Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
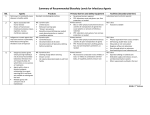
The Affordable Care Act and Women’s Preventive Care Services In accordance with the Affordable Care Act (ACA) and corresponding regulations, Coventry Health Care expanded women’s preventive care benefits to ensure that women have access to a full range of preventive services without cost sharing. EXPANDED PREVENTIVE CARE SERVICES For Coventry fully insured group health plans that are not grandfathered plans, the following preventive care services will be included without cost sharing: • Well-woman visits (including prenatal visits) • Screening for gestational diabetes • Human papilloma virus (HPV) DNA testing for women 30 years and older • Risk-reducing medications, such as tamoxifen and raloxifene, for women 35 years and older who have an increased risk for breast cancer • Sexually transmitted infection counseling • Human immunodeficiency virus (HIV) screening and counseling • FDA-approved contraception methods and contraceptive counseling (subject to standard medical management and formulary restrictions)* • Breastfeeding support, supplies (manual or standard electric pumps) and counseling • Domestic violence screening and counseling To be covered with no additional cost sharing, these services must be done by in-network physicians. Most self-funded plans are required to offer similar coverage without cost sharing. Please note: Coventry will cover most contraceptive prescriptions with no cost share. However, there are some contraceptive prescriptions for which members will have to pay a deductible, copayment or coinsurance. Contraceptive prescriptions that Coventry covers with no cost sharing are listed in the chart at the end of this document. OVER-THE-COUNTER FEMALE CONTRACEPTIVES Over-the-counter female contraceptives will be covered with no cost-sharing for members ONLY with a prescription. *Certain religious employers that offer insurance to their employees are not required to cover contraceptive services. ©2015 Coventry Health Care, Inc. All rights reserved. PREV.SERVICES.EMP.0615 Some Facts about the Benefits of Women’s Preventive Services ■ The Centers for Disease Control and Prevention (CDC) states that most cervical cancers are preventable with regular screenings and follow-up treatment. They are also very curable when found early. ■ HPV DNA testing can detect the presence of high-risk HPV strains in cervical cells, which can lead to cervical cancer, according to the CDC. Source: http://www.cdc.gov/Features/ CervicalCancer/ The Affordable Care Act and Women’s Preventive Care Services CONTRACEPTIVE PRESCRIPTIONS Coventry will cover the contraceptive prescriptions listed below with no cost sharing for members receiving these drugs or devices for the prevention of conception. Contraceptives not on this list will be covered at the applicable member cost share. (Please note: This list is subject to change.) Altavera Alyacen Amethia/Lo Amethyst Apri Aranelle Aubra Aviane Azurette Balziva Briellyn Camila Camrese/Lo Caziant Chateal Cryselle Cyclafem Dasetta Daysee Deblitane Delyla Desogestrel/ethinyl/estra Drospirenone-Ethinyl Estradiol Elinest Ella Emoquette Enpresse Enskyce Errin Estarylla Falmina Femcap Gianvi Gildagia Gildess/Fe Gynol Heather Implanon^ Introvale Jencycla Jolivette Junel Junel Fe Kariva Kelnor 1-35 Kurvelo Larin/Fe Leena Lessina Levonest Levonorgestrel Levonorgestrel-Eth-Estradiol Levora Loryna Low-Ogestrel Lutera Lyza Marlissa Medroxyprogesterone vial 150mg Microgestin/Fe Mirena^ Mono-Linyah Mononessa Myzilra Necon 1/35 Nexplanon^ Next Choice Nikki Nora-Be Norethindrone Acetate Norgestimate-Ethiny-Estradiol Norgestrel-Ethinyl-Estradiol Norlyroc Nortrel 1/35 Nuvaring Ocella Ogestrel Orsythia Ortho-Diaphragm Paragard T 380-A^ Philith Pirmella Plan B Plan B One-Step Portia Previfem Quasense Reclipsen Sharobel Skyla^ Solia Sprintec Sronyx Syeda Tilia Fe Today Contraceptive Sponge Tri-Estarylla Tri-Legest Fe Tri-Linyah Tri-Previfem Tri-Sprintec TriNessa Trivora VCF Velivet Vestura Viorele Vyfemla Wera Wide Seal Diaphragm Wymzya Fe Xulane Zarah Zenchent/Fe Zovia ^May be covered under your medical benefit. Please refer to your health plan documents. The Affordable Care Act and Women’s Preventive Care Services This plan does not cover all health care expenses and includes exclusions and limitations. Members should refer to their plan documents to determine which health care services are covered and to what extent. The following is a partial list of services and supplies that are generally not covered. However, your plan documents may contain exceptions to this list based on the plan design or rider(s) purchased. • A ll medical and hospital services not specifically covered in, or which are limited or excluded by your plan documents, including costs of services before coverage begins and after coverage terminates. • Cosmetic surgery. • Custodial care. • Dental care and dental x-rays. • Donor egg retrieval. • Durable medical equipment. • Experimental and investigational procedures, (except for coverage for medically necessary routine patient care costs for Members participating in a cancer clinical trial). • Hearing aids. • Home births. • Immunizations for travel or work. • Implantable drugs and certain injectable drugs including injectable infertility drugs. • Infertility services including, but not limited to, artificial insemination and advanced reproductive technologies such as IVF, ZIFT, GIFT, ICSI and other related services unless specifically listed as covered in your plan documents. • Nonmedically necessary services or supplies. • Orthotics except diabetic orthotics. • Outpatient prescription drugs (except for treatment of diabetes), unless covered by a prescription plan rider and over-the-counter medications (except as provided in a hospital) and supplies. • Radial keratotomy or related procedures. • Reversal of sterilization. • Services for the treatment of sexual dysfunction or inadequacies including therapy, supplies or counseling. • Special duty nursing. • Therapy or rehabilitation other than those listed as covered in the plan documents. • Weight control services including surgical procedures, medical treatments, weight control/loss programs, dietary regimens and supplements, appetite suppressants and other medications; food or food supplements, exercise programs, exercise or other equipment; and other services and supplies that are primarily intended to control weight or treat obesity, including Morbid Obesity, or for the purpose of weight reduction, regardless of the existence of comorbid conditions.