Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
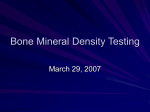
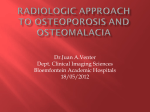
Eur Radiol (2009) 19: 172–176 DOI 10.1007/s00330-008-1099-2 MUSCULO SKELETAL Antonios E. Papadakis Apostolos H. Karantanas Giorgos Papadokostakis Effie Petinellis John Damilakis Can abdominal multi-detector CT diagnose spinal osteoporosis? Received: 7 September 2007 Revised: 9 May 2008 Accepted: 17 May 2008 Published online: 19 July 2008 # European Society of Radiology 2008 E. Petinellis Department of Radiotherapy, Faculty of Medicine, University Hospital of Heraklion, P.O. Box 2208 Iraklion, 71003, Crete, Greece A. E. Papadakis (*) . J. Damilakis Department of Medical Physics, Faculty of Medicine, University of Crete, P.O. Box 2208 Iraklion, 71003, Crete, Greece e-mail: [email protected] Tel.: +30-2810-392092 Fax: +30-2810-542095 A. H. Karantanas Department of Radiology, Faculty of Medicine, University of Crete, P.O. Box 2208 Iraklion, 71003, Crete, Greece G. Papadokostakis Department of Orthopedics, Faculty of Medicine, University Hospital of Heraklion, P.O. Box 2208 Iraklion, 71003, Crete, Greece Abstract The aim of this study was to (1) generate quantitative CT (QCT) densitometric data based on routine abdominal multi-detector (MDCT) examinations and (2) investigate whether these data can be used to differentiate osteoporotic from healthy females. Twenty-five female patients (group A) with a history of radiotherapy were examined both with routine abdominal MDCT and standard QCT to generate a MDCTto-QCT conversion equation. Twentyone osteoporotic (group B) and 23 healthy female patients (group C) were also recruited in the study. Patients of groups B and C underwent routine abdominal MDCT examina- Introduction Osteoporosis is the most common metabolic bone disorder leading to enhanced bone fragility and, consequently, to lowenergy bone fractures. As the elderly population is expected to grow in the coming years, the total number of individuals affected by osteoporosis is also expected to increase dramatically [1]. Quantitative assessment of osteoporosis and estimation of fracture risk relies mainly on bone mineral density (BMD) assessment [2–5]. Dual-energy X-ray tion for various clinