Survey
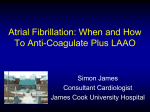
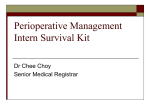
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Anticoagulation Management in the Ambulatory Surgical Setting 2.7 DIANA HILL EISENSTEIN, MSN, RN, FNP-BC, CNOR www.aorn.org/CE ABSTRACT Many people receiving maintenance anticoagulation therapy require surgery each year in ambulatory surgery centers. National safety organizations focus attention toward improving anticoagulation management, and the American College of Chest Physicians has established guidelines for appropriate anticoagulation management to balance the risk of thromboembolism when warfarin is discontinued with the risk of bleeding when anticoagulation therapy is maintained. The guidelines recommend that patients at high or moderate risk for thromboembolism should be bridged with subcutaneous low-molecular-weight heparin or IV unfractionated heparin with the interruption of warfarin, and low-risk patients may require subcutaneous lowmolecular-weight heparin or no bridging with the interruption of warfarin. The guidelines recommend the continuation of warfarin for patients who are undergoing minor dermatologic or dental procedures or cataract removal. The literature reveals, however, that there is not adequate adherence to these recommendations and guidelines. Management of anticoagulation therapy by a nurse practitioner may improve compliance and safety in ambulatory surgery centers. AORN J 95 (April 2012) 510-521. © AORN, Inc, 2012. doi: 10.1016/j.aorn.2012.01.018 Key words: anticoagulation therapy, thromboembolism risk, warfarin, vitamin K antagonist. M illions of patients receive anticoagulants for the prevention of thromboembolic events.1 Maintenance anticoagulation therapy (ACT) is prescribed for a variety of indicates that continuing education contact hours are available for this activity. Earn the contact hours by reading this article, reviewing the purpose/goal and objectives, and completing the online Examination and Learner Evaluation at http://www.aorn.org/CE. The contact hours for this article expire April 30, 2015. medical diagnoses and conditions, including atrial fibrillation, history of myocardial infarction, implantation of mechanical heart valves, indwelling myocardial stents, history of thromboembolism, and prevention of stroke.1,2 Each year, approximately 250,000 people receiving warfarin for long-term ACT will require interruption of this therapy for surgical or other invasive procedures.3 Continuation of ACT during surgical or invasive procedures predisposes patients to increased bleeding risks because of warfarin’s long half-life (ie, two to three days). The overall effect of warfarin can last up to five doi: 10.1016/j.aorn.2012.01.018 510 AORN Journal ● April 2012 Vol 95 No 4 © AORN, Inc, 2012 ANTICOAGULATION MANAGEMENT www.aornjournal.org days.4 In addition, withholding this medication bestandardization and recommended the use of infore a procedure or surgery may result in subtheraternational normalized ratio (INR), which is a 2 peutic levels for up to a week. Interrupting anticoformula calculated to correct for differences in agulation can result thromboplastin rein the formation of agents.4 The dependent control variable thrombosis. This can One goal of anticoagulation management in many research have devastating conduring the phases of perioperative care is studies is the amount sequences, such as appropriate regulation of warfarin. Warfarin has a narrow therapeutic range, and modest of time individuals embolic stroke, changes in dose can lead to either thrombosis spend within therawhich results in mapeutic INR range. jor disability or death or hemorrhage. Warfarin has a narin 70% of patients.5 Health care providers row therapeutic must appropriately assess the patient’s ACT when range, and modest changes in dose can lead to surgical or other invasive procedures, whether either thrombosis or hemorrhage.6 Most surgeries can be performed without risk of serious hemorelective or emergent in nature, are required. The rhage when the INR is less than 1.5.5 challenge is to balance the patient’s risk of expeOne of the goals of anticoagulation manageriencing a thromboembolism, arterial or venous, ment during the phases of perioperative care is when discontinuing a prescribed blood thinner appropriate regulation of warfarin. All individuals, with the risk of bleeding if ACT is maintained. whether they are instructed to continue warfarin at current or reduced dosages or to discontinue PHARMACOLOGY use of warfarin should undergo INR monitoring Warfarin is the predominant maintenance vitaone to two days before the procedure.3 Medicamin K antagonist and the most widely pretions, particularly ACT, need to be resumed in an scribed anticoagulant in North America.4 It acts pharmacologically by inhibiting the enzymes appropriate time frame. responsible for the cyclic interconversion of vitamin K in the liver. This converted or reGUIDELINES FOR ANTITHROMBOTIC duced form of vitamin K serves as a cofactor in THERAPY The American College of Chest Physicians the production of coagulation protein factors II (ACCP) has developed evidence-based practice (ie, prothrombin), VII, IX, and X. Suppressing guidelines for antithrombotic therapy during the the production of clotting factors prevents the perioperative period.3 High-risk patients or painitial formation and propagation of a thromtients undergoing procedures for which there is an bus. Warfarin has no effect on formed thrombi 4 increased risk of bleeding should be treated with or previously circulating clotting factors. Prothrombin time had been used for decades to bridging therapy of subcutaneous or IV heparin or monitor warfarin anticoagulation. Prothrombin subcutaneous low-molecular-weight heparin. The time measures the amount of time required for ACCP recommends that health care providers clot formation when laboratory personnel add calkeep patients on warfarin for minor dental, skin, cium and thromboplastin to citrated blood. Comor eye procedures.3 When bleeding is a concern, the