Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
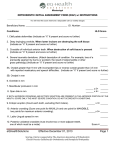
ORIGINAL ARTICLE The effectiveness and long-term stability of overbite correction with incisor intrusion mechanics Huda Al-Buraiki,a Cyril Sadowsky,b and Bernard Schneiderc Chicago, Ill Background: Correction of deep overbite with subsequent achievement of long-term stability is difficult. The purpose of this study was to investigate the effectiveness and long-term stability of overbite correction with incisor intrusion mechanics. Methods: The treated group consisted of 25 subjects (13 female, 12 male) with deep overbite of at least 4 mm (mean overbite, 5.9 mm). The orthodontic treatment was initiated in the late mixed or early permanent dentition, and all patients were treated nonextraction. All patients had lateral cephalometric radiographs taken at pretreatment (T1), posttreatment (T2), and postretention (T3). The treatment included cervical headgear and lever arches to intrude mainly the maxillary incisors and occasionally the mandibular incisors. Premolars were not included in the fixed appliances during the treatment. The untreated group consisted of 25 age- and sex-matched subjects from the Bolton Growth Study. Results: The mechanics used were effective in overbite correction. During the posttreatment period, overbite increased by 0.7 mm. Conclusions: Although this change was statistically significant, the amount was small and is considered clinically insignificant, given the severity of the overbite pretreatment. Furthermore, a net overbite correction (T3-T1) of 3.3 mm and postretention overbite on 2.6 mm is an excellent clinical outcome. (Am J Orthod Dentofacial Orthop 2005;127:47–55) D eep overbite is a common feature of many malocclusions. One of the objectives of orthodontic treatment is to establish a normal overbite. A review of the literature reveals a great controversy among the proponents of the different treatment modalities. Some investigators insist that overbite is best treated by incisor intrusion to a leveled functional occlusal plane. The smile line has been used to help determine which incisors to intrude. Others resorted to “leveling and aligning,” using continuous archwires, achieving overbite correction by extrusion of the buccal segments with minimal intrusion and some proclination of incisors. Many studies have been performed to examine the types and amounts of postretention relapse after orthodontic treatment.1-6 All studies showed that overbite decreased during treatment and had a tendency to From the Department of Orthodontics, University of Illinois at Chicago. a Former resident. b Professor. c Clinical professor. Reprint requests to: Dr Cyril Sadowsky, University of Illinois at Chicago, College of Dentistry, Department of Orthodontics (MS 841), 801 South Paulina, Chicago, IL 60612; e-mail, [email protected]. Submitted, July 2003; revised and accepted, October 2003. 0889-5406/$30.00 Copyright © 2005 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2003.10.034 increase after treatment. The degree of relapse varied from one study to another (Table I). The majority of the stability studies were focused on quantifying the amount of relapse and identifying the factors that might have contributed to it, such as extraction, pretreatment overbite, and intercanine distance. In addition, overbite was one of several variables studied rather than the main focus of these studies. Thus, very few studies have described the mechanotherapy and its effectiveness in overbite correction. The purpose of this study was to investigate the effectiveness and long-term stability of overbite correction with incisor intrusion mechanics. MATERIAL AND METHODS Records of the treated group were obtained from the office of Dr Andrew Haas, Cuyahoga Falls, Ohio. The group consisted of 25 subjects (13 female, 12 male) with deep overbite of at least 50% mandibular incisor overlap. Twenty-two subjects had Class II, Division 1 malocclusion, and 3 had Class I malocclusion. The orthodontic treatment was initiated in the late mixed or early permanent dentition, and all patients were treated nonextraction. Premolars