Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
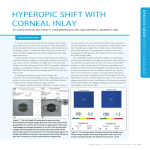
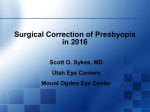
Slide 1 ___________________________________ ___________________________________ ___________________________________ VA N D I R I M E R , O D D I PLOM AT, A M E RI CA N B OA RD OF OPTOM E TRY ___________________________________ [email protected] 3 0 3 - 74 0 - 5 4 7 5 ___________________________________ ___________________________________ ___________________________________ Slide 2 ___________________________________ PRESBYOPIA Ahhhh, the presbyope! “I want to see all distances without glasses” As clinicians we have all heard this, probably at least once a day. ___________________________________ What are your options? Bifocals Progressives Mono vision contacts Multi-focal contacts Multi-focal IOL’s ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 3 PRESBYOPIA The newest option in our near future………… CORNEAL INLAYS 3 Inlay Designs • Kamra • Raindrop • Presvia Flexivue Microlens ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 4 ___________________________________ CORNEAL INLAYS • 3 variations on the concept of placing an implant inside the cornea are in different stages of the approval process. • Kamra inlay (from AcuFocus in Irvine, Calif.) Uses the pinhole principle to increase depth of field • Raindrop (from ReVision Optics in Laguna Hills, Calif.) makes the cornea multifocal by reshaping it • Flexivue Microlens (from Presbia in Amsterdam) creates multifocal vision using an in-cornea lens. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 5 ___________________________________ KAMRA INLAY • • • • Inlay is placed under a corneal flap It can be placed in an emmatropic eye or after LASIK procedure has been performed The inlay is placed into the non dominant eye The Kamra inlay is commercially available in 49 countries, and nearly 20,000 inlays have been implanted worldwide to date ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 6 ___________________________________ ___________________________________ 3.8mm Total diameter 1.6mm Aperture 5μ Thick ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 7 ___________________________________ 8,400 ___________________________________ micro-perforations (5-11µ) Pseudo-random pattern ___________________________________ Maximize nutrient flow Minimize visual symptoms ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 8 ___________________________________ KAMRA INLAY The KAMRA™ (Acufocus, Inc.) Inlay extends uses small aperture optics to depth of focus Published clinical and commercial results are similar: ___________________________________ Mean UNVA: J1 with 96-97% of eyes J3 or better Mean UIVA: 20/20 - 20/25 Mean UDVA: 20/20 ___________________________________ Can be used to treat a broad range of presbyopes Result remains stable over the long-term ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 9 ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 10 Reading Performance after Small-Aperture Corneal Inlay Journal of Cataract and Refractive Surgery March 2011 • Improved near visual acuity in all 32 patients • Mean improvement of 2.7 +/- 1.6 lines of near vision • LogMAR of 0.38 +/-0.14 (approx 20/50) • Improved vision due to increased depth of field based on small aperture optics. • Completely reversible procedure • Distance acuity was maintained at 20/20 ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 11 KAMRA INLAY RESULTS ___________________________________ MEDSCAPE.COM -FDA PANEL DELIVERS MIXED VERDICT ON KAMRA CORNEAL INLAY JUNE 9, 2014 The primary effectiveness endpoint, • 75% of the subjects achieving uncorrected near visual acuity of 20/40 or better at 12 months, • 83.5% of the 478 subjects who completed 12 months of the study and remaining consistent through 36 months. • Participants had a mean 2.9-line gain at month 12. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 12 KAMRA INLAY RESULTS • Subject satisfaction questionnaires on a scale of 1- 7 • Baseline near vision was 1.7 and improved to 4.7 at 12 months • Remained consistent at 4.7 for 3 years • Safety findings by clinical investigator Jay S Pepose, MD, Phd • 0.6% rate of persistent BCDV LOSS of 2 lines or more at consecutive visits at 12 months • 0% incidence of BDCVA worse than 20/40 if they were 20/20 or better pre op • 3.3% of patients had increased ocular pressure • 5.9% with decreased BCDVA more than 2 lines at 3+ months • Outcomes were better in procedures with a femtosecond laser that created a “POCKET” rather than a flap. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 13 KAMRA INLAY – INTRALASE POCKET • In a subsequent confirmatory trial of 151 subjects • Using an intralase pocket with a separation of spot/line settings of 6x6 microns as the surgical standard. • Primary endpoint improved to 90.8% with a drop in inlay removals caused by refractive changes. Outcomes went from 6.9% to 2.7%. The 6x6 is now the standard. