Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
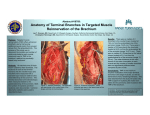
Eur J Orthop Surg Traumatol DOI 10.1007/s00590-013-1181-6 UP-TO DATE REVIEW AND CASE REPORT Stress injury of the acromion: case report and literature review Atul Kumar Taneja • Francisco Pires Negromonte Abdalla Skaf • Received: 29 December 2012 / Accepted: 27 January 2013 Ó Springer-Verlag France 2013 Abstract We report a case of stress injury of the acromion related to golf practicing in a 40-year-old male. Fractures of the scapula are unusual, with stress injury of the acromion being even rarer. The probable mechanism would be a strong contraction of posterior fibers of the deltoid during golf swing. There are few published reports of similar injuries, and to our knowledge, this is the first to demonstrate its features by magnetic resonance imaging. A review of the literature is also presented. Keywords Stress fracture Acromion Shoulder Golf Magnetic resonance imaging plain radiographs and healed with conservative treatment. We report a case of stress injury of the acromion related to golf practicing in a 40-year-old male diagnosed by magnetic resonance imaging (MRI). Golf may be a demanding sport, and the mechanism suggested would be a strong contraction of posterior fibers of the deltoid during the swing forward to strike the ball [7]. MRI is especially helpful in stress injuries and non-displaced fractures. Therefore, early recognition by radiologists and orthopedics surgeons is of utmost importance to prevent causative activity and perform adequate treatment regimen. Case report Introduction Injuries of the acromion may result from multiple mechanisms, with only few cases of stress injuries being reported so far [1–6]. Most cases of stress injuries of the acromion published were minimally displaced fractures diagnosed by A. K. Taneja F. P. Negromonte A. Skaf Departamento de Radiologia Musculoesquelética, Hospital do Coração (HCor) and Teleimagem, São Paulo, Brazil A. K. Taneja Musculoskeletal Imaging and Intervention Division, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA A. K. Taneja (&) Teleimagem, R. Des. Eliseu Guilherme, N. 53, 7. Andar, São Paulo, SP 04004-030, Brazil e-mail: [email protected] A. Skaf Alta Diagnósticos, São Paulo, Brazil A 40-year-old right-handed man presented with history of pain on his right shoulder that begun while playing amateur golf 1 month earlier. Just before he hit the ball off the tee, he felt a sudden pain on the posterior and superior aspect of the shoulder. He felt pain in non-specific movements while he continued to play during that day and the following few days, even after starting taking oral painkillers during a total of 5 days. Neither other injuries nor other sports activities were reported in the following weeks after the golf play. He was otherwise healthy, without any history of serious musculoskeletal injury, systemic disease, or bone disorder. Clinical examination revealed mild swelling and focal tenderness over superior and posterior region of the right shoulder. There was complete range of motion. Plain radiographs of the shoulder were performed at another institution and reported to be normal. MRI scan of the right shoulder was performed at our facility using the following pulse sequences: axial proton density (PD)weighted fat-suppressed [TR/TE = 2,870/37; number of excitations (NEX) = 2; slice thickness = 3.0 mm; 123 Eur J Orthop Surg Traumatol matrix = 320 9 320], coronal T2-weighted fat-suppressed (2,200/42; 1; 3.5 mm; 256 9 256), sagittal T2-weighted fat-suppressed (2,570/46; 2; 4.0 mm; 320 9 320), sagittal PD-weighted (1,500/23; 2; 4.0 mm; 384 9 384), and coronal T1-weighted (400/11; NEX 1; 3.5 mm; 384 9 384). MRI revealed extensive bone marrow edema of the acromion, represented by increased signal intensity (SI) on T2-weighted fat-suppressed images (Fig. 1). Also, a marked hypointense thin line on PD-weighted images was depicted at the acromion base, next to the posterior deltoid muscle attachment site, which could illustrate a small nondisplaced linear fracture (Fig. 2). Minimal tendinopathy of the supraspinatus and infraspinatus was also seen, as well as mild degenerative changes of superior glenoid labrum. The association of clinical history of sudden shoulder pain during golf swing, focal tenderness at the acromion site on clinical examination and MRI findings, was suggestive of stress injury of the acromion. The intensity of the edema and a possible thin fracture demonstrates the acuteness of the injury. The patient underwent conservative treatment with nonsteroidal anti-inflammatory drugs for 2 weeks, and rest for 4 weeks. Then, physical activities were gradually reintroduced during following 2 months. Physical evaluation of the patient after 3 months of injury did not revealed pain, and muscle strength was normal. Routine activities and sports were restored without any further complications or recurrence of pain. Discussion Fractures of the scapula infrequently occur, with stress injury of the acromion being an even uncommon entity [1]. Fractures of the acromion may be due to multiple causes and are mostly secondary to trauma [2] and more recently have also been reported following surgery with reverse shoulder arthroplasty [8, 9], with few cases of stress lesions reported so far [1, 3]. Previous reports have described acromion stress fractures visible on radiographs at its different anatomic points (Table 1), but to our knowledge, no report in the literature showed MRI features of such entity. Stress injuries are usually due to abnormal muscular strength applied to a bone with normal resistance [6]. Repetitive loads or a single muscle contraction is a common mechanism of stress fracture of legs, but in the upper extremity this cause is less common, specially at the scapula because it is well protected and highly mobile [3, 4]. The only reported case of similar injury related to golf practice was done by Hall and Calvert [4], in a 42-year-old right-handed woman with a