were not included in the fixed appliances during treatment, as is often the case in this practice. All patients had lateral cephalometric radio47 48 Al-Buraiki, Sadowsky, and Schneider Table I. American Journal of Orthodontics and Dentofacial Orthopedics January 2005 Literature survey of overbite treatment outcome Overbite Authors, year (reference) T1 (mm) T2-T1 (mm) ⌬ (%) T3-T2 (mm) Relapse (%) Bishara et al, 1973 (1) Hellekant et al, 1989 (2) Fidler et al, 1995 (5) 4.7 ⫾ 1.8 ⫺1.7 36 0.4 23 5.1 ⫾ 1.4 ⫺2.5 49 0.8 32 4.4 ⫾ 1.6 ⫺1.5 ⫾ 1.8 34 0.9 ⫾ 1.6 60 Sadowsky et al, 1994 (4) 4.5 ⫾ 1.9 ⫺1.9 ⫾ 1.9 42 0.5 ⫾ 1.1 26 Carcara 2001, (6) 4.8 ⫾ 2.2 ⫺2.7 ⫾ 1.1 56 0.8 ⫾ 0.9 30 Table II. Malocclusion Class II Division 1 Class II Division 1 Class I; Class II Division 1; Class II Division 2 Class II Treatment Edgewise appliance Edgewise appliance Headgear, edgewise appliance Headgear, edgewise appliance Headgear, edgewise appliance Retention time (y) Postretention Time Mean 14.8 mo ⱖ2 y Mean 14 y 8.4 ⫾ 3.2 6.3 ⫾ 1.8 y 3.3 Mean 7.4 y Characteristics of treated group Time (y) Characteristic Mean SD Range Age at T1 Age at T2 Age at T3 Treatment time (T2-T1) Posttreatment duration (T3-T2) Retention time Maxillary Mandibular Postretention time Maxillary Mandibular 11.3 14.2 26.6 3 12.3 1.7 2 4 1.5 3.9 8.2-15.1 10.8-18.3 20.2-38.4 0.9-4.9 7.7-25.7 5 8 1.3 1.3 2.3-7.7 6.1-12.1 7.3 4.3 4.3 3.9 2-20.3 1-18.3 graphs taken at pretreatment (T1), posttreatment (T2), and postretention (T3). A member of the auxiliary staff in the office identified records that satisfied the selection criteria described above. Table II summarizes the characteristics of the sample. All subjects were treated by a single operator with a .018 ⫻ .025-in standard edgewise appliance. In the mechanotherapy, the principle of the lever arch was used to intrude incisors or prevent their eruption. The .017 ⫻ .025-in or .018 ⫻ .025-in mandibular archwire was stepped down mesial to the molar tube, bypassing the buccal segments and engaging the incisors anteriorly. The .017 ⫻ .025-in or .018 ⫻ .025-in maxillary ideal archwire was gabled several millimeters anterior to the molar tube to engage the incisors anteriorly while bypassing the canines and premolars. When engaged, the maxillary archwire had an intrusive and lingual root torque effect on the incisors. The anteroposterior dis- crepancy was corrected with cervical headgear, with the outer bow long and bent up to deliver a distal root moment to the first molars (counteracting the mesial root thrust created by the intrusion arch). An intrusion force (with a slight retraction vector) was delivered to the maxillary incisors by the elastics (2-4 oz) worn from canine hooks on the inner bow of the cervical headgear and engaging the incisal wings of the brackets of the maxillary incisors. Tandem mechanics was initially used in 16 of the 25 patients with mandibular arch length deficiency. Tandem mechanics included a cervical headgear together with a mandibular .022-in archwire engaged in the mandibular molar headgear tube and directly ligated to the mandibular incisors with a V-shaped bend in the canine region. Sliding hooks and active open-coil springs were then inserted distal to the bend and Class III elastics attached to the hooks to avoid mandibular incisor proclination. Al-Buraiki, Sadowsky, and Schneider 49 American Journal of Orthodontics and Dentofacial Orthopedics Volume 127, Number 1 Table III. Age and sex distribution of treated and untreated groups T1 age (y) Sample Treated Female Male Total Untreated Female Male Total T2 age (y) n Mean SD Mean SD 13 12 25 11.2 11.3 11.3 1.6 1.8 1.7 14 14.4 14.2 1.8 2.3 2 13 12 25 11.3 11.4 11.3 1.6 1.6 1.6 14.1 14.4 13.3 1.6 2 1.8 At the completion of active treatment, the appliances were removed, and retainers were inserted. The maxillary retainer consisted of a Hawley appliance with a passive anterior bite plane. The patients were instructed to wear the retainers for 24 hours per day for 5 years. In the mandible, a fixed lingual wire was used. Some patients had a bonded canine-tocanine wire, whereas others had a bonded firstpremolar-to-first-premolar