Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
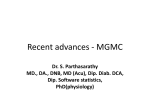
Alexandria Journal of Anaesthesia and Intensive Care 34 Propofol versus Remifentanil Patient Controlled Sedation for Awake Craniotomy During Epileptic Surgeries Ashraf A Moussa, MD*, Saad A Sheta, MD**, Essam A Eid, MD* Department of Anaesthesia, * National Liver Institute, Menofiya University, Egypt; **Faculty of Medicine, Alexandria University, Egypt. ABSTRACT Background: Anaesthesia for neurosurgical procedures, specifically craniotomies requiring patient participation presents a challenge to both the neuroanaesthesiologist and the neurosurgeon. Despite the popularity of general anaesthesia for these procedures, there has been a renewed interest in this technique of awake craniotomy due to its definite advantages in specific patient populations. This study evaluate two anaesthetic regimens for propofol and remifentanil for awake craniotomy in epileptic surgeries. Methods:Total drug administered, incidence of complications, sedation score and patient satisfaction were assessed in 20 patients, randomely assigned into 2 equal groups, aged 1855 years undergoing awake craniotomy for epileptic surgeries. Sedation was induced via propofol patient controlled sedation in group I and via remifentanil patient controlled sedation in group II, Results : five patients in the remifentanil group versus two patients in propofol group experienced nausea and /or vomiting. Respiratory rate depression, desturation were more frequent in remifentanil group while pain and hypotension were more frequent in propofol group. Both groups achieved a good level of sedation and patient satisfaction. Conclusion : Propofol and remifentanil are almost ideal drugs for conscious sedation during awake craniotomy. Key wards: Awake craniotomy; epilepsy; propofol; remifentanil. INTRODUCTION Victor Horsley in 1886 performed the first surgical resection for epilepsy (1), since then, the role of the neuroanaesthesiologist has been redefined from one merely administering a general anaesthesia that does not trigger seizures, to providing monitored anaesthesia care for “ awake craniotomy”(2). Anaesthesia is usually provided using a combination of local anaesthesia (local infiltration and regional blockade) and intravenous medications to provide sedation, anxiolysis, and supplemental analgesia during these long procedures(3). Traditionally, neurolept analgesia using a combination of opioid (often fentanyl) and droperidol has been popular technique (4). Regional blockade of the scalp is achieved by blocking four pairs of nerves. The supraorbital and supratrochlear nerves which are the terminal branches of the ophthalmic division of the trigeminal nerve. The auriculo- AJAIC-Vol. (8) No. 2 June 2005 temporal nerve, which is the terminal branch of the mandibular division of the trigeminal nerve, the greater and lesser occipital nerves which are branches from the cervical plexus. Plus blockade of the terminal portions of the temporal branches of the maxillary division of the trigeminal nerve (3) . Recently, the use of propofol sedation during these procedures has been reported (5). However, several reports suggest that propofol has a potent anticonvulsant effect and may depress epileptic activity (6,7). Fortunately, because of its short duration of action, propofol administration could be suspended in advance of neurophysiological monitoring to minimize drug-induced adverse effects. Remifentanil is a novel ultra short acting estrase metabolized synthetic opioid. It is highly selective μ opioid agonist and has an ester linkage rendering it susceptable to rapid meta- Alexandria Journal of Anaesthesia and Intensive Care bolism by non-specific blood and tissue estrases.Adult pharmacokinetic studies have shown a rapid onset of peak effect (blood-brain equilibration time :1.2 – 1.4 min), a short duration of action independent of the duration of infusion (context-insensitive, half-time :3 min) and rapid clearance (40 ml/kg/min). From the time the infusion switch off, the duration of action of the usual plasma concentration is 3-6 minutes with no residual effects. These pharmacokinetic