similar history (during golf practice), that presented a linear fracture at the base of the 123 Fig. 1 Sagittal (a), coronal (b), and axial (c) T2-weighted fatsuppressed MR images show extensive bone marrow edema at the acromion (arrow) extending to its base (arrowheads), close to the attachment site of posterior deltoid muscle (curved arrows) Eur J Orthop Surg Traumatol Fig. 2 a and b Sagittal PD-weighted MR images show a hypointense thin line at the acromion base, which could represent a small nondisplaced linear fracture (arrows) acromion visible on plain radiograph. The mechanism suggested would be a strong contraction of the posterior fibers of the deltoid as the head of the golf club swing forward to strike the ball [10], which reminds our case. The bone may also be repeatedly stressed by shots over a short period of time, although there was no history of an excessive amount of golf practice neither in our case nor in the case reported by Hall and Calvert [4]. Acromion injury due to muscle forces related was also reported by Rask and Steinberg [5], but in a different situation, where a car mechanic heard a snap and felt pain over his shoulder while applying torque to a screwdriver, and plain radiograph demonstrated a minimally displaced fracture at the base of the acromion. With the scapula fixed and the deltoid set while holding the shoulder in abduction, probably the adduction and external rotation of the arm during tightening the screw did sufficient bending movement to cause the fracture of the acromion [5]. Another mechanism suggested in the literature is the abnormal pressure from the humeral head on the acromion in the set of rotator cuff arthropathy, as reported by Dennis et al. [2] and Roy et al. [3]. In our patient and in most of the previously reported cases [4–6], there was no rotator cuff arthropathy or violent activity. The most reasonable explanation would be repetitive subcritical load to the shoulder or a single powerful muscle contraction leading to excessive overload at the acromion during the specific activity related by the patient: golf practicing. Although usually seen as a leisurely activity, golf can be a demanding sport and may result in serious injuries, especially regarding the shoulder. Professional and elitelevel golfers often acquire overuse injuries as a result of repeated swings during practice sessions, but also amateur golfers may suffer either from overuse as they work to improve their game or bad technique. The complete golf swing movement is divided into five phases: (1) takeaway (from address until the club is horizontal), (2) backswing (from horizontal to top of backswing), (3) downswing (from top of backswing until the club is horizontal), (4) acceleration (from horizontal club to impact), and (5) follow-through (from ball contact until end of swing). To generate power and clubhead speed, the skilled golfer will Table 1 Previous published case reports of stress fractures of the acromion, listed by year Author Year Anatomic location Related activity Rask and Steinberg [5] Dennis et al. [2] 1978 1986 Neck of acromion Anterior aspect of acromion (3 cases) Applying torque to set a screw above head Chronic rotator cuff arthropathy and osteoporosis Schils et al. [6] 1990 Medial aspect of acromion Professional football player Hall and Calvert [4] 1995 Base of acromion Amateur golf player Ward et al. [1] 1994 Base of acromion (2 cases) Professional football player and jai alai player Roy et al. [3] 2002 Base of acromion Chronic rotator cuff arthropathy and osteoporosis 123 Eur J Orthop Surg Traumatol maximize the shoulder turn relative to the hip turn during the backswing, and in a right-handed golfer, the right posterior deltoid muscle is active mostly during takeaway and backswing [7]. Regarding our case, the correct time of the reported sudden pain is difficult to precise, since in amateurs these phases are not well defined, but it seemed to occur during the transition from backswing to downswing. Most stress injuries of the acromion reported were minimally displaced fractures and healed with conservative treatment, such as immobilization for few weeks followed by gradual motion [2]. As in the typical stress injury, it is important to recognize the pathologic process, with MRI being helpful in theses cases; some of these fractures may even become complete, non-united, or evolute to pseudarthrosis if causative activity is continued [2, 6]. Also, benefits may be obtained with modifications of the golf swing [7], especially in amateur players. Conflict of interest None. References 1. Ward WG, Bergfeld JA, Carson WG Jr (1994) Stress fracture of the base of the acromial process. Am J Sports Med 22(1):146–147 123 2. Dennis DA, Ferlic DC, Clayton ML (1986) Acromial stress fractures associated with cuff-tear arthropathy. A report of three cases. J Bone Joint Surg Am 68(6):937–940 3. Roy N, Smith MG, Jacobs LGH (2002) Stress fracture of base of the acromion. Ann Rheum Dis 61(10):944–945 4. Hall RJ, Calvert PT (1995) Stress fracture of the acromion: an unusual mechanism and review of the literature. J Bone Joint Surg Br 77(1):153–154 5. Rask MR, Steinberg LH (1978) Fracture of the acromion caused by muscle forces. A case report. J Bone Joint Surg Am 60(8):1146–1147 6. Schils JP, Freed HA, Richmond BJ, Piraino DW, Bergfeld JA, Belhobek GH (1990) Stress fracture of the acromion. AJR Am J Roentgenol 155(5):1140–1141 7. Kim DH (2004) Shoulder injuries in golf. Am J Sports Med 32(5):1324–1330 8. Hamid N, Connor PM, Fleischli JF, D’Alessandro DF (2011) Acromial fracture after reverse shoulder arthroplasty. Am J Orthop 40(7):E125–E129 9. Wahlquist TC, Hunt AF, Braman JP (2011) Acromial base fractures after reverse total shoulder arthroplasty: report of five cases. J Shoulder Elbow Surg 20(7):1178–1183 10. Brys P, Geusens E (2007) Scapular, clavicular, acromioclavicular and sternoclavicular joint injuries. In: Vanhoenacker FM, Allen GM (eds) Imaging of orthopedic sports injuries: with 23 tables. Springer, Berlin, pp 169–182