wire. Patients were observed until a decision was made regarding the future of the third molars. The T3 records were taken, on average, 7 years 4 months and 4 years 4 months after the removal of maxillary and mandibular retainers, respectively (Table II). The untreated group consisted of 25 age- and sex-matched subjects (13 female, 12 male) who exhibited Class II, Division 1 malocclusion with deep overbite but had not undergone any orthodontic treatment. The cephalograms for this group were drawn from copies of the Bolton Growth study, available in the Department of Orthodontics, University of Illinois at Chicago. Owing to the limited number of subjects with a T3 record matching the age of subjects in the treated group, only T1 and T2 records were used. Table III summarizes the age and sex distribution of the treated and untreated groups. Both skeletal and dental variables were measured on the individual cephalogram at T1, T2, and T3. The skeletal variables included the ANB, mandibular plane angle, Y-axis, the upper, lower, and total anterior face heights, and finally, the lower anterior face height ratio (Fig 1). The dental variables included overjet (the horizontal distance between the maxillary and mandibular incisor tips measured parallel to the functional occlusal plane), overbite (the vertical distance between the incisal tip of the maxillary and mandibular incisor), and the interincisal angle. Additional variables were measured with cephalometric superimposition. The overall superimposition was patterned after Björk and Skieller,7 registering on Fig 1. Skeletal variables measured on individual cephalograms. P, porion; S, sella; Or, orbitale; A, A-point; B, B-point; PO, pogonion; Gn, gnathion; Me, menton; N, nasion. Measurements: 1, ANB angle; 2, mandibular plane angle; 3, y axis; 4, upper anterior face height; 5 lower anterior face height; 6, total anterior face height. the anterior inferior outline of sella turcica and the anterior contour of the middle cranial fossa (De Coster’s line), including the greater wings of the sphenoid, cribriform plate, the orbital roof, and the inner surface of the frontal bone. This superimposition was used to transfer the Frankfort plane from 1 cephalogram to the other. Maxillary superimposition was patterned after Doppel et al.8 It is achieved by superimposing on the posterior border of the zygomatic processes. Vertically, the floor of the orbit was raised 1.5 mm for each millimeter the palatal plane is lowered. 50 Al-Buraiki, Sadowsky, and Schneider Fig 2. Variables measured on maxillary superimposition (solid line, T1; broken line, T2). 1, ⌬ U1 angle; 2, ⌬ U1 vertical; 3, ⌬ U6 vertical; 4, maxillary rotation. Mandibular superimposition was patterned after Bjork’s structural method, in which the tip of the chin, the inner cortical plate and trabecular pattern of the symphysis, the mandibular canal, or the lower contour of the molar germ of the second or third molar before root formation are superimposed.9 On the maxillary and mandibular superimposition, the following variables were measured (Figs 2 and 3): 1. Change in the angulation of incisors: angle formed between long axes of the 2 maxillary and 2 mandibular incisors. A negative value indicates incisor uprighting. 2. Change in the vertical position of incisors: vertical distance between 2 points located 17 mm apical to the incisal edge of each incisor (approximating the center of resistance). 3. Change in the vertical position of molars: measured at the mesiobuccal cusp. 4. Maxillary and mandibular rotation: the angle formed by the two Frankfort horizontal lines. A negative value indicates an opening (clockwise) rotation. To test intraoperator reliability for the angular and linear measurements, 20 radiographs (10 patients) were selected at random from the original sample. These radiographs were retraced and remeasured, with the 2 measurements at least 4 weeks apart. The data obtained from the repeated measurements were statistically com- American Journal of Orthodontics and Dentofacial Orthopedics January 2005 Fig 3. Variables measured on mandibular superimposition (solid line, T1; broken line, T2). 1, ⌬ L1 angle; 2, ⌬ L1 vertical; 3, ⌬ L6 vertical; 4, mandibular rotation. pared with the original measurement with a singlesample paired t test. An independent t test was used to determine the differences between the treated and untreated groups at T1. For the variables measured on the individual cephalograms (T1, T2, and T3), a paired t test was used to assess treatment and posttreatment changes. For the variables derived from the superimposition, changes were measured rather than absolute values; treatment and posttreatment changes were tested with a singlesample t test. An independent t test was used to compare T2-T1 changes between the treated and untreated groups. Difference were considered statistically significant at P ⬍ .01. RESULTS Intraoperator reliability was examined with the paired t test. There were no statistically significant differences between the measurements from the original tracings and those repeated at a later date. (Table IV). Table V summarizes the pretreatment measurements for the treated group as compared with the untreated group at T1. The treated group had a mean ANB angle of 5.9° with an increased overjet and overbite (6.2 mm and 5.9 mm, respectively). The mandibular plane, Y-axis, and lower anterior face height ratio seem to be within normal limits. Independent sample t test revealed no statistically significant differences between the 2 groups in all variables except for the anterior face height measurement. Although the Al-Buraiki, Sadowsky, and Schneider 51 American Journal of Orthodontics and Dentofacial Orthopedics Volume 127, Number 1 Table IV. Paired t test of repeated measurements Variables ANB (°) Mandibular plane (°) Y-Axis (°) Upper anterior face height (mm) Lower anterior face height (mm) Total anterior face height (mm) Overjet (mm) Overbite (mm) Interincisal angle (°) ⌬ L1 angle (°) ⌬ L1 vertical (mm) ⌬ L6 vertical (mm) Mandibular rotation (°) ⌬ U1 angle (°) ⌬ U1 vertical (mm) ⌬ U6 vertical (mm) Maxillary rotation (°) Mean difference ⫾ SD P value 0.2 ⫾ 0.5 0.0 ⫾ 1.4 ⫺0.3 ⫾ 1.2 0.1 ⫾ 1 0.7 ⫾ 3.3 0.4 ⫾ 1.1 0.1 ⫾ 0.6 0.0 ⫾ 0.5 0.2 ⫾ 2.8 0.5 ⫾ 2.4 0.2 ⫾ 0.7 0.1 ⫾ 0.9 0.3 ⫾ 1.3 0.6 ⫾ 1.5 0.1 ⫾ 0.6 0.2 ⫾ 0.9 0.2 ⫾ 1.2 .3 1.0 .4 .8 .5 .3 .8 1.0 .9 .6 .5 .9 .5 .3 .8 .6 .6 upper, lower, and total anterior face heights were statistically different, there was no statistically significant difference in lower anterior face height ratio between the treated and untreated groups. Treatment changes The ANB angle was reduced by 2.6°, and the mandibular plane and Y-axis increased by 2.1° and 2°, respectively. All anterior face height measurements increased without a change in the anterior face height ratio. The overjet and overbite were reduced by 4.1 mm and 4 mm, respectively, whereas the interincisal angle remained unchanged. There were no statistically significant changes in the angulation of maxillary and mandibular incisors and the vertical position of maxillary incisors. Maxillary molars, mandibular molars, and mandibular incisors moved occlusally. The maxilla and mandible rotated clockwise 1.4° and 1.6°, respectively (Table VI). Mean differences between the treated and untreated groups In the treated group, T2-T1 change represents the net effect of treatment and growth, whereas in the untreated group it represents growth alone. The changes reported below are mean differences between the two groups (Table VI). Treatment reduced the ANB angle by 2.5° and increased the mandibular plane and Y-axis angles by 3.1° and 2.1°, respectively. There was an increase in all anterior face height measurements, with no change in the lower anterior face height ratio. The overjet and overbite decreased by 4.1 mm and 3.9 mm, respectively. The change in the interincisal angle was not statistically different between the 2 groups. Maxillary and mandibular superimposition showed that the mean difference between the treated and untreated groups was statistically significant for the maxillary and mandibular rotation and changes in the vertical position of both the maxillary incisors and molars. The maxilla and mandible rotated clockwise 1.6° and 2.9°, respectively. Maxillary incisors were