Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
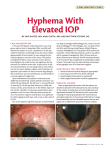
Hyphema Rhea V. Morgan, DVM, DACVIM (Small Animal), DACVO BASIC INFORMATION Description Hyphema is blood in the front chamber of the eye. The blood may be clotted, or it may move freely. Free blood often settles when the animal is quiet, then disperses and becomes more noticeable when the animal is active. Causes Numerous causes of hyphema exist, including the following: • Trauma—blunt or penetrating • Abnormalities of blood clotting • Hypertension (high blood pressure) • Excessively high circulating protein levels (hyperviscosity) or number of red blood cells (polycythemia) • Inflammation of the eye (uveitis), especially uveitis associated with certain tick-borne infections (ehrlichiosis, Lyme disease, and others) • Movement of the lens within the eye and following retinal detachment • Tumors of the eye • Congenital birth defects of the eye, such as persistence of certain blood vessels and structures that should disappear soon after birth or the collie eye anomaly • As a complication of eye procedures or surgery Clinical Signs Hyphema is usually diagnosed by a thorough eye examination. The eye examination often involves tear testing, fluorescein staining of the cornea, glaucoma testing, and evaluation of the deeper structures of the eye. Diagnostic Tests Once the presence of hyphema is confirmed, a search is instituted for the cause. A complete physical examination is conducted to look for other evidence of bleeding or an underlying cause. Routine laboratory tests, blood pressure measurement, blood clotting tests, and assays for tick-borne diseases may be recommended. If there is too much blood in the eye to allow examination of the deeper structures, an ocular ultrasound may be helpful. X-rays of the skull may be done to look for metallic foreign bodies and evidence of trauma. Further testing may be needed if a systemic cause is found, to better define its effects on other organs of the body. TREATMENT AND FOLLOW-UP Treatment Options Therapy for hyphema involves treating both the eye and the underlying cause. Appropriate treatment of the cause often helps prevent further hyphema. Affected animals are kept quiet to decrease the chance of further bleeding. If the cornea is not ulcerated, topical steroids are started, because the hyphema commonly causes inflammation within the eye. Topical atropine is often used to dilate the pupil, unless secondary glaucoma is present. If glaucoma is detected, then anti-glaucoma drugs are started. Injection into the eye of drugs that dissolve clots may be tried when hyphema occurs after surgery on the eye. Follow-up Care Close monitoring of the eye is needed until the hyphema resolves, which can range from days to months. Repeated staining of the cornea and glaucoma testing are performed. Laboratory tests and blood pressure measurements may be repeated periodically, depending on the underlying cause. Prognosis Prognosis is highly variable. If the hyphema is mild and associated with trauma or a disease that can be effectively treated, the prognosis is good. Mild hyphema may resolve within days and may have no effect on vision. If hyphema is severe, or if it is accompanied by bleeding into the back of the eye or by a retinal detachment, then the eye will be permanently blind. Severe hyphema may also lead to either shrinkage of the eye (over several weeks to months) or secondary glaucoma. If severe, unresponsive secondary glaucoma develops, then removal of the eye may be considered. Hyphema that does not respond to topical therapy or is caused by diseases that are difficult to treat has a poor to guarded (uncertain) prognosis. In these cases, the hyphema can persist for long periods of time and can recur. Long-standing hyphema can disrupt the nutrition of the lens, which leads to cataract formation. IF SPECIAL INSTRUCTIONS HAVE BEEN ADDED, THEY WILL APPEAR ON THE LAST PAGE OF THE PRINTOUT. Copyright © 2011 by Saunders, an imprint of Elsevier Inc. All rights reserved.