values make it ideal sedo-analgesia for awake craniotomy (8) . The purpose of this study is to compare propofol versus remifentanil in patient controlled sedation technique during the long procedures of awake craniotomy for epeliptic surgeries. PATIENTS After institutional ethics approval from King Faisal Specialist Hospital & Research Centre (KFSH&RC) and acquisition of written, informed consent, 20 adult patients aged 18-55 years, presented for awake craniotomy for intractable epilepsy. Each patient was randomly assigned into one of two equal groups using a computer – generated list (MS Excel 7.0 ), to receive propofol or remifentanil. Group P received propofol as a patient controlled sedation (PCS), and group R received remifentanil as PCS . Exclusion criteria included 100% above ideal body weight, patients who are suffering from any significant arrhythmia, uncontrolled hypertension, severe CNS, lung, liver, renal or endocrine diseases. The chronic use of of anxiolytic, antidepressants or analgesic drugs, or any such use of within 12 h of surgery, was also considered as an exclusion criterion. All patients were receiving anticonvulsant therapy, but the dose was tapered or the drug was discontinued before surgery.Ondansteron 4mg was AJAIC-Vol. (8) No. 2 June 2005 35 given prophylactically i.v on call to OR, the patients were unpremeditated. Regional blockade of the scalp was performed by the surgeon in the holding bay area, 30-60 minutes before the patient arrived in the operating room using bupivacaine 0.5% with epinephrine. Supplemental local anaesthetic solution (bupivacaine 0.25% with epinephrine) was used to infiltrate along the incision lines prior to surgery. During craniotomy, dura mater was anaesthetized using a mixture of lidocaine 1% and 0.25% bupivacaine without epinephrine (9) . On arrival, the patient was placed as comfortable as possible on the operating table. The monitors used included an ECG (lead II), non-invasive automated blood pressure and a pulse oximeter. Supplemental oxygen was given using nasal prongs that were adapted for the monitoring of end tidal CO2 and respiratory rate (Marquette Electronics, Solar 8000, UK). Maintenance intravenous fluid consisted of Ringers lactate at 70 ml/hr through minimum 18-gauge cannula, plus the deficits, and a 20-gauge i.v. cannula was also inserted for the study drug PCA device. Preoperatively, all patient were shown how to use the standard patient controlled analgesia device (Baxter PCA II, Deerfield, USA). and were instructed to administer sedation if they wished to be more “sleepy” or if they experienced anxiety or discomfort.Patients were encouraged to use the PCS device early in the operative procedure( to ensure that they understood how to use it and what effect it would have on them) and were reminded that they could use the pump if they requested more sedation or became restless during the operation. They were also told that supplemental sedation was available from their anaesthesiologist if they were uncomfortable and that the anaesthesiologist would take over administration of sedation if they were unable Alexandria Journal of Anaesthesia and Intensive Care or unwilling to do so at any point in the operation. Sedation for group P consisted of an initial bolus dose of propofol 0.5 mg/kg, a lockout interval of 3 minutes, and patient controlled boluses of 0.25 mg/kg (one half of the initial bolus dose) via a standard PCA device. A basal infusion of 3mg/kg/hr (50 µg/kg/min), was adjusted via a standard syringe pump (Diprifusor TM, Grasepy 3500, by SIMS, Waterford, Herts, UK). Sedation for group R consisted of remifentanil hydrochloride using an initial bolus dose of 0.5 μg/kg over 30 60 seconds, patient contolled boluses of 0.25 μg/kg, a lockout time of 2 min using the standard PCA device. Basal infusion of 0.1 μg/kg/min was used via the standard syringe pump. Remifentanil dosage had been determined by an early open label dose – ranging study(10) To avoid potential interference with the neurophysiological monitoring in group P, propofol administration was suspended 15 minutes prior to neurophysiological recording. ll complications such as