ACCP recommends discontinuing warfarin at mercially prepared thromboplastin reagents proleast five days before an invasive procedure.3,7 duce substantially different results because of Patients not treated with bridging therapy will variability in their sensitivity. The World Health have subtherapeutic ranges in their INR and, Organization recognized the need for monitoring AORN Journal 511 April 2012 Vol 95 therefore, have an increased risk of thromboembolic events. Health care providers should restart the patient’s ACT within 12 to 24 hours after the procedure or as soon as there are no signs of active bleeding.3 Management should be individualized and coordinated among the patient, nonmedical caregiver, primary care provider, surgeon, and anesthesia professional in a timely and comprehensive manner.1 Anticoagulants are among the medications most frequently implicated in adverse drug events, many of which are preventable.8 National hospital accreditation organizations and patient safety groups have emphasized the need for health care providers to develop strategies or guidelines to reduce the risk and improve the safe use of anticoagulants.9-11 During 2008, the US surgeon general issued a nationwide action statement to reduce the number of cases of deep vein thrombosis and pulmonary embolism in the United States and urged health care organizations to incorporate coordinated, multifaceted plans to address the problem.9 The Joint Commission has called for the reduction of harm associated with ACT and recommends that health care providers use approved protocols and management programs to individualize care; evaluate and improve ACT safety practices; and educate personnel, patients, and patients’ family members.10 The Institute for Safe Medication Practices (ISMP) indicates that there may be a misunderstanding by the patient because of previous instructions to discontinue a medication before a surgical or other invasive procedure,11 therefore, the ISMP emphasizes that health care providers should communicate clearly in instructing patients when to discontinue and resume all medications. 512 AORN Journal HILL EISENSTEIN No 4 SIGNIFICANCE FOR AMBULATORY SURGERY CENTERS A majority of surgical or other invasive procedures are being performed at ambulatory surgery centers (ASCs).3 Patients on long-term ACT are at increased risk of adverse outcomes without proper ACT management during the phases of their perioperative care. Even though the ACCP has established clinical guidelines to support clinicians, it acknowledges that there are gaps in the literature, many observational studies are based on small populations, and no standardized bridging anticoagulation protocols are presented.3 The ACCP guidelines recommend that practice patterns be based on patient characteristics and the type of procedure being performed.3 As evidence-based practice changes, it is difficult for individual health care providers to stay abreast of new information. Recognized barriers to clinicians’ compliance with current antithrombotic practice and guidelines include lack of familiarity with ACT guidelines, lack of awareness of the significance of consistent ACT practices, disagreement with ACT guidelines, and resistance to change.12 Knowledge from research demonstrates that warfarin can be safely interrupted in low- to intermediate-risk patients during a short perioperative phase but that prolonged interruption or discontinuation of ACT for perioperative procedures increases the patient’s risk for thromboembolic events.7 Garcia et al7 reported a 0.4% incidence of thromboembolic events when warfarin was interrupted for five or fewer days; however, the incidence of thromboembolic events increased to 2.2% when warfarin interruption extended beyond seven days. Warfarin is 1.5 times more likely to be discontinued after an ambulatory procedure and twice as likely to be discontinued after an overnight hospitalization for elective surgery.13 ANTICOAGULATION MANAGEMENT www.aornjournal.org PATIENT EDUCATION Anticoagulation Therapy (ACT) Overview Anticoagulation medicine helps prevent blood clots from forming and helps prevent postoperative complications caused by clotting, such as heart attack, deep vein thrombosis, or pulmonary embolism. This medicine also may be given if you are at risk for blood clots (eg, being obese, immobile, on bed rest). Some medicines used for ACT include warfarin and heparin. Some medicines may be taken as pills; others must be given as a shot. How do health care providers know if the ACT is working? Depending on your health and the condition being treated, your doctor will order a blood test called the international normalized ratio (INR), which measures how long it takes your blood to clot, to decide the proper medicine and dose. It is very important to return to the hospital, clinic, or outpatient office as instructed by your doctor for repeated laboratory tests. An INR also will be performed before surgery. Your doctor will advise you whether to stop taking your medication before surgery and when to resume taking it after your surgery. How do I take this medicine? You should take the ACT medicine in the evening at the same time every day or as directed by your doctor. Never skip a dose. If you do miss a dose, you should take it as soon as possible but never take two doses at the same time. If you forget to take a dose and don’t remember until the next day, call your doctor’s office for instructions. What do I have to do differently if I am on ACT? This medicine can cause bleeding problems so you should avoid playing potentially dangerous sports; use an electric razor to shave; use a soft toothbrush; use waxed dental floss gently; wear gloves for yard work and when using sharp tools; wear shoes or nonskid slippers in the house; trim nails carefully; and be careful when using knives and scissors. Some foods interfere with ACT, so you must be careful of what you eat. For instance, foods high in vitamin K can change your INR range easily. You should avoid eating large amounts of vitamin K-rich food