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 14 KAMRA • Being able to remove the inlay if the patient is unhappy is a big advantage. “Previous papers have reported that patients’ refractive state returned to within ±1 D of the preoperative refractive state after inlay removal, with no loss of corrected distance visual acuity. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 15 FDA – MIXED VERDICT • Panel members were convinced 7 to 1 that there is "reasonable assurance" it improves near vision in presbyopic patients • However, the committee split down the middle 4 to 4, on the question of reasonable assurance of safety • triggering a tie-breaking "no" vote from committee chair Neil M. Bressler, MD. on a third question, whether the inlay's benefits outweigh its risks, the vote was 4 yes, 3 no, and 1 abstention. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 16 FDA’S TAKE • FDA Chief Ophthalmic medical officer Eva Rorer, MD faulted AcuFocus for excluding 8.7 (44) subjects for removing the lens because of visual problems, they believe the subjects should have been counted as failures- which dropped the endpoint to 75.8% • Only 25% from both trials gained 4 or more lines of UCNVA, which is equal to 1D of accommodation. • One of the “no” votes from Dr. Alvin Eisner, PhD was due to concerns about outcome of explanted patients over time and the uncertainty of hyperopic shift over time. In addition, the intereference of the device with ophthalmic examinations. The device may affect the clinicians ability to see the retina. • The “abstain” vote by Dr. Dahr stated it is very difficult to determine “Benefit” when there is such a subjective variability from patient to patient when it comes to a patient’s “perceived” benefit. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 17 PRESVIA FLEXIVUE MICROLENS ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 18 FLEXIVUE MICROLENS INLAY ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 19 FLEXIVUE MICROLENS ___________________________________ • Placed into a stromal pocket instead of under flap ___________________________________ • Ziemer Femto laser device with a proprietary pocketmaking algorithm ___________________________________ • Pre-loaded delivery system ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 20 THE PRESBIA FLEXIVUE MICROLENS ___________________________________ • Small, hydrophilic acrylic refractive inlay • 3.2 mm wide, with a 1.6-mm hole in the center. • The refractive power of the ring ranges from +1.5 D to +3.5 D. • Presbia announced in November that the FDA had given conditional approval to begin a Phase II trial of the inlay. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 21 PRESVIA FLEXIVUE MICROLENS ___________________________________ • Placed in the nondominant eye of a patient who is emmatropic in both eyes • Creates a slight myopic shift and a mild multifocal effect in the implanted eye. • ___________________________________ Creating a small amount of monovision. • A mixture of a little monovision and multifocality, very welltolerated. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 22 ADVANTAGES OF FLIXIVUE LENS • The main advantage the Flexivue has compared to the other inlays is its more physiologic approach to correcting near vision. • Unlike the pinhole mechanism of action used by the Kamra inlay, it provides an optical correction depending on the refractive defect present,” he says. • Does not have issues regarding distribution of nutrients, which is a factor with Raindrop and Kamra inlays. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 23 FLEXIVUE MICROLENS • It is advised to do a contact lens mono vision trial with a +1.50 contact lens in the nondominant eye prior to surgery. it gives the patient the opportunity to experience the controlled monovision the inlay produces • FDA-approved Phase II clinical studies are just starting. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 24 FLEXIVUE MICROLENS • Small Cohorts with positive results • Limited published research, nothing published in peer-reviewed journals • Prospective study 47 emmatropes with inlay implanted in nondominant eye • UCNVA 20/32 or better in 75% of eyes at 12 months • UCDVA unaffected • Decreased contrast sensitivity • Patient satisfaction and level of spectacle independence was high ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 25 FLEXIVUE MICROLENS (PRESBIA) • Inlay provides distance vision through a plano central zone that is surrounded by a ring of varying add power for near vision, similar to a multifocal contact lens or multifocal IOL. • 3.0 mm diameter lens with UV blocker • 1.5 mm opening in the center to facilitate flow of fluid nutrients • Plano central zone, peripheral refractive zone with add power from +1.25 to +3.50 D • Cosmetic appearance of inlay not of