nausea, vomiting, seizures, excessive sedation, pain, oxygen desaturation less than 90%, increase end tidal C02 (≥ 45mmHg), decrease respiratory rate (< 8/min.), inability to cooperate, induction of general anaesthesia, airway obstruction, hypotension and hypertension (± 20% from the basal readings) were documented. At anytime during the procedure, if a patient developed seizures, they were treated by a small intravenous dose of thiopentone (25-50mg), and if developed nausea and/or vomiting, they were treated by ondansteron 4mg iv. Intraoperative sedation was assessed prior to surgery (baseline) and then hourly by the attending anaesthesiologist based on a 5-point scale (Appendix I). The technical difficulty associated with each surgical procedure was evaluated by the surgeon based on a 5-point scale(technically easy = 1, AJAIC-Vol. (8) No. 2 June 2005 36 technically difficult = 5). Patient satisfaction was evaluated using a short questionnaire completed by each patient in the recovery room and on the postoperative days 1 and 3 (Appendix II). The total doses of all drugs required and the incidence of complications were tabulated for each patient. Statistical analysis was performed using analysis of variance. Where significance was found, Student t-test was performed. P > 0.05 was considered significant. Fisher’s or Chi-square test was used for the analysis of complications. Calculations were performed on a personal computer, using a standard software package (Winstat TM 3.0, Kalmia, US) RESULTS There were no difference among the two groups in age, sex, weight and length of surgery (table 1). The majority of patients underwent temporal lobectomy. The duration of anaesthesia and surgery averaged 4-5 hours and surgical difficulty was comparable between the both groups. The total requirements of drugs by each group of patients are shown in table 2. In the propofol group, the mean total propofol dose for the initial bolus doses and the basal infusion was 15.8±2mg/kg. All patients in group P required additional PCS boluses of propofol with a mean value of 4.2 ± 4 mg/kg. In the remifentanil group, the mean total remifentanil dose including the initial and basal infusion doses was 28.65 ± 4 µg /kg .All patients in group R required additional PCS boluses of remifentanil with a mean value of 1.9 ±2 µg/kg. The incidence of complications is shown in table 3. Five patients in remifentanil group (50%) experienced nausea and / or vomitting during the surgery, all of them received at least one dose of ondansteron 4 mg iv, this Alexandria Journal of Anaesthesia and Intensive Care was statistically significantly higher than propofol group where two patients only (20 %) had nausea and / or vomitting. p‹ 0.05. One patient in group R had a neurological deficit immediately post operatively in the form of dysphasia that was improving by the time of discharge from hospital. During the first 15 min after initiation of study drug administration and prior to scalp incision, a reduction in systolic blood pressure was observed in patients receiving propofol (from 134 ± 11 to 121 ± 21 mmHg) and a reduction in the respiratory rate per minute in patient receiving remifentanil (from 14 ± 4 to 10 ± 8) and both reductions were statistically significant from the other group, with stable values (P < 0.001, analysis of covariance). No statistically significant difference were observed between propofol and remifentanil groups in the incidence of hypotension (10% in both groups ), or bradycardia (20% and 10 % respectively) throughout the procedure. Compared with baseline, sedation scores increased in a similar fashion in both groups with higher score values for propofopl group during the whole period of surgery when compared to the sedation score values in the remifentanil group but these values did not reach the levels of statistical significance (Figure 1). Patient satisfaction was similar in the two groups with respect to the general level of comfort and willingness to repeat the procedure using the same sedation technique (Table 4). Satisfaction with the option of self administered sedation was high and maintained through out the third postoperative