at a single meal. These include green, leafy, vegetables, such as kale, collard greens, spinach, and turnip greens. Some medicines interfere with ACT, so never begin tak- ing a new medicine without first talking to your doctor. Some of these medicines include antibiotics; pain medicines; nonsteroidal anti-inflammatory drugs, such as ibuprofen; and diabetes medicines that are taken by mouth. Popular herbs, such as ginseng, ginkgo biloba, garlic, chamomile, and ginger, all may influence the INR and increase bleeding time. You may be asked to use a medicine log or journal to help track medicine usage and dosing. Never start or stop taking these medicines without first talking to your doctor. Tell all health care providers, including your dentist and pharmacist, that you are on ACT, so they can plan your care accordingly. Your doctor may tell you to decrease your dose of ACT or stop oral ACT medicine before surgery. He or she may start you on a different medicine, such as heparin or low-molecular-weight heparin. Ask your dentist if you should take your ACT medicine differently before dental procedures like removing a tooth. Some surgery, such as skin surgery or a biopsy of soft tissue, can be done safely without changing your ACT medicine, but it is always best to check with your doctor. Carry or wear medical identification to let health care providers know that you take ACT. Tell your doctor if you have any side effects from the medicine; your doctor may change the dose or substitute another medicine. What are the signs and symptoms of side effects of ACT? Bleeding is the primary adverse effect of taking anticoagulation medicine. The most serious effect is bleeding in the brain; signs of this include uncoordination, dizziness, new headache, nausea, or vomiting. Signs of bleeding in the stomach or intestines include vomitus that looks like coffee grounds; dark, tarry, or red stools; weakness; dizziness; thirst; or abdominal pain. Seek medical care if you experience any of these symptoms and even for simple things like cuts that do not stop bleeding or fail to heal, or unexplained or prolonged bruising. Resource Anticoagulation therapy. The Heart Hospital Baylor. http:// www.thehearthospitalbaylor.com/handler.cfm?event⫽practice, template&se⫽1&cpid⫽20127&ppe⫽Abstract%20%2D% 20Anticoagulant%20Therapy. Accessed October 14, 2011. AORN Journal 513 April 2012 Vol 95 No 4 HILL EISENSTEIN Medication continuity is generally considered to studies provide evidence that ACT management be the responsibility of the patient. However, a services are an effective method of improving change in medication regimen, such as disconcare.14-16 Results of other research support the use of nurse-managed ACT care.17-20 Services tinuation of warfarin five days prior to a proceprovided by a perioperative nurse practitioner dure, may be confusing to patients. In actuality, (NP) would be an appropriate solution for the restarting medications requires participation 13 assessment, management, interruption, and refrom health care providers and the patient. An increased risk of unintended warfarin discontinsumption of ACT in the ambulatory setting. The uation after elective procedures may be a result of NP develops specific pathways from evidencethe health care provider discontinuing the warfarin based guidelines and collaborates with other before surgery but failing to instruct the patient to health professionals. Also, the use of inpatient restart the medication after surgery. With other medcomputer-based clinical decision support systems ications, health care providers instruct patients to has been proven to be advantageous with anticotake their medications the night before or the mornagulation management for surgical procedures.21 ing of the procedure and to continue taking them as normal after surgery.13 IMPLICATIONS FOR HEALTH CARE The ISMP contends that health care providers Health care is interconnected to many other asprescribing initial ACT may transfer the responsipects of life as a natural consequence of the way bility to resume discontinued medication therapy in which the care after an invasive proprovided affects peocedure to patients, ple, communities, nurses, pharmacists, Services provided by a perioperative nurse and society. The aror primary care phypractitioner would be an appropriate solution eas that health care sicians.11 Patients are for the assessment, management, interruption, affects include, but placed at high risk and resumption of anticoagulation therapy in are not limited to, the ambulatory setting. when communication health policy, organiabout medications is zation, and financing; not clear.10,11 This ethics; professional translates to the posdevelopment; human diversity; social issues; sibility of thromboembolism complications occurhealth promotion; and disease prevention. ring at home during the first two weeks after surgery.3 These thromboembolic events can have Health Policy, Organization, and Financing devastating consequences that ultimately could result Although the ACCP has recommended standards in the patient’s death. It is essential, therefore, that for ACT during the phases of perioperative care, health care providers manage ACT appropriately the World Health Organization Collaborating Cenduring the phases of perioperative care. tre for Patient Safety Solutions emphasizes that imAlthough practice guidelines have been estabplementation of standards requires leadership suplished for the use of ACT during surgical and port, with active physician, nursing, and pharmacist other invasive procedures, there is limited reinvolvement.22 It is important for health care providsearch on patient outcomes and health care proers at ASCs to follow health policy and have a stanvider efficacy in the ASC.3 Consistent ACT mandardized system to document agement in ambulatory settings is vital during the prescription and nonprescription medications vulnerable perioperative phase to help prevent before admission, bleeding and thromboembolic events. Several 514 AORN Journal ANTICOAGULATION MANAGEMENT the