concern, as in KAMRA ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 26 RAINDROP NEAR VISION INLAY ___________________________________ REVISION OPTICS INC. • Clear Hydrogel Lens • Very small diameter optics • Hyperprolate shape designed to reshape the anterior corneal curvature • Enhances near and intermediate vision via multi-focal affect ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 27 REVISION OPTICS’ RAINDROP ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 28 RAINDROP INLAY • Formerly known as PresbyLens in the U.S. and Vue+ in Europe • 2mm diameter inlay is made of medical-grade hydrogel plastic similar to that used for soft contact lenses and has optical characteristics that are almost identical to the human cornea, according to the company. • The inlay improves both near and intermediate vision, as demonstrated by a study involving 38 people who received the Raindrop Near Vision implant in their non-dominant eye • The Raindrop Near Vision corneal inlay is placed within the cornea under a LASIK-style flap. When in position, the inlay changes the curvature of the cornea so the front of the eye acts much like a multifocal contact lens. • The inlay has no power. ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 29 RAINDROP INLAY • Effective in a variety of situations, including bilateral implantation in hyperopic patients. • 23 hyperopic subjects implanted, non-dominant eye first then 6 months later in the dominant eye. • Near vision improved from LogMar 0.54 to -0.04. Distance and intermediate vision also improved and remained stable (article doesn’t state by how much) • Bilateral implantation improved near vision by one line of acuity • 80% of bilateral subjects were 20/20 or better at all distances at follow up visits • 9 months post op all subjects (N=23) were satisfied with their vision • Very Important to trial with multi-focal contact lenses to see if they adapt well ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 30 CONTRAINDICATIONS FOR INLAYS • • ___________________________________ Previous ocular surgeries Any ocular pathology, • Keratectasia • Corneal degeneration • Severe blepharitis • Retinal disease • Glaucoma • Cataract • Topographic irregularities • Severe dry eyes – treat aggressively prior to surgery ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 31 DISADVANTAGES OF INLAYS • All of them reduce distance vision to some degree. • Trade-off for improved reading vision ___________________________________ ___________________________________ • All of them cause some night glare • Using an inlay requires a compromise in distance vision. • Nondominant eye in a patient who is a good adapter usually does well ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 32 DISCLOSURE ___________________________________ The information in this lecture was found on: http//www.reviewofophthalmology.com/content/t/c ornea/c/46512/#sthash.CwNwW9Wz.dpuf. Inlays and Presbyopia: The Next Froentier http//www.allaboutvision.com FDA web-site Medscape.com FDA Panel Delivers Mixed Verdict on KAMRA corneal inlay by Mirian E. Tucker June 9, 2014 ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 33 U.S. TRENDS IN REFRACTIVE SURGERY: 2014 ISRS SURVEY ___________________________________ ___________________________________ R I C H A R D J . D U F F E Y, M D D AV I D L E A M I N G , M D ___________________________________ R E F R A C T I V E S U B S P E C I A LT Y D AY CHICAGO: OCTOBER 17, 2014 ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 34 ___________________________________ 2014 SURVEY Sixth year of ONLINE*** Survey E-mailed to 1022 U.S. ISRS members; 486 Opened Eighteenth year of refractive data collection overall ___________________________________ 15% response rate of the membership’s opened e-mail requests analyzed by October 8, 2014. ___________________________________ Alphabet soup of refractive surgery including corneal and lens-based surgeries, premium IOLs, and FS cataract surg. ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 35 PREFERRED SURGERY FOR A 30 YO -10.00 DIOPTER MYOPE ___________________________________ ___________________________________ * 40% LVC 50 43 45 40 35 27 30 '05 '08 25 20 ___________________________________ '11 13 15 '12 11 10 '13 3 5 1 '14 0 Never Surface Ablation LASIK RLE P-IOL WAIT ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 36 ___________________________________ EXCIMER LASER MOST COMMONLY USED 70 50 '97 60 '00 44 '06 * 40 ___________________________________ '03 50 '09 30 '10 20 '11 '12 10 ___________________________________ '13 '14 0 VisX Wavelight B and L Schwind 6 0 ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 37 FLAPMAKER MOST COMMONLY USED ___________________________________ * 71% femtoflaps 52 60 '98 50 '00 ___________________________________ '04 40 '07 30 '10 6 '11 20 11 8 10 0 10 5 4 0 B-L Moria Amadeus '12 ___________________________________ '13 1 '14 Nidek B-D Intralase Ziemer Other FS ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 38 ___________________________________ COMANAGEMENT 80 70 '00 60 '04 50 '07 55 '10 45 40 ___________________________________ '11 30 '12 20 '13 10 '14 11 ___________________________________ 0 Yes No ___________________________________ >50% DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 39 PREFERRED FLAP THICKNESS (WHEN NO OTHER CONSTRAINTS) ___________________________________ ___________________________________ 68 70 60 '04 50 '07 40 30 '10 30 ___________________________________ '11 20 '12 10 '13 1 0 80 1 100 120-130 '14 150-160 ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 40 ___________________________________ MINIMUM RESIDUAL STROMAL BED THICKNESS REQUIREMENT FOR LASIK * 64% at 275 microns or greater ___________________________________ 80 '04 70 '07 60 '08 50 '10 40 ___________________________________ '11 36 34 30 '12 20 23 '13 10 '14 0 225 1 200 0250 275 4 350 325 1 300 ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 41 ___________________________________ TOTAL CASES OF POST LASIK ECTASIA AS THE PRIMARY SURGEON IN CAREER ___________________________________ 60 50 '04 40 * Slight Growth Rate '06 32 30 ___________________________________ '10 '11 20 17 19 '12 10 11 7 6 '13 6 3 0 0 1 2 3 4 5 '14 6 to 10 ___________________________________ >10 DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 42 MINIMUM CENT. CORNEAL PACHYMETRY FOR LASIK (ALL OTHER PARAMETERS NORMAL) ___________________________________ 49 50 * 73% OK with 480 or less 45 ___________________________________ 40 35 '05 30 '08 26 '10 25 '11 20 '12 15 11 13 10 '13 ___________________________________ '14 5 1 0 0 540 microns 520 500 480 460 no limit ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 43 TOTAL LVC VOLUME IN ISRS (X1000) 600 549 500 428 '08 '09 '10 '11 '12 '13 '14 400 300 200 121 100 0 Surface Ablation DUFFEY/ LEAM IN G 2014 ___________________________________ LASIK ___________________________________ ___________________________________ ___________________________________ Total LVC *22% Increase in Total LVC from 2012-13. *Ratio of PRK / Total LVC remained at 22% over past four years. ___________________________________ ___________________________________ ___________________________________ Slide 44 ___________________________________ 2014 ISRS SUMMARY Thinner flaps dominate: 100 micron or less flaps are favored by 68% of surgeons (up from 12% in ‘04). ___________________________________ Preferred RSB thickness is stable: 34% think 250 microns is adequate, but 65% recommend 275 microns or more. New post-LASIK ectasia cases show a slight rise in rate. ___________________________________ ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 45 ___________________________________ 2014 ISRS SUMMARY During cataract surgery 68% of surgeons will offer to correct astigmatism if it is 0.75 D or more; 97% if 1.25 D or more. ___________________________________ LRI/AK preferred (91%) if K astigmatism <1.0D Toric IOL preferred (77%) if K astigmatism > 1.12D CXL offered by 23% of ISRS members surveyed in the U.S. (not FDA-approved). ___________________________________ ___________________________________ DUFFEY/ LEAM ING 2014 ___________________________________ ___________________________________ ___________________________________ Slide 46 UPDATES ON REFRACTIVE SURGERY MED’S We are changing from Durezol to Lotemax “GEL” BID x7d then QDx7d Besivance TID x 7d Ilevro QD or Nevanac TID x 5d FOR PRK Patients (harder to get now) ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 47 LOTEMAX “GEL”- COUPONS AVAILABLE ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 48 REMINDER ___________________________________ Have your patient’s come in for Testing PRIOR to the surgery day • • • Wavescans – • patients can accommodate a lot and we have difficulty getting the scans. This can significantly delay the surgery team and add more time your patient is at the surgery center on their day of surgery. • Small pupils can affect our ability to get wavescans and they may need to be changed to conventional surgery. This can be avoided if testing is done prior to the surgery day. We can use a diluted dilating drop to slightly open the pupil to get the wavescans. The pupil CANNOT be dilated on surgery day. Topographies – • At times, a topography can make or break the decision of LASIK vs PRK. It is much easier to discuss the procedural change with a patient PRIOR to their surgery day. This allows them to schedule more time off work and start the medications prior to surgery if switched from LASIK to PRK. ___________________________________ ___________________________________ It can SAVE AT LEAST AN HOUR OF TIME ON SURGERY DAY! ___________________________________ ___________________________________ ___________________________________ ___________________________________