day. DISCUSSION Awake craniotomy requires: (1) sufficient depth of anaesthesia during opening and closing the bone flap; (2) full consciousness during cortical mapping; (3) smooth transition between anaesthesia and consciousness; (4) adequate ventilation; and (5) patients immobility and comfort throughout surgery. In attempt to satisfy these requirements,some techniques have been established. These are summarized as sedation and local anaesthesia(11) and asleep-awake-asleep technique(12) . The combination of various drugs have been tried for conscious sedation. In 1950s, codeine was the favoured drug. The “lytic cocktail” (13) consisting of a combination of pethedine, promethazine and chlorpromazine was used by many anaesthesiologist as multipurpose sedative agent. The concept of neuroleptanalgesia was started in 1959 using a combination of droperidol and fentanyl (14). Table 1: Demographic Data ; Surgical charactristics Characteristic Group P Age (yr) 32 ± 11 Sex (M/F) 4: 6 Weight (kg) 71 ± 10 Length of surgery (Hr) 4.4 ± 1.0 Surgical Site T/F 8/2 Surgical difficulty (1-5) 3 ± 0.9 Local anaesthetic scalp block (Bupivacaine 0.5% 20 ± 1 with epinephrine 1/200.000) (ml) Local anaesthetic scalp infiltration (Bupivacaine 35 ± 18 0.25% with epinephrine 1/200.000) (ml) Data are presented as mean ± SD or number of patients. T/F = Temporal / Frontal. AJAIC-Vol. (8) No. 2 June 2005 37 Group R 30 ± 17 5: 5 77 ± 12 4.5 ± 1.4 8/2 3 ± 0.7 20 ± 1 41 ± 11 Alexandria Journal of Anaesthesia and Intensive Care 38 Table 2: Drug Administered in the two groups of patients. Characteristic Group P Total dose of propofol (mg/kg) 15.8 ± 2 (Initial + basal infusion ) mg/kg Total dose of PCS propofol (mg/kg) 4.2 ± 4 mg/kg 21±2 PCS Demand ratio (%) (success : total demand) 22±20 Total Dose ondansteron (mg) Number of patients given intraoperative 3 Ondansteron Group R 28.65 ± 4 mg/kg 1.9 ± 2 mg/kg 6±8 39±28 5 PCS = Patient controlled Sedation. P < 0.05 between groups. Table 3: The Icidence of Intraoperative Complications in the two groups of patients. Characteristic Group P Group R Nausea / Vomiting 2 5* Pain 2 1 Excessive Sedation 0 0 Uncooperative 0 0 Induction of General Anaesthesia 0 0 Seizures 1 1 Airway Obstruction 0 1` Transient Respiratory Rate Depression 1 4* Desaturation 1 2 Hypercapnia 2 5 Hypotension 1 1 Bradycardia 2 1 Neurological Deficits 0 1 * statistically significant (p ≥ 0.05). PATIENT SEDATION SCORES (APPENDIX 1) SEDATION SCORE 5 4 GROUP P 3 GROUP R 2 1 1 2 3 4 5 TIME FROM PRE OPERATIVE (HRS) Fig. 1. patient sedation scores in the two groups at different time Intervals. AJAIC-Vol. (8) No. 2 June 2005 Alexandria Journal of Anaesthesia and Intensive Care 39 Table 4: Patient Satisfaction Questionaire Results Questionaire score (1-4 ) Satisfaction index PACU POD 1 POD 3 General level of comfort Group P 2.9±1.1 2.9±0.9 3.0±1.1 Group R 2.9±0.9 2.8±1.2 2.9±1.1 Willingness to use same technique In the future Group P 3.0±0.8 3.0±0.9 3.0±1.1 Group R 2.9±1.1 3.0±1.2 3.1±0.7 Satisfaction with patient-administration Group P 3.2±0.9 3.5±0.4 3.5±0.4 Group R 3.1±0.8 3.4±0.2 3.4±0.2 Data are presented as mean = SD PACU = post operative care unit POD = Post operative day. The introduction of ultra-short acting synthetic opioids opened a new door to the anaethetist whereby the drugs given in the infusion form can be titrated to effect. The choice of anaesthetic drugs depend on the individual anaesthesiologist. For conscious sedation, virtually all rely on some combination of a short acting opioid and a non narcotic sedative. The commonly used opioid include fentanyl, sufentanil and remifentanil and the sedatives used include midazolam, droperidol and propofol(15,16). Propofol offers the advantage of being a short acting sedative with antiemetic and amnestic properties. Considerable controversy regarding its anticonvulsant properties was easily overcomed by its stopping 15-20 minutes before neurophysiological monitoring to ensure minimal impact(16). This comparative study of propofol versus remifentanil for sedation during awake craniotomy showed more respiratory depression and perioperative nausea and / or vomiting with remifentanil. With