relatively intruded 1.5 mm, and maxillary molars were extruded 2.3 mm. It is interesting to note that the vertical changes of the mandibular incisors and molars were not statistically different between the 2 groups. Posttreatment changes The ANB and mandibular plane angle decreased by 0.8° ⫾ 1.2° and 2° ⫾ 3°, respectively. All anterior face height measurements increased, with no change in the lower anterior face height ratio. There was a statistically significant increase, albeit small, in both overjet (0.7 ⫾ 0.8 mm) and overbite (0.7 ⫾ 1.1 mm). The interincisal angle showed no change (Table VII). Maxillary and mandibular superimposition revealed a statistically significant change in mandibular rotation as well as in the vertical position of incisors and molars, both maxillary and mandibular (Table VIII). The mandible rotated 2.4° ⫾ 2.3° counterclockwise, maxillary incisors erupted 1.9 ⫾ 1.5 mm, and maxillary molars erupted 1.4 ⫾ 1.2 mm. The mandibular incisors erupted 1.6 ⫾ 1.6 mm, whereas the molars erupted 2.1 ⫾ 2.1 mm. Measuring mean differences between the treated and untreated groups was not feasible, owing to the lack of T3 data for the untreated group. DISCUSSION Study design This was a retrospective study with inherent limitations. To minimize selection bias, the sample was identified by a member of the auxiliary staff in the office to satisfy the selection criteria set by the investigator. The untreated group was age- and sex-matched to the treated group. In addition, there was no statistically significant difference in pretreatment variables in the treated and untreated groups except for anterior face height measurements, which was more likely due to a difference in magnification (as will be discussed in the following section). Yet, equivalence between the two groups cannot be assured because of the retrospective nature of the study. Material and method The treated sample consisted of 25 subjects. The treatment was initiated in the late mixed or early permanent dentition just before the pubertal spurt, to 52 Al-Buraiki, Sadowsky, and Schneider Table V. American Journal of Orthodontics and Dentofacial Orthopedics January 2005 Comparison between treated and untreated groups at T1 Variables ANB (°) Mandibular plane (°) Y-axis (°) Upper anterior face height (mm) Lower anterior face height (mm) Total anterior face height (mm) Lower anterior face height ratio Overjet (mm) Overbite (mm) Interincisal angle (°) Treated (mean ⫾ SD) Untreated (mean ⫾ SD) Mean difference 5.9 ⫾ 1.87 23.1 ⫾ 4.1 57.5 ⫾ 3.0 53.1 ⫾ 2.9 63.8 ⫾ 4.8 117.3 ⫾ 5.8 54.4 ⫾ 2.5 6.2 ⫾ 2.3 5.9 ⫾ 1.2 128.8 ⫾ 11.8 5.7 ⫾ 1.6 23.6 ⫾ 3.2 59.1 ⫾ 2.3 50.6 ⫾ 2.9 59.5 ⫾ 3.5 110.1 ⫾ 5.3 53.9 ⫾ 1.4 5.2 ⫾ 2.1 5.7 ⫾ 1.9 130.4 ⫾ 9.4 0.2 ⫺0.5 ⫺1.6 2.5* 4.3* 7.2* 0.5 1 0.2 ⫺1.6 *P ⬍ .01. Table VI. T2-T1 changes in treated and untreated groups Variables Treated T2-T1 (mean ⫾ SD) Untreated T2-T1 (mean ⫾ SD) Mean difference ANB (°) Mandibular plane (°) Y-axis (°) Upper anterior face height (mm) Lower anterior face height (mm) Total anterior face height (mm) Lower anterior face ratio (mm) Overjet (mm) Overbite (mm) Interincisal angle (°) ⌬ L1 angle (°) ⌬ L1 vertical (mm) ⌬ L6 vertical (mm) Mandibular rotation (°) ⌬ U1 angle (°) ⌬ U1 vertical (mm) ⌬ U6 vertical (mm) Maxillary rotation (°) ⫺2.6 ⫾ 1.8* 2.1 ⫾ 2.4* 2.0 ⫾ 2.0* 4.0 ⫾ 2.6* 5.5 ⫾ 2.7* 9.1 ⫾ 4.7* 0.4 ⫾ 1.1 ⫺4.1 ⫾ 3.1* ⫺4.0 ⫾ 1.2* ⫺0.5 ⫾ 14.1 ⫺1.4 ⫾ 6.4 1.5 ⫾ 1.6* 1.6 ⫾ 1.1* ⫺1.6 ⫾ 2.3* 1.0 ⫾ 10.2 0.1 ⫾ 1.5 4.1 ⫾ 1.9* ⫺1.4 ⫾ 1.4* ⫺0.1 ⫾ 1.0 ⫺1 ⫾ 2.1 ⫺0.1 ⫾ 1.4 2.2 ⫾ 2.1 3.1 ⫾ 3.1 5.3 ⫾ 3.8 0.3 ⫾ 1.8 0 ⫾ 0.9 ⫺0.1 ⫾ 1.4 ⫺1.4 ⫾ 6.0 1.4 ⫾ 2.6 1.9 ⫾ 1.3 1.9 ⫾ 1.4 1.3 ⫾ 1.8 0.1 ⫾ 2.3 1.6 ⫾ 0.9 1.8 ⫾ 1.0 0.2 ⫾ 1.0 ⫺2.5* 3.1* 2.1* 1.9* 2.4* 3.8* 0.1 ⫺4.1* ⫺3.9* 0.9 ⫺2.8 ⫺0.3 ⫺0.3 ⫺2.9* 0.9 ⫺1.5* 2.3* ⫺1.6* *P ⬍ .01. Table VII. Paired t test of posttreatment changes Variables ANB (°) Mandibular plane (°) Y-axis (°) Upper anterior face height (mm) Lower anterior face height (mm) Total anterior face height (mm) Lower anterior face height ratio Overjet (mm) Overbite (mm) Interincisal angle (°) *P ⬍ .01. T2 (mean ⫾ SD) T3 (mean ⫾ SD) 3.3 ⫾ 1.4 25.2 ⫾ 4.5 59.5 ⫾ 3.0 57.1 ⫾ 2.7 69.2 ⫾ 5.3 126.4 ⫾ 6.6 54.7 ⫾ 