patient’s instructions for the administration of those medications proceeding the date of the procedure, and an updated list that includes new medications and those previously prescribed to be resumed at the time of discharge. Recommendations include the use of technological support and electronic medical records to facilitate medication reconciliation.22 Preoperative clinic visits improve patient outcomes, specifically in patients older than 60 years, and reduce procedure cancellations and delays, which translates to cost savings.23 Adverse events relating to ACT are costly, as indicated by the average cost of an inpatient recurrent venous thromboembolic event (ie, $14,975).24 Ethical Decision Making Noncompliance with current antithrombotic guidelines is a concern.12 Creating an anticoagulation pathway in an ASC is an ethical decision to strive for improved patient outcomes, prevent adverse events, and eliminate inconsistent and unpredictable patterns of practice associated with anticoagulation.25 Aspects of care addressed by a pathway would include immediate initiation of anticoagulation after surgery, postprocedure administration of ACT earlier in the day, improved ACT management or coordination by an NP rather than by various providers, use of a pathway by practitioners other than NPs for consistency.25 Professional Role Development Nurse practitioners are successfully moving from the primary care setting to the perioperative environment. By using evidence-based guidelines, the NP functions independently or collaboratively with the surgeon and the anesthesia professional. In the perioperative environment, the NP might obtain the patient’s medical and surgical history, perform a physical assessment, www.aornjournal.org perform the nursing and anesthesia assessments, provide patient teaching, order and interpret diagnostic tests, eliminate unnecessary tests, act as a resource person for perioperative personnel and patients before and after surgery, prescribe necessary medications related to ACT, and perform medication reconciliation.26,27 The role of the NP is well-suited to manage these and other responsibilities in the ASC (Table 1). By evaluating and assessing the patient, the NP can identify individuals who need thromboembolism prophylaxis, which is often missed.27 Highrisk patients may need a referral to an inpatient surgical setting rather than having the surgery performed in an ASC. Human Diversity and Social Issues Health care providers need to adjust care to meet the needs of the ever-changing patient population. Annual use of warfarin for preventative measures has increased 20% because of the expanding population of older adults.19 Health care providers should direct special attention toward the heterogeneity of culture, language, health beliefs, and risk for disease among US geriatric patients, many of whom have been prescribed ACT and require outpatient procedures.28 Approximately one-third of all Americans will be classified as a minority or an older adult in the near future.29 Previous research suggests that African Americans and Spanishspeaking Hispanics achieve a therapeutic range of INR less often than adults in other populations.30 Low literacy levels present yet another barrier to health promotion. Written patient materials are meant to provide information and promote health. Research conducted to assess readability and to assess the cultural sensitivity of written anticoagulation educational material in an African American population found that, as age increased, reading skills decreased and the mean reading level was three to four grades below the reported AORN Journal 515 April 2012 Vol 95 HILL EISENSTEIN No 4 TABLE 1. Nursing Care Plan for a Perioperative Patient on Anticoagulation Therapy Diagnosis Risk for injury Nursing interventions Ineffective family therapeutic regimen management 516 AORN Journal Interim outcome statement Confirms patient identity. Verifies allergies. Verifies operative procedure, surgical site, and laterality. Establishes IV access. Reviews medication reconciliation sheet for current medications, medication allergy interactions, contraindications, medication-medication or herbalmedication interactions. Verifies medication label. Performs patient identification by using at least two identifiers. Ensures the seven rights of medication administration are followed: right patient, right medication, right dose, right route, right time, right reason, and right documentation. Administers correct dose by validating order as prescribed; obtaining accurate patient weight before surgery by using a facility-approved conversion chart to convert pounds to kilograms; and calculating weight-based dose accurately and verifying the calculation with two licensed individuals. Assesses the patient’s preoperative hydration status as appropriate (eg, weight, height, skin turgor, pulses, hematocrit, blood urea nitrogen, albumin, serum electrolytes, total protein, serum osmolality, specific gravity levels). Prioritizes nursing actions, such as correcting hypovolemia, hypervolemia, and blood glucose levels. Provides equipment and supplies based on patient’s needs. Evaluates response to medications. Assesses psychosocial issues specific to the patient’s medication management. Identifies barriers to communication. Determines knowledge level. Includes patient or designated support persons in perioperative teaching. Provides instruction about prescribed medications. Verifies patient’s and designated support person’s ability to understand information. Provides necessary time to process information. Outcome statement The patient receives correct medication(s) in accurate doses, at the correct time, and via the correct route throughout the surgical experience. Medication reconciliation records are completed. The patient receives appropriately administered medication(s). The patient or designated support person can state the correct dose, frequency of administration, and purpose of each prescribed medication at time of discharge. The patient or designated support person