propofol, there was more sedation, pain and hyoptension. Most of these side effects, as well as the depth of sedation, are dosedependent; thus the the titration of the AJAIC-Vol. (8) No. 2 June 2005 drugs by the use of patient controlled administration were attempted to be at an equi-sedative level in both groups. The chosen infusion rate of propofol (3mg/kg/h) in this study is in good accordance with the data previously published for sedation during regional blockade(17,18). Conversely, the initial remifentanil infusion rate was probably too high reflected by lower rate of PCS administration in group R when compared to group P. Sa Rego and coworkers(19) recommend remifentanil rather given as bolus increments of 0.25 µg/kg when needed instead of continuous infusion. However, when respiratory depression occurred, normalisation could be achieved rapidly by dose reduction because of the very rapid degradation of remifentanil(20). All the remifentanil patients were breathing adequately upon shortlasting stimulation. The optimal infusion rate for remifentanil during regional blockade can therefore be estimated around 0.075 µg/kg/min. The inclusion of a basal infusion is also advantageous during propofol for long procedures during which the patients often become restless or fatigued as the procedure progresses(21). A basal infusion provides a baseline level of sedation that Alexandria Journal of Anaesthesia and Intensive Care patients may augment by using PCS or asking for a bolus in response to clinical circumestances. As the number of patients in our study was small, the power of the study was calculated. The power was greater than 0.80 for all. Although, our centre is the most well known hospital in the whole middle east for awake craniotomies, the turn over number of cases is still very limited and a multi-centres study should be planned for future for this kind of surgeries. Nausea and vomiting are documented side–effects of opioids in general, including remifentanil, whereas propofol is known to have antiemetic properties (22). In this study, 5 patients experinced nausea and/or vomiting during surgery in the remifentanil group but only two in the propofol group. This is unpleasant for the patient and may induce movements disturbing the surgeon or even increase the risk of aspiration of gastric content in the sedated patients. The reported incidence of nausea and vomiting ranges from 8% to 50%. The different causative factors exacerbating nausea and vomittin include use of opioids, surgical stimulation such as stripping of dura, temporal lobe, meningeal vessle manipulation also insufficient analgesia combined with hypovolaemia. Various drugs have been tried to prevent and treat nausea and vomitting including ondansteron, dropridol and propofol(23). Two patients in group P (20 %) experienced intraoperative pain, one of them was due to irritation at the study drug iv site, that was overcomed by infusion to a larger bore iv cannula while the other patient experienced pain at the time of dural reflection and suturing and was overcomed by asking the surgion to infiltrtate the site of dural suturing. Only one patient in group R (10%), experienced pain during dural retraction that was treated by informing the surgeon to decrease the retraction. This difference AJAIC-Vol. (8) No. 2 June 2005 40 did not reach statistical significance (logistic regression analysis ). One patient in the propofol group (10%) experienced an episode of respiratory depression defined as respiratory rate < 8 breaths / min or SaO2 <95% for at least 1 min, compared to four patients in the remifentanil group (40%), (P < 0.01, Fisher’s Exact test). One patient in the propofol group and two patients in the remifentanil group experienced episodes of oxygen desaturation ≤ 90%. These episodes were of short duration and only in one case did study drug administration have to be inturrupted (remifentanil) for 3 minutes. In both groups, but more often in the remifentanil group, some patients experienced respiratory depression (defined as a respiratory rate of less than eight breaths per minute or oxygen saturation below 95%). When this problem was specifically addressed