1.9 2.2 ⫾ 0.6 1.9 ⫾ 0.8 128.3 ⫾ 8.6 2.5 ⫾ 1.9 23.2 ⫾ 4.5 59.0 ⫾ 3.8 58.6 ⫾ 3.0 72.1 ⫾ 6.6 130.7 ⫾ 7.5 55.1 ⫾ 2.4 2.9 ⫾ 0.8 2.6 ⫾ 1.3 127.4 ⫾ 7.0 Difference ⫺0.8 ⫾ 1.2* ⫺2 ⫾ 3.0* ⫺0.5 ⫾ 2.5 1.5 ⫾ 1.4* 2.9 ⫾ 3.2* 4.3 ⫾ 3.7* 0.3 ⫾ 1.1 0.7 ⫾ 0.8* 0.7 ⫾ 1.1* ⫺0.9 ⫾ 7.8 American Journal of Orthodontics and Dentofacial Orthopedics Volume 127, Number 1 Table VIII. One-sample t test of posttreatment changes (superimposition) Variables ⌬ L1 angle (°) ⌬ L1 vertical (mm) ⌬ L6 vertical (mm) Mandibular rotation (°) ⌬ U1 angle (°) ⌬ U1 vertical (mm) ⌬ U6 vertical (mm) Maxillary rotation (°) T3-T2 (mean ⫾ SD) 1.4 ⫾ 3.9 1.6 ⫾ 1.6* 2.1 ⫾ 2.1* 2.4 ⫾ 2.3* 1.5 ⫾ 6.0 1.9 ⫾ 1.5* 1.4 ⫾ 1.2* 0.5 ⫾ 1.4 *P ⬍ .01. take advantage of growth. The limited sample size was the result of 3 factors. The first was that the practitioner retains for a very long period of time, which makes obtaining a T3 cephalogram several years postretention very difficult. Only 3 patients had T3 cephalograms 1 year after mandibular retainer removal (maxillary retention is usually discontinued several years before mandibular); the others ranged between 1.7 and 18.3 years (the majority in the 2-5-year range). The second factor was that the T2 cephalogram must have been taken no later than 3 months from appliance removal. The third factor was that patients for whom premolars were bonded, even if it was done toward the end of treatment, were excluded from the study to ensure that active premolar extrusion was not part of the leveling process. The untreated group was sex- and age-matched at both T1 and T2 (Table III). There was no statistically significant difference between the two groups in all pretreatment variables except for anterior face height measurements, which were slightly greater in the treated than in the untreated group. The lower anterior face height ratio was the same in both groups, and thus the differences in anterior face height measurements were more likely than not due to difference in magnification. This, however, should have little or no effect on the findings of this study. The linear measurements examined in this study were changes in anterior face height measurements (rather than the actual value at T1, T2, and T3), overjet, and overbite. Because these measurements were small in magnitude, the effect of magnification was considered negligible. For example, a 10% difference in magnification would theoretically affect changes in overbite and overjet by 0.4 mm (mean changes were 4 mm in the untreated group). Al-Buraiki, Sadowsky, and Schneider 53 Effectiveness of treatment mechanics The results of this study show that incisor intrusion mechanics used in the treated sample are effective in the correction of overbite. The mean correction was 4 mm, 68% of the pretreatment overbite. Samples from different studies exhibit different pretreatment overbite. As a result, it seems reasonable to examine the percentage of the correction (amount of correction relative to the pretreatment overbite) rather than the actual value. The amount of overbite correction reported in this study seems greater than reported in previous studies.4-6 In those studies, the amount of correction ranged from 1.5 mm to 2.7 mm, and the correction percentage ranged from 34% to 58% (Table I). However, the difference could be due to the deeper pretreatment overbite found in our sample. The closest posttreatment overbite reported in the literature is 2.1 mm, with a pretreatment overbite of 4.8 mm (compared with 5.9 mm reported in this study). The treatment resulted in both skeletal and dental changes. The skeletal changes included opening rotation of the mandible, evident in the superimposition as well as the increase in Y-axis and mandibular plane angle, all of a similar magnitude. It also included an increase in all anterior face height measurements. There was a proportionate increase in upper and lower anterior face heights, thus maintaining the lower anterior face height ratio. In the treated group, both mandibular incisors and molars moved occlusally a similar amount (1.5 mm and 1.6 mm, respectively). The mean differences between the treated and untreated groups in