demonstrates knowledge of medication management. ANTICOAGULATION MANAGEMENT www.aornjournal.org TABLE 1. (continued) Diagnosis Interim outcome statement Nursing interventions Obtains an interpreter if needed. Provides alternatives to interpreter when appropriate (written material, video, tape recording in primary language). Provides patient and designated support person with written discharge and at-home instructions. Reinforces information provided by other members of the health care team. Observes and evaluates return demonstrations of perioperative instruction. Clarifies information. Encourages patient and designated support person to describe in their own words their understanding of instructions. Encourages patient and designated support person to communicate feelings regarding surgery and expected outcomes. Provides patient and designated support person time to ask questions. Communicates discharge instructions verbally and in writing. Encourages designated support person’s participation in the instructional process. Evaluates patient’s and designated support person’s responses to perioperative instruction. Evaluates response to instruction about prescribed medications. educational reading level.31 Additionally, when developing ACT management services, health care providers should take into account the Culturally and Linguistically Appropriate Services standards developed by the US Health and Human Services Office of Minority Health.32 Health Promotion and Disease Prevention One of the goals established by The Joint Commission is to reduce patient harm associated with the use of anticoagulation medications.10 Implementation of case management and evidencebased guidelines pertaining to anticoagulation regulation during the phases of perioperative care will promote health and reduce the risk of adverse drug events.6 Focused perioperative management Outcome statement The patient or designated support person describes medication adverse effects to report at time of discharge. by NPs with the use of current established guidelines and practices will provide the opportunity to educate and reinforce patient knowledge on medication dosage, food and medication interactions, preadmission and discharge instructions, risks of thromboembolism, and bleeding complications. Furthermore, establishing a rapport with patients improves education and compliance.6 THEORETICAL FOUNDATIONS FOR NURSING PRACTICE Jean Watson’s theory of transpersonal caring, which focuses on the moment-to-moment encounters of the person who is providing care and the person who is being cared for, is an ideal theory to apply to the management of ACT in an AORN Journal 517 April 2012 Vol 95 HILL EISENSTEIN No 4 I. Initial Data _____ 1.What is the patient’s name and hospital record number: ___________________________________ _____ 2.In what age range (in years) does the patient’s age fit? A = 18 – 30 B = 31 – 40 C = 41 – 50 D = 51 – 60 E = 61 – 70 F = 70+ _____ 3.What is the patient’s gender? A = Male B = Female _____ 4.What is the patient’s race? A = Asian B = Black C = Hispanic D = White E = Other _____ 5.What is the patient’s highest level of education? A = High school diploma B = 1 to 4 years post high school education C = 5+ years post high school education D = Other: _______________________________________________________________________ _____ 6.What is the patient’s preoperative diagnosis? A = History of atrial fibrillation B = History of deep vein thrombosis C = Presence of a mechanical heart valve D = Presence of myocardial stent E = Other: _______________________________________________________________________ _____ 7.What is the planned invasive procedure to be performed? _________________________________ _____ 8.What is the date of the proposed invasive procedure? _____________________________________ _____ 9.What is the patient’s current warfarin dose? ____________________________________________ ____10. What is the patient’s desired international ratio (INR) target range? A = 1.5 to 2.5 B = 2.6 to 3.5 C = Other _______________ ____11. Who was the initial ACT prescriber? A = Advanced practice nurse B = Anesthesia professional C = Primary care provider D = Surgeon E = Other ____12. Who was the prescriber at the time of the surgical procedure? A = Advanced practice nurse B = Anesthesia professional C = Primary care provider D = Surgeon E = Other ____13. What comorbidities did the patient present with? ________________________________________ II. 24 Hour Interview Date of Interview__/__/____ A. Adverse events ____14. Did the patient experience a thromboembolism? A = No B = Yes Time__/__/____ ____15. Did the patient have any bleeding problems? A = No B = Yes ____16. Did the patient experience any other problems? A = No B = Yes Specify _________________________________________________________________________ ____17. Was the patient’s ACT restarted within 24 hours of procedure? A = No B = Yes ____18. If no, did the interviewer instruct the patient to contact his or her primary care provider for ACT management? A = No B = Yes Figure 1. Ambulatory Surgical/Invasive Procedure Anticoagulation Therapy Data Collection Form. 518 AORN Journal ANTICOAGULATION MANAGEMENT www.aornjournal.org B. Patient instructions ____18. Did the patient received instructions to restart ACT after the invasive procedure? A = No B = Yes ____19. If yes, what time was the patient instructed to resume ACT? A = In the evening on the day of the procedure B = In the morning after the procedure C = In the evening on the day after procedure D = Other ____20. If yes, what time did the patient actually restart his or her ACT? A = In the evening on the day of the procedure B = In the morning after the procedure C = In the evening on the day after procedure D = Other ____21. Who gave the patient instructions to restart ACT? A = Advanced practice nurse B = Anesthesia professional C = Primary care provider/prescriber D = Surgeon E = Other III. Week 2 Interview Date of Interview__/__/____ A. Adverse events ____22. Did the patient experience a thromboembolism? A = No