in a previous study(24) the administration of low doses of propofol to maintain concscious sedation or light sleep did not cause respiratory depression. The use of opioids for sedation carries with it a well known risk of respiratory depression(25) Due to rapid elimination and short context sensitive half-time with remifentanil(26) the episodes were shortlasting. Nevertheless, this study confirms that the administration of sedative or analgesic agents during regional anaesthesia necessiates close monitoring of repiratory function and provision of oxygen supplementation(27). However, opioids depress both the hypoxic and the hypercapnic ventilatory responses(22). Thus, oxygen supplementation and pulse oximeter monitoring may not protect against dangerous, high carbon dioxide levels. For this reason, continuous clinical assessment of respiratory function or endtidal carbon dioxide measurements should be applied when opioids are used for sedation. Patients achieved similar levels of sedation and were similarly satisfied with both techniques. Sedation score Alexandria Journal of Anaesthesia and Intensive Care values were higher in propofol than in remifentanil group during the whole period of surgery, but did not reach a value of statistical significance. Continuous basal infusion for both drugs maintain this level of sedation during the whole period of surgery in a relatively low dose of drugs administration. Propofol may exert a positive effect on mood(28,29), which has been postulated to contribute to the high levels of patient satisfaction which was noted in group P. Our results suggest that patient satisfaction is independent on this effects, if they exist, since satisfaction is maintained well into the third postoperative day. In conclusion, both propofol as a sedative, with antiemetic, euphoric and short duration of action, and remifentanil as an analgesic, sedative and ultra-short duration of action, is almost ideal agent for concious sedation in cases of awake craniotomy for epileptic surgeries. The method of their administration is for the anaethesiologist preference taking into consideration the utmost advantage of a continuous basal infusion for both drugs for these long procedures. The combination of both agent for this type of surgery may be the future study cocktail with lower doses and consequently, lesser side effects. Acknowledgements We deeply thanks Prof John Grivin(9), consultant of neurosurgery, King Faisal Specialist Hospital & Research Centre for his unlimited guidance, advises and co-operation . Appendix 1 Intraoperative Sedation Score Score Criteria 1. Fully awake and oriented 2. Drowsy, eyes open 3. Drowsy, eyes closed, but arousable to command 4. Drowsy, eyes closed arousable to mild physical stimulation 5. Unrousable to mild physical stimulation Appendix 2 Patient Satisfaction Questionaire Please help us evaluate your anaesthetic by completing the following questions. We are interested in your honest opinion, positive or negative. We also welcome your comments and suggestions. Circle your answer: 1. How satisfied were you with your pain management and overall level of comfort? ______4______ ______3_______ _________2________ __________ 1 _______ very satisfied mostly satisfied mildy satisfied or quite dissatified indifferent 2.If you were to have surgery again, would opt for the same method of management? ____ 1 ______ _____ 2 _______ ______ 3 ________ _________ 4 _______ no, definitely not no, I don’t think so yes, I think so yes, definitly 3. Did you like the method of self-administeration of sedative medication? ____ 4 ____ _____ 3 ______ _______ 2 _______ _________ 1 ________ yes, definitly yes, I think so no, I don’t think so no, definitly not AJAIC-Vol. (8) No. 2 June 2005 41 REFERENCES 1- Calhan LD, Engel J Jr: Surgery for epilepsy; a review. Acta Neurol Scan 1986;73:551-60. 2- Kofte W A, Tempelhaff R: Ane-sthesia for epileptic patients and for epileptic surgery. In: James Cottrell and David Smith (eds). Anesthesia and Neuorosurgery; 3rd ed. Churchill Livingstone, USA, 1994, 843-65. 3- Samra S: Anaesthetic management of awake craniotomy. Indian Society of Neuroanaesthesia and Critical Care 2001;131-4. 