RA, Seibold JR, McCloskey DA, Kujala G, Medsger Jr TA, et al. Intravenous iloprost infusion in patients with Raynaud phenomenon secondary to systemic sclerosis. Ann Intern Med 1994;120:199e206. [33] Torlay HI, Madock R, Capell HA, Brouwer RM, Maddison PJ, Black CM, et al. A double blind, randomised, multicentre comparison of two doses of intravenous iloprost in the treatment of Raynaud’s phenomenon secondary to connective tissue diseases. Ann Rheum Dis 1991;50:800e4. [34] Scorza R, Caronni M, Mascagni B, Berruti V, Bazzi S, Micaleff E, et al. Effects of long-term cyclic iloprost therapy in systemic sclerosis with Raynaud’s phenomenon. A randomized controlled study. Clin Exp Rheumatol 2001;19:503e8. [35] Rademaker M, Cooke ED, Almond NE, Beacham JA, Smith RE, Mant TG, et al. Comparison of intravenous infusions of iloprost and oral nifedipine in treatment of Raynaud’s phenomenon in patients with systemic sclerosis: a double blind randomized study. BMJ 1989;298:561e4. [36] Wigley FM, Korn JH, Czuka ME, Medsger TA, Rothfield NF, Ellman M, et al. Oral iloprost treatment in patients with Raynaud’s phenomenon secondary to systemic sclerosis. Arthritis Rheum 1998;41:670e7. [37] Vayssairat M. Preventive effect of an oral prostacyclin analog, beraprost sodium, on digital necrosis in systemic sclerosis. French Microcirculation Multicenter Group for the Study of Vascular Acrosyndromes. J Rheumatol 1999;26:2173e8. [38] Humbert M, Sitbon O, Simonneau G. Drug therapy: treatment of pulmonary hypertension. N Engl J Med 2004;351:1425e36. [39] Braun-Moscovici Y, Nahir AM, Balbir-Gurman A. Endothelin and pulmonary arterial hypertension. Semin Arthritis Rheum 2004;34:442e53. [40] Korn JH, Mayes M, Matucci Cerinic M, Rainisio M, Pope J, Hachulla E, et al. Digital ulcers in systemic sclerosis. Prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum 2004;50:3985e93. [41] Ramos-Cazals M, Brito-Zeron P, Nardi N, Claver G, Risco G, Parraga FD, et al. Successful treatment of severe Raynaud’s phenomenon with bosentan in four patients with systemic sclerosis. Rheumatology 2004;43:1454e6. [42] Snyder MJ, Jacobs MR, Grau RG, Wilkes DS, Knox KS. Resolution of severe digital ulceration during a course of bosentan therapy. Ann Intern Med 2005;142:802e3. [43] Humbert M, Cabane J. Successful treatment of systemic sclerosis digital ulcers and pulmonary arterial hypertension with endothelin receptor antagonist bosentan. Rheumatology 2003;42:191e3. [44] Font J, Ramos-Cazals M, Nardi N, Brito-Zeron P, Aguilo S, Belenguer R. One-year prospective follow-up of bosentan treatment for severe e8 [45] [46] [47] [48] [49] M. Gayraud / Joint Bone Spine 74 (2007) e1ee8 Raynaud’s phenomenon associated with systemic sclerosis. Ann Rheum Dis 2005;64(III):278. Watanabe H, Ohashi K, Takeuski K, Yamashita K, Yokoyama T, Ttran Q, et al. Sildenafil for primary and secondary pulmonary hypertension. Clin Pharmacol Ther 2002;71:398e402. Kumana CR, Cheung GTY, Lau CS. Severe digital ischaemia treated with phosphodiesterase inhibitors. Ann Rheum Dis 2004;63: 1522e4. Rosenkranz S, Diet F, Karasch T, Weibrauch J, Wasserman K, Erdman E. Sildanefil improved pulmonary hypertension and peripheral blood flow in a patient with scleroderma-associated lung fibrosis and the Raynaud phenomenon. Ann Int Med 2003;139:871e3. Kumar N, Allen J, Murray A, Griffiths B. A pilot study assessing the response of a single dose of sildenafil citrate in the treatment of Raynaud’s phenomenon in patients with systemic sclerosis. Rheumatology 2004; 2(Suppl):97. Gore J, Silver R. Oral sildenafil for the treatment of Raynaud’s phenomenon and digital ulcers secondary to systemic sclerosis. Ann Rheum Dis 2005;64:1387. [50] Kamata Y, Kaminura T, Iwamoto M, Minota S. Comparable effects of sildenafil citrate and alprostadil on severe Raynaud’s phenomenon in a patient with systemic sclerosis. Clin Exp Dermatol 2005;30:451. [51] Coleiro B, Marshall SE, Denton CP, Howell K, Blann A, Welsch KJ, et al. Treatment of Raynaud’s phenomenon with the selective serotonin reuptake inhibitor fluoxetine. Rheumatology 2001;40:1038e43. [52] Dziadzio M, Denton CP, Smith R, Howell K, Blann A, Bowers E, et al. Losartan therapy for Raynaud’s phenomenon and scleroderma. Arthritis Rheum 1999;42:2646e55. [53] Hirschi M, Katzenschlager R, Francesconi C, Kundi M. Low level laser therapy in primary’s Raynaud’s phenomenon- Results of a placebo controlled double blind intervention study. J Rheumatol 2004;31: 2408e12. [54] Matsumoto Y, Ueyama T, Endo M, Sasaki H, Kasashima F, Abe Y, et al. Endoscopic thoracic sympathicotomy for Raynaud’s phenomenon. J Vasc Surg 2002;36:57e61. [55] Kotsis SV, Chung KC. A systematic review of the outcomes of digital sympathectomy for treatment of chronic digital ischemia. J Rheumatol 2003;30:1788e92.