the present study were not statistically significant; that is to say, the treatment had no effect on the mandibular dentition. The absence of mandibular incisor intrusion could be partly explained by the use of class III elastics—16 patients that were initially treated with tandem mechanics—which might have counteracted the effect of the lever arches on the mandibular incisors. Other studies have shown more mandibular molar movement than that reported in this study, with similar amounts of change for the mandibular incisors.4,10,11 The reports in the literature suggest that some leveling took place by extrusion of the mandibular buccal segments contrary to the findings in the present study. In the treated group, maxillary incisors maintained their vertical position while erupting 1.6 mm in the untreated group (relative intrusion), and the maxillary molars extruded 4.1 mm while erupting 1.8 mm in the untreated group. Previous studies reported similar changes in maxillary incisors and molars during treatment.4,5,10,11 54 Al-Buraiki, Sadowsky, and Schneider The relative intrusion of maxillary incisors coupled with the vertical occlusal movement of the molars decreases the amount of incisor overlap and thus was responsible for the overbite correction. The extrusion of the molars (maxillary molars moved more occlusally in the treated than in the untreated group) can result in 1 of 2 effects, opening rotation of the mandible or increasing the vertical development of the mandible. In spite of its small magnitude, opening rotation of the mandible is evident from the results of this study. In absence of posterior face height measurement, the effect of molar extrusion on posterior vertical development of the mandible cannot be examined. Stability of overbite correction Although statistically significant, the increase in overbite during the posttreatment period was small (0.7 mm at 17%) and is clinically insignificant. The posttreatment increase in overbite could be relapse or part of the normal development. Unfortunately, a matching group for the period T3-T2 was not available to help answer this question. Driscoll-Gilliland et al12 evaluated growth and stability in untreated and treated subjects. The untreated group had a similar age distribution (T2-T1) to that of the untreated group in this study (T3-T2). In their untreated sample, the overbite remained unchanged, as it did in the T2-T1 period in the untreated sample in our study. This suggests that the 0.7 mm of posttreatment increase in overbite reported in our treated sample is relapse rather than normal development. The amount of relapse reported in this study is similar to amounts in previous reports.1,2,4-6 However, the percentage of relapse (17%) seems to be slightly lower compared with previous reports (23%-60%). The difference was small, and statistical testing was not feasible. When the net correction (T3-T1) is evaluated, the difference becomes more apparent. The mean net change in overbite reported in this study was 3.3 mm, compared with a range of 0.6 mm to 1.9 mm reported in previous studies. There was no change in the Y-axis in the posttreatment period. This indicates that the opening rotation of the mandible that occurred during treatment was not recovered in the posttreatment period. The reduction in mandibular plane angle and counterclockwise rotation of the mandible (2° and 2.4°, respectively) could be due to either an increase in the posterior vertical development of the mandible or significant bone apposition on the posterior part of the inferior border of the mandible (remodeling). It is interesting to note that the untreated American Journal of Orthodontics and Dentofacial Orthopedics January 2005 group in the Driscoll-Gilliland study12 showed no change in mandibular rotation. During the posttreatment period, there was also slightly more eruption of the maxillary incisors than of the maxillary molars. The eruption of the maxillary incisors might have contributed to the small amount of overbite increase reported in this study. In the mandible, there was slightly more eruption of the molars than the incisors. The amount of mandibular