4- Arches DP, Mc Kenna JMA, Marin L, et al. Conscious sedation analgesia during Craniotomy for intractable epilepsy: a review of 354 consecu-tive cases. Can J Anesth 1988; 35: 338-44. 5- Silbergeld DL, Mueller WM, Colley PS, et al. Use of propofol (Diprivan) for awake craniotomies : technical notes. Surg Neurol 1992;38:271-9. 6- Rampill IJ, Lopez CE, Laxer KD, et al. Propofol sedation may disrupt interctable epileptiform activity from a seizure focus. Anesth Analg 1993;77:1071-3. 7- Ebrahim ZY, Schubert A, Van Ness P, et al. The effect of propofol seda-tion on seizures and intra cranially recorded epileptiform activity in pat-ient with partial epilepsy. Anesthesio-logy 1995;82:843-51. 8- Borkenstadt H, Perel A, Hadani M, et al. Monitored anesthesia care using remifentanil and propofol for awake craniotomy. J Neurosurg Anesthe-siol. 2001;13(3):246-9. 9- Grivin JP. Neurosurgical considera-tion and general methods for cranio-tomy under local anaesthesia. Int Anesthesiol Clin 1986;24:89-113. 10- Hans P, Bonhomme V, Born JD, et al. Target-controlled infusion of pro-pofol and remifentanil combined with bispectral index monitoring for awak craniotomy. Anaesthesia, 2000; 55(3): 255-59. 11- Blanshard HJ, Chung F, Mannienen PH, et al: Awake craniotomy for removal of intracranial tumour : consideration for early discharge. Anesth Analg 2001; 92:89-94. 12- Tongier WK, Joshi GP, L anders DF, et al. Use of the laryngeal mask airway during awake craniotomy for tumour resction. J Clin Anesth 2000; 12: 592-4. 13- Laborit H, Huguenard P : Pratique de phibernotherapie en chrurgie et en medicine. Paris : Masson (1954). 14- De Castro, Mundoleer P : Anesthsia Sans Barbituritiques, la neuroleptanalgesia. Anaesth Analg Reanimo 1959; 16: 1022-56. 15- Drummond JC, Iragui-Madoz VJ, Alksne JF, et al. Masking of epilepti-form activity by propofol durin seiz-ures surgery. Anesthesilogy 1992; 76: 652-4. 16- Ian A, Rosemary A, Adrian W ,et al. Propofol sedation during awake craniotomy for seizures: patient-controlled administration versus neurolepanal-gesia. Anesth Analg 1997;84:1285-91. 17- White PF, Negus JB. Sedative infu-sions during local and regional anesthesia: a comparison of mida-zolam and propofol. J Clin Anesth 1991; 3:32-9. 18- Pollock JE, Neal JM, Liu SS et al. Sedation during spinal anesthesia. Anesthesiology 2000;93:728-34. 19- Sa Rego MM, Inagaki Y, White PF. Remifentanil administration during monitred anaesthesia care: are intermittent boluses an effective alter-native to a contiuous infusion? Anesth Analg 1999;88:518-22. 20- Egan TD, Lemmens HJ, Fiset P, et al. The pharmacokinetics of the new shortacting opioid remifentanil (G187084B) in healthy adult male volunteers. Anesthesiology 1993; 79: 881-92. 21- Park WY, Watkins PA. Ptient-controlled sedation during epidural anaesthesia. Aneth Analg 1991; 72: 304-7. 22- Borgeat A, Wilder-Smith OH, Saiah M, et al. Subhypnotic doses of propofol possess direct antiemetic properties. Anesth Analg 1992; 74: 539-41. 23- Lichtor J, Zancy J: Psychological preparation and preoperative medication. Anaesthesia. In: Ronald D Miller (ed). Anesthesia, 4th ed. ChurchillLivingstone, The United Sates of Amirica, 1994, 1033-6. 24- McHardy FE, Fortir J, Chung F, et al. A comparison of midazolam, alfentanil, and propofol for sedation in outpatient Alexandria Journal of Anaesthesia and Intensive Care intraocular surgery. Can J Anesth 2000;47:211-14. 25- Dionne RA, Yagiela JA, Moore PA, et al. Comparing efficacy and safety of four intravenous sedation regi-mens in dental outpatients. J Am Dent Assoc 2001;132:740-51. 26- Hughes MA, Glass PS, Jacobs JR. Context-sensitive half-time in multicompartment pharmacokinetic mod-els for intravenous anesthetic drugs. Anesthesiology 1992;76:334-41. AJAIC-Vol. (8) No. 2 June 2005 43 27- Lauwers m, Camu F, Brevik H, et al. The safety and effictiveness of remifentanil as an adjunct sedative for regional anesthesia. Anesth Analg 1998;88:134-40. 28- Whitehead C, Sanders LD, Oldroyd G, et al. The subjective effect of low dose propfol. Anaesthesia 1994; 49: 490-6. 29- Harper N, Dunkley C, Hume D. Sedation using remifentanil. Anaes-thesia 2003; 58(2), 197-98.