Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
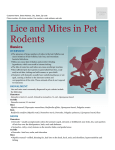
Mangy Mutts: Diagnosis and Treatment of Common Mites in Dogs and Cats Joya Griffin, DVM, DACVD Animal Dermatology Clinic: Louisville and Lexington, KY Canine Demodicosis Demodex mites are a follicular mites that is part of the dog’s normal cutaneous microfauna. They are transmitted from the bitch to the puppies during nursing. Dogs born via c-section do not have any Demodex mites. A defect in the immune system of the skin or immunosuppression allows the mites to proliferate in hair follicles. D. canis is the most common type of Demodex mite, however, several morphologically different types of mites have been reported. The long-bodied mite, D. injae, is often found on dogs with a greasy/oily skin and hair coat and is associated with a pruritic dermatitis over the dorsal midline and sebaceous gland hyperplasia. Terrier breeds are overrepresented. D. injai has also been found within otic secretions. The short-bodied mite, D. cornei, has been found in association with D. canis. Recent DNA sequencing indicates that this short-bodied is a morphologic variant of D. canis and is not a separate species as D. injae is thought to be. Regardless of the type of Demodex mites found in dogs, similar efficacy is seen with treatment. Juvenile-onset demodicosis is often seen in young dogs who have been afflicted by endoparasitism, malnutrition and debilitation. This form is likely genetically based due to strong breed predispositions. Dogs with juvenile-onset demodicosis should not be bred. Immunosuppression caused by chemotherapy, neoplasia, hypothyroidism, or hyperadrenocorticism predisposes adult dogs to demodicosis. A direct cause-and-effect relationship with demodicosis is inapparent as many immunosuppressed animals do not develop demodicosis. Clinical disease is divided into localized and generalized forms. Localized forms, no more than four lesions up to 2.5 cm each, do not warrant treatment and spontaneously resolve. Generalized disease can be severe with few cases spontaneously curing. Clinical signs include mild erythema, comedones and scaling and can progress to partial or complete alopecia with follicular papules, pustules and furunculosis. In severe cases crusting, exudation, focal ulceration, and draining tracts may be seen. Lesions generally start on the face and progress to the limbs and then to other parts of the body. Fever, lethargy and lymphadenopathy can be present with generalized disease. Pedal demodicosis can cause severe interdigital swelling and can be painful especially in large breeds. Diagnosis of demodicosis is most commonly done via deep skin scrapes where capillary oozing is achieved. Gentle clipping in longer haired breeds should be done. The skin should be squeezed during or in between scraping to extrude the mites deep within the hair follicles. Best yield is achieved by scraping primary lesions such as papules and pustules. Ulcerated areas should be avoided. Even though, Demodex mites are a part of the normal microfauna, it is very uncommon to find even one mite on deep skin scrape. If one mite is found on a single skin scrape, numerous additional scrapes should be done as it is very rare to find even 1 Demodex mite in normal dogs. The number and life stage of the mites should be recorded and the site they were obtained from so that these same sites can be surveyed throughout treatment. Trichograms are a useful technique for areas that cannot be scraped like the face, periocular region and paws; however, a negative skin scrape does not rule out demodicosis and negative trichograms should be followed by deep skin scrapes. Fifty to 100 hairs should be pulled in the direction of hair growth and placed in mineral oil on a slide and covered with a cover slip. Skin biopsy can be done in instances where skin scrape and trichogram are negative and the index of suspicion for demodicosis is high. This may be necessary on the paws and in the Sharpei breed. Direct examination of cytology from very exudative lesions can also yield Demodex mites. Mites can also be found on fine-needle aspirates of lymph nodes. Secondary bacterial infections should be identified and treated. Gram-negative infections are common with pedal demodicosis with associated furunculosis. Treat mild, localized disease with weekly chlorhexidine or benzoyl peroxide baths and monitor for progression of lesions. Generalized demodex cases should be bathed once to twice weekly with the aforementioned shampoos. The following treatment options are available: 1. 0.025- 0.06% Amitraz dips weekly or every 2 weeks. Medium to long-haired dogs should be clipped and skin should remain dry between dips. 2. Milbemycin oxime once daily at 1-2 mg/kg. 3. Moxidectin as spot-on (Advantage Multi®) weekly. Note: This treatment option works better in dogs with mild disease. 