B = Yes Time__/__/____ ____23. Did the patient have any bleeding problems? A = No B = Yes ____24. Did the patient experience any other problems? A = No B = Yes Specify _________________________________________________________________________ ____25. Did the patient contact the ACT prescriber after the invasive procedure for any reason pertaining to ACT? A = No B = Yes ____26. Is the patient currently taking ACT A = No B = Yes ____27. If no, why not? ___________________________________________________________________ ____28. Was an INR obtained since the last interview? A = No B = Yes IV. Week 4 Interview Date of Interview__/__/____ A. Adverse events ____29. Did the patient experience a thromboembolism? A = No B = Yes Time__/__/____ ____30. Did the patient have any bleeding problems? A = No B = Yes ____31. Did the patient experience any other problems? A = No B = Yes Specify _________________________________________________________________________ ____32. Did the patient contact the ACT prescriber contacted after invasive procedure for any reason pertaining to ACT? A = No B = Yes ____33. If yes, why? ___________________________________________________________________ ____34. Is the patient currently taking ACT? A = No B = Yes ____35. If no, why not? _________________________________________________________________ ____36. Was an INR obtained since the last interview? A = No B = Yes Figure 1. Continued AORN Journal 519 April 2012 Vol 95 ambulatory setting.33,34 This theory expounds on the act of caring with the concept of intentional caring that produces a positive energy, resulting in health and healing in the present and future. Caring through the acts of listening, expressing emotion, educating, and performing procedures and treatments is a component of an ethically aware practice that produces positive outcomes. A consciousness of this theory has safety and economic advantages as well as system success. This theory is explicitly suited for perioperative ACT management by NPs because outpatient surgeries and procedures predispose individuals and their family members to increased levels of stress. The NP provides management, treatment, counseling, and education in a sensitive and caring manner to promote health and prevent illness. FUTURE RESEARCH Research is needed to assess methods of interrupting and reestablishing use of anticoagulants in an ASC to evaluate outcomes and adverse effects and to determine compliance with existing ACT guidelines. Anticoagulation services other than primary care providers have shown statistically significant improvements in patient outcomes.14-18 The role of the NP is expanding from primary care to specialty areas. Research supports using NPs to manage ACT and other services during the phases of perioperative care. Therefore, it is recommended that research be initiated to evaluate outcomes associated with NP-led ACT management in an ASC. A research tool that could be used to collect data is shown in Figure 1. Health care personnel would collect initial data beginning 24 hours before the patient’s surgery or procedure. The personnel would then collect ongoing data in person or with the use of telephone interviews about outcomes pertaining to adverse events, quality of care issues, compliance with guidelines, comparison of providers, and differences in population groups at two weeks and four weeks after surgery. A quantitative, prospective, 520 AORN Journal HILL EISENSTEIN No 4 cohort study would help clarify the effects of ACT management provided by NPs. CONCLUSION National safety goals have drawn attention to anticoagulation standards and the needs associated with them. Current research suggests that long-term ACT does not need to be interrupted during minor procedures for dentistry, dermatology, and ophthalmology. Analysis of evidence also suggests that interrupting long-term ACT for minor surgery or other invasive procedures is a recommended and acceptable practice when there is a significant risk of bleeding. Prolonged discontinuation of ACT, however, may predispose individuals to unnecessary risks of thromboembolism. Potential advantages of anticoagulation management in the ASC by an NP include improved communication among health care providers and patients, increased awareness of the need for ACT education, improved health care provider and patient compliance with perioperative ACT guidelines, an enhanced patient perioperative experience, and overall cost savings related to adverse events and complications. Perioperative ACT management by NPs appears to be a practical and beneficial next step in reducing risks and complications of ACT when patients are undergoing surgery. References 1. 2. 3. 4. Garcia DA, Witt DM, Hylek E, et al. Delivery of optimized anticoagulant therapy: consensus statement from the Anticoagulation Forum. Ann Pharmacother. 2008; 42(7):979-988. Gaines KK. Management of anticoagulation therapy for invasive procedures. Urol Nurs. 2005;25(5):379-380. Douketis JD, Berger PB, Dunn AS, et al. The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133(6 suppl):299S-339S. Dipro JT, Talbert RL, Yee GC, Matzke GR, Wills BG, Posey LM. Venous thromboembolism. In: Weitz M, ANTICOAGULATION MANAGEMENT 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. Davis K, eds. Pharmacotherapy: A Pathophysiologic Approach. New York, NY: McGraw-Hill Companies, Inc; 2008:347-352. Kaplan BC, Trischwell DL, Longstreth WT Jr, et al. Vascular events, mortality, and preventive therapy following ischemic stroke in the elderly. Neurology. 2005;65(6):835-842. Venkatachalam V, D’Atillio K, Lewis A, Acevedo M. Anticoagulation in ambulatory care: an evidence-based review of the literature. Prof Case Manag. 2007;12(2):106-111. Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med. 2008;168(1):63-69. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289(9):1107-1116. The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. 