incisor eruption was similar to that reported by Driscoll-Gilliland et al.12 The differential eruption between mandibular incisors and molars could be due to the incorporation of anterior bite plane in the maxillary retainer, holding the incisors while allowing some eruptions of mandibular molars. The postretention time is an important variable in any study that involves the stability of orthodontic correction. One might expect an increase in the amount of relapse with the increase in the postretention duration. However, the postretention period reported in this study (7.3 ⫾ 4.3 years after maxillary retention and 4.3 ⫾ 3.9 years after the discontinuation of mandibular retention) is long enough to show most if not all the relapse expected to occur posttreatment, given the long retention duration, with growth being completed long before the T3 records were taken. The relative stability of overbite correction (small magnitude of change) reported in this sample can be attributed to several factors. The long retention period and the retainer design are important. The relative stability of overjet reported in this study might have played a role in overbite stability as well. Also, the effectiveness of the mechanics allowed overcorrection, which might or might not have contributed to the relative stability of overbite correction. The reader should be reminded that the current study excluded subjects with Class II, Division 2 malocclusions, who might exhibit a higher overbite relapse. Whether incisor intrusion mechanics produce a more stable overbite correction than the other methods of leveling is a question yet to be answered. It will require a comparison between matching samples treated with different mechanics as compared with the mechanics used in this study. CONCLUSIONS Results from this study revealed that the mechanics implemented were effective in overbite correction. Posttreatment changes revealed a small increase in overbite and overjet that was considered clinically insignificant. A postretention overbite of 2.6 mm is American Journal of Orthodontics and Dentofacial Orthopedics Volume 127, Number 1 an excellent clinical achievement, and a net overbite correction (T3-T1) of 3.3 mm seems to be greater than in previous reports. REFERENCES 1. Bishara S, Chadha J, Potter R. Stability of intercanine width, overbite, and overjet correction. Am J Orthod 1973;63:588-95. 2. Hellekant M, Lagerstrom L, Gleerup A. Overbite and overjet correction in Class II, Division 1 sample treated with Edgewise therapy. Eur J Orthod 1989;11:91-106. 3. Uhde MH, Sadowsky C, BeGole EA. Long term stability of dental relationships after orthodontic treatment. Angle Orthod 1983;53:240-52. 4. Sadowsky C, Schneider B, Begole EA, Tahir B. Long-term stability after orthodontic treatment with prolonged retention. Am J Orthod Dentofacial Orthop 1994;106:243-9. 5. Fidler BC, Artun J, Joondeph DR, Little RM. Long term stability of Angle Class II Division 1 malocclusion with successful occlusal results at end of active treatment. Am J Orthod Dentofacial Orthop 1995;107:267-85. Al-Buraiki, Sadowsky, and Schneider 55 6. Carcara S, Preston B, Jureyda O. The relationship between the curve of Spee, relapse, and the Alexander Discipline. Semin Orthod 2001;7:90-9. 7. Bjork A, Skieller V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod 1983; 5:1-46. 8. Doppel DM, Ward MD, Joondeph DR, Little R. An investigation of maxillary superimposition technique using metallic implants. Am J Orthod Dentofacial Orthop 1994;105:161-8. 9. Bjork A. Prediction of mandibular growth rotation. Am J Orthod 1969;55:585-99. 10. Elms TN, Buschang PH, Alexander RG. Long-term stability of Class II, Division 1, nonextraction cervical face-bow therapy: II. Cephalometric analysis. Am J Orthod Dentofacial Orthop 1996; 109:386-92. 11. Bernstein RI. Leveling the curve of Spee with a continuous archwire technique: a long-term cephalometric analysis [thesis]. Buffalo NY: University of Buffalo; 1999. 12. Driscoll-Gilliland J, Buschang P, Behrents R. An evaluation of growth and stability in untreated and treated subjects. Am J Orthod Dentofacial Orthop 2001;120:588-97.