Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
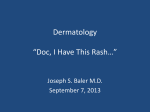
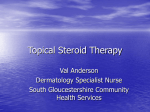
Perioral dermatitis mostly targets women This inflammatory skin disorder may have a hormonal cause and can often be linked to topical steroids, writes Johnny Loughnane Forum Dermatology Perioral dermatitis – note spread to lower eyelid Perioral dermatitis following use of clobetasone . Note more inflammatory rash when steroids have been used PERIORAL DERMATITIS is an inflammatory skin disorder, particularly common in women between the ages of 20 and 40. The cause is not known, although the female predominance may point to hormonal factors. Many patients have used topical steroids. It presents with papules, scaly erythema and, rarely, pustules. The absence of open and closed comedones helps distinguish it from acne. The rash is distributed around the mouth with sparing of the skin immediately adjacent to the lips. The nasolabial fold and lower eyelid are often involved. Rarely, the upper eyelids are involved. If topical steroids have been applied, the rash becomes more florid, with the papules a deeper red and scaly erythema more prominent. Keep in mind that it may present with periocular involvement alone. It is rare in males and one should always suspect steroid use, which must be enquired into. Often the steroid has been applied to an area of seborrhoeic dermatitis. While potent and very potent steroids are the usual culprits, it can also occur with moderately potent steroids. A feeling of slight itch or stinging is usual and some patients complain of a tight feeling in the areas involved. If steroids have been applied, this feeling of tightness may worsen for a while following steroid withdrawal. It is important to warn patients about this. Topical steroids tend to relieve this feeling, so the patient may be tempted to reuse them. Advise patients to use a moisturiser instead. If there is an unacceptable flare on stopping a potent steroid, one may wean the patient off steroids – first using Perioral dermatitis with sparing of skin immediately adjacent to lips clobetasone (Eumovate) for five days before replacing it with hydrocortisone for a further five days. All steroids must then be stopped. When the perioral dermatitis is cleared it may be evident that the patient had seborrhoeic dermatitis. They usually do well on hydrocortisone – antifungal combination cream, eg. Daktacort. Hydrocortisone does not seem to cause or exacerbate perioral dermatitis. Treatment with oral tetracycline is very effective. Usually, a four week course is all that is needed. If steroids have been applied, response is slower and an eight week course may be needed. Oxytetracycline 250mg-500mg twice daily is the standard tetracycline. Lymecycline (Tetralysal) 300mg once daily, may be a better option as its absorption is not so much reduced by food and once daily dosage may be more convenient. While treatment is almost always effective, there is a risk of recurrence. If there is frequent recurrence, one tablet of lymecycline taken once weekly should be considered. Many patients will be taking the combined oral contraceptive. Evidence suggests that adding tetracyclines does not reduce the contraceptive effect. However, standard advice remains that patients should take extra contraceptive precautions for the first two weeks of tetracycline use. Tetracycline is contraindicated in children under 12 and in pregnancy–here topical erythromycin is an option. Johnny Loughnane is in practice in Co Limerick FORUM May 2005 57