2008. US Department of Health and Human Services. http://www .surgeongeneral.gov/new/pressreleases/pr20080915 .html. Accessed October 24, 2011. Ambulatory Health Care. 2011 National Patient Safety Goals. The Joint Commission. http://www.jointcommission .org/ahc_2011_npsgs. Accessed October 24, 2011. Orders to “continue previous meds” continue a long standing problem. The Institute for Safe Medication Practices. November 1, 2000. http://www.ismp.org/ Newsletters/acutecare/articles/20001101.asp. Accessed October 24, 2011. Caprini JA, Hyers TM. Compliance with antithrombotic guidelines. Manag Care. 2006;15(9):49-66. Bell CM, Bajcar J, Bierman AS, Li P, Mamdani MM, Urbach DR. Potentially unintended discontinuation of long-term medication use after elective surgical procedures. Arch Intern Med. 2006;166(22):2525-2531. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care: anticoagulation control, patient outcomes, health care costs. Arch Intern Med. 1998;158(15):1641-1647. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515-1522. Biscup-Horn PJ, Streiff MB, Ulbrich TR, Nesbit TW, Shermock KM. Impact of an inpatient anticoagulation management service on clinical outcomes. Ann Pharmocother. 2008;42(6):777-782. Shimabukuro TT, Kramer J, McGuire M. Development and implementation of nurse-managed anticoagulation program. J Healthc Qual. 2004;26(1):4-12. Connor CA, Wright CC, Fegan CD. The safety and effectiveness of a nurse-led anticoagulant service. J Adv Nurs. 2002;38(4):407-415. Hennessy BJ, Vyas M, Duncan B, Allard SA. Evaluation of an alternative model of anticoagulant care. Ir J Med Sci. 2000;169(1):34-36. Taylor FC, Gray A, Cohen H, Gaminara L, Ransay M, Miller D. Costs and effectiveness of a nurse specialist anticoagulant service. J Clin Pathol. 1997;50(10):823-828. Durieux P, Nizard R, Ravaud P, Mounier N, Lepage E. A clinical decision support system for prevention of venous thromboembolism: effect on physician behavior. JAMA. 2000;283(21):2816-2821. www.aornjournal.org 22. WHO Collaborating Center for Patient Safety Solutions. Assuring medication accuracy at transitions of care. Patient Safety Solutions. 2007;1(6). http://www .ccforpatientsafety.org/common/pdfs/fpdf/presskit/ PS-Solution6.pdf. Accessed October 24, 2011. 23. Ferschi MB, Tung A, Sweitzer B, Huo D, Glick DB. Preoperative clinic visits reduce operating room cancellations and delays. Anesthesiology. 2005;103(4):855-859. 24. Bullano M, Willey V, Hauch O, Wygant G, Spyropoulos AC, Hoffman L. Longitudinal evaluation of health plan cost per venous thromboembolism or bleed event in patients with a prior venous thromboembolism event during hospitalization. J Manag Care Pharm. 2005; 11(8):663-673. 25. Delmora BA, Hansen D, Money KA, Paplanus LM, Sutton PR. An anticoagulation pathway for quality management. Appl Nurs Res. 2000;13(2):105-110. 26. Barnett JS. An emerging role for nurse practitioners— preoperative assessment. AORN J. 2005;82(5):825-834. 27. Kidik PJ, Holbrook KF. The nurse practitioner role in evidence-based medication strategies. J Perianesth Nurs. 2008;23(2):87-93. 28. Yeo G. How will the US healthcare system meet the challenge of the ethnogeriatric imperative? J Am Geriatr Soc. 2009;57(7):1278-1285. 29. 2008 Older Americans: key indicators of well-being. AgingStats.gov. Federal Interagency Forum on Aging Related Statistics. http://www.agingstats.gov/agingstatsdotnet/ Main_Site/Data/Data_2008.aspx. Accessed October 24, 2011. 30. Bhandari VK, Wang F, Bindman AB, Schillinger D. Quality of anticoagulation control: do race and language matter? J Health Care Poor Underserved. 2008; 19(1):41-55. 31. Wilson F, Racine E, Tekieli V, Williams B. Literacy, readability and cultural barriers: critical factors to consider when educating older African Americans about anticoagulation therapy. J Clin Nurs. 2003;12:275-282. 32. National Standards on Culturally and Linguistically Appropriate Services (CLAS). US Department of Health & Human Services, The Office of Minority Health. http://minorityhealth.hhs.gov/templates/browse.aspx? lvl⫽2&lvlid⫽15. Accessed October 24, 2011. 33. Watson J. Intentionality and caring-healing consciousness: a practice of transpersonal nursing. Holist Nurs Pract. 2002;16(4):12-19. 34. Watson J. Caring theory as an ethical guide to administrative and clinical practices. JONAS Healthc Law Ethics Regul. 2006;8(3):87-93. Diana Hill Eisenstein, MSN, RN, FNP-BC, CNOR, is a nurse practitioner at Cooper University Hospital, Camden, NJ, and a perioperative staff nurse at Virtua-West Jersey Health System, Berlin, NJ. Ms Eisenstein has no declared affiliation that could be perceived as posing a potential conflict of interest in the publication of this article. AORN Journal 521 EXAMINATION CONTINUING EDUCATION PROGRAM 2.7 Anticoagulation Management in the Ambulatory Surgical Setting www.aorn.org/CE PURPOSE/GOAL To educate perioperative nurses about managing anticoagulation therapy (ACT) during the ambulatory perioperative period. OBJECTIVES 1. 2. 3. 4. Identify conditions for which ACT is appropriate. Discuss the perioperative management of ACT. Identify barriers to clinicians’ compliance with ACT. Discuss advantages of appropriate management of ACT. The Examination and Learner Evaluation are printed here for your convenience. To receive continuing education credit, you must complete the Examination and Learner Evaluation online at http://www.aorn.org/CE. QUESTIONS 1. Maintenance ACT may be prescribed for 1. atrial fibrillation. 2. history of myocardial infarction. 3. implantation of mechanical heart valves. 4. indwelling myocardial stents. 5. history of thromboembolism. 6. prevention of stroke. a. 1, 3, and 5 b. 2, 4, and 6 c. 2, 3, 5, and 6 d. 1, 2, 3, 4, 5, and 6 2. When a patient on ACT requires a surgical or other invasive procedure, the challenge is to balance the patient’s risk of having a thromboembolism when discontinuing a prescribed blood thinner with the risk of bleeding if ACT is maintained. a. true b. false 522 AORN Journal ● April 2012 Vol 95 No 4 3. The predominant maintenance vitamin K antagonist used for the prevention of thrombosis in North America is a. streptokinase. b. warfarin. c. enoxaparin. d. heparin. 