4. Ivermectin at 0.3- 0.6 mg/kg or moxidectin at 0.2- 0.5 mg/kg by mouth once daily. In sensitive breeds, an initial dose of 0.05 mg/kg increasing every few days to the therapeutic dose is recommended. Monitor for neurologic side effects. Dogs should be evaluated monthly and treated beyond a negative skin scrape is achieved (no mites or dead mites skeletons on cytology of exudates). Predisposing factors of demodicosis should be identified and treated to maximize response to therapy. Long-term glucocorticoid therapy should be avoided during treatment and in dogs with a history of demodicosis. Close monitoring for recurrence of disease should be done for the first 12 months after remission. Some adult-onset cases cannot be cured and remain on some form of therapy for life. Feline Demodicosis Cats can be afflicted by two species of Demodex mites, Demodex cati and Demodex gatoi as well as a third unnamed morphologic variant. D. cati are part of the normal fauna residing within hair follicles and sebaceous glands of cats and are analogous to D. canis in the canine counterpart. Demodex cati is associated with systemic disease and a compromised immune system. D. gatoi, on the other hand, is a contagious, superficial mites that causes extreme pruritus in otherwise normal cats. Demodex cati associated with lesions of alopecia, comedones, crusts, papules, seborrhea, military dermatitis, erosions and ulceration. Pruritus is variable. If lesions are localized they are generally on the face. D. cati can also cause ceruminous otitis alone or in conjunction with skin lesions. Mites are diagnosed based on deep skin scraping, trichogram or biopsy. Patients should be screened for retroviral infection and systemic or infectious diseases. Treat with oral ivermectin 0.3 mg/kg SID or every other day or 0.0125% amitraz dips weekly (should only be used if there is treatment failure with ivermectin due to the potential for toxicity). Diagnosis of Demodex gatoi requires finding the mite on trichogram, superficial skin scrape or fecal floatation. Due to the small number of mites normally present and the grooming behavior of cats, actually identifying the mites is difficult. The best areas to scrape are non-alopecic areas where the cat would have difficulty reaching. A “response to treatment trial” is the common method of diagnosis. Treatment of choice requires weekly dipping with 2% lime sulfur for a minimum of 6 weeks. Some have found treatment with daily or every other day oral ivermectin at 0.3 mg/kg to be successful. Treatment failures have been seen. All cats in the household, even asymptomatic individuals, should be treated. Studies are currently looking at the development of a molecular diagnostic method to diagnose Demodex gatoi in cats. Recent DNA sequencing confirmed two species of Demodex with D. cati resembling D. canis in dogs and D. gatoi resembling D. brevis, the facial mites of humans that reside in sebaceous glands. Sarcoptes Sarcoptes scabiei var. canis is a contagious and zoonotic mite that causes intense pruritus in hypersensitive dogs. The pattern of distribution affects sparsely haired areas such as the elbows, hocks and ear margins. It can spread to the ventrum and face and usually is represented by intense erythema as the primary lesion. Secondarily, excoriations, scaling, lichenification, hyperpigmentation and secondary infections occur. Most infected dogs itch a few days after being infected by scabies mites but have mild symptoms. Three to four months later, intense pruritus develops. A positive pinnal-pedal response is present in most affected individuals. Diagnosis is done via demonstrating the mites on superficial skin scrapes. The mite is difficult to find due to small numbers of mites on the infected patient. A response to treatment is the most common diagnostic method. Treatment with weekly lime sulfur dips, weekly oral ivermectin, bimonthly subcutaneous ivermectin, and topical AdvantageMulti® or Revolution® every two weeks for 4-6 weeks to stop the life cycle of the mite which is 10-21 days. All in-contact animals should be treated even if asymptomatic. Environmental decontamination is not necessary. Notoedres Notoedres cati, also referred to as feline scabies, is associated with pruritus, scaling and crusting of the head and face. Mites are recovered on superficial skin scrapes and the mites can be easily spread to all in-contact animals and humans. Treatment is like that of scabies. Otodectes Otodectes cynotis is a contagious mite that has a 3 week life cycle. The mite infects the vertical and horizontal ear canals of dogs and cats. The mite feeds on surface keratin and can cause irritation and local trauma. Animals with mite produce copious amounts of sebum that is dark in color due to blood and ear mite feces and causes an occlusive otitis externa. The mites can spread to the face, back claws and face due to scratching. Milliary dermatitis can occur in cats. Diagnosis is based on identifying the mites in otic debris in mineral oil. Many licensed topical therapies are available. Systemic therapy with ivermectin or topical miticides is also effective. All in-contact animals should be treated and the environment cleaned as the mite can live off of the host for several weeks. References 1. Muellar, RS, et al. Treatment of demodicosis in dogs: 2011 clinical practice guidelines. Vet Derm, 23; 86- 96. 2. Ordeix, L, et al. Demodex injai infestation and dorsal greasy skin and hair in eight wirehaired fox terrier dogs. Vet Derm, 20; 267-272. 3. Milosevic, MA, et al. PCR amplification and DNA sequencing of Demodex injai from otic secretions of a dog. Vet Derm, 24, 286-288. 4. Ravera, I, et al. Small Demodex populations colonize most parts of skin of healthy dogs. Vet Derm, 24, 168- 172. 5. Fondati, A, et al. Prevalence of Demodex canis-positive healthy dogs at trichoscopic examination. Vet. Derm, 21, 146-151. 6. Frank, LA, et al. A molecular technique for the detection and differentiation of Demodex mites on cats. Vet Derm, 24, 367-369. 7. Beale, K. Feline demodicosis: a consideration in the itchy or overgrooming cat. J Feline Med Surg, 14 (3), 209-213. 8. Campbell, KL. Small Animal Dermatology Secrets. Hanley and Belfus, 2004. 9. Terada, Y. Sarcoptes scabiei var. canis refractory to ivermectin treatment in two dogs. Vet Derm. 21, 608-612. 10. Curtis, C. Current trends in the treatment of Sarcoptes, Cheyletiella and Otodectes mite infestations in dogs and cats. Vet Derm. 15, 108-114.