4. Most surgeries can be performed without risk of serious hemorrhage when the international normalized ratio is a. less than 1.5. b. 1.5 to 1.9. c. 2.0 to 2.4. d. greater than 2.5. 5. High-risk patients or patients undergoing procedures for which there is an increased risk of bleeding should be 1. treated with bridging therapy of subcutaneous or IV heparin. 2. continued on warfarin but in lower doses. © AORN, Inc, 2012 CE EXAMINATION 3. transitioned to streptokinase. 4. treated with bridging therapy of subcutaneous low-molecular-weight heparin. a. 2 b. 3 c. 1 and 4 d. 2 and 3 6. Health care providers should restart the patient’s ACT 1. as soon as the patient is discharged. 2. as soon as there are no signs of active bleeding. 3. within 24 to 48 hours after the procedure. 4. within 12 to 24 hours after the procedure. a. 1 and 3 b. 2 and 4 c. 1, 2, and 3 d. 1, 2, and 4 7. Recognized barriers to clinicians’ compliance with current antithrombotic practice and guidelines include 1. confusion because of contradictory ACT guidelines published by regulatory agencies. 2. disagreement with established ACT guidelines. 3. lack of awareness of the significance of consistent ACT practices. 4. lack of familiarity with ACT guidelines. 5. resistance to change. a. 1 and 3 b. 2, 4, and 5 c. 2, 3, 4, and 5 d. 1, 2, 3, 4, and 5 8. Methods for providing consistent ACT management in ambulatory settings include 1. ACT management services. www.aornjournal.org 2. nurse-managed ACT care. 3. services provided by a perioperative nurse practitioner. 4. use of inpatient computer-based clinical decision support systems. a. 1 and 3 b. 2 and 4 c. 1, 2, and 4 d. 1, 2, 3, and 4 9. When using evidence-based guidelines and practices, the nurse practitioner caring for the patient on ACT in the perioperative setting might 1. obtain the patient’s medical and surgical history. 2. perform a physical assessment. 3. schedule procedures and ACT management by using a strictly cost-effective approach. 4. provide patient teaching. 5. order and interpret diagnostic tests. 6. prescribe necessary medications. a. 1, 3, and 5 b. 2, 4, and 6 c. 1, 2, 4, 5, and 6 d. 1, 2, 3, 4, 5, and 6 10. Potential advantages of appropriate management of ACT during the perioperative phase are 1. improved communication among health care providers and patients. 2. improved health care provider and patient compliance with perioperative ACT guidelines. 3. an enhanced patient perioperative experience. 4. overall cost savings related to adverse events and complications. a. 2 and 3 b. 1 and 4 c. 1, 2, and 4 d. 1, 2, 3, and 4 The behavioral objectives and examination for this program were prepared by Rebecca Holm, MSN, RN, CNOR, clinical editor, with consultation from Susan Bakewell, MS, RN-BC, director, Perioperative Education. Ms Holm and Ms Bakewell have no declared affiliations that could be perceived as posing potential conflicts of interest in the publication of this article. AORN Journal 523 LEARNER EVALUATION CONTINUING EDUCATION PROGRAM 2.7 Anticoagulation Management in the Ambulatory Surgical Setting T his evaluation is used to determine the extent to which this continuing education program met your learning needs. Rate the items as described below. OBJECTIVES To what extent were the following objectives of this continuing education program achieved? 1. Identify conditions for which anticoagulation therapy (ACT) is appropriate. Low 1. 2. 3. 4. 5. High 2. Discuss the perioperative management of ACT. Low 1. 2. 3. 4. 5. High 3. Identify barriers to clinicians’ compliance with ACT. Low 1. 2. 3. 4. 5. High 4. Discuss advantages of appropriate management of ACT. Low 1. 2. 3. 4. 5. High CONTENT 5. To what extent did this article increase your knowledge of the subject matter? Low 1. 2. 3. 4. 5. High 6. To what extent were your individual objectives met? Low 1. 2. 3. 4. 5. High 7. Will you be able to use the information from this article in your work setting? 1. Yes 2. No 8. Will you change your practice as a result of reading this article? (If yes, answer question #8A. If no, answer question #8B.) www.aorn.org/CE 8A. How will you change your practice? (Select all that apply) 1. I will provide education to my team regarding why change is needed. 2. I will work with management to change/ implement a policy and procedure. 3. I will plan an informational meeting with physicians to seek their input and acceptance of the need for change. 4. I will implement change and evaluate the effect of the change at regular intervals until the change is incorporated as best practice. 5. Other: ____________________________ 8B. If you will not change your practice as a result of reading this article, why? (Select all that apply) 1. The content of the article is not relevant to my practice. 2. I do not have enough time to teach others about the purpose of the needed change. 3. I do not have management support to make a change. 4. Other: __________________________ 9. Our accrediting body requires that we verify the time you needed to complete the 2.7 continuing education contact hour (162-minute) program: _________________________________ This program meets criteria for CNOR and CRNFA recertification, as well as other continuing education requirements. AORN is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AORN recognizes these activities as continuing education for registered nurses. This recognition does not imply that AORN or the American Nurses Credentialing Center approves or endorses products mentioned in the activity. AORN is provider-approved by the California Board of Registered Nursing, Provider Number CEP 13019. Check with your state board of nursing for acceptance of this activity for relicensure. Event: #12512; Session: #0001; Fee: Members $13.50, Nonmembers $27 The deadline for this program is April 30, 2015. A score of 70% correct on the examination is required for credit. Participants receive feedback on incorrect answers. Each applicant who successfully completes this program can immediately print a certificate of completion. 524 AORN Journal ● April 2012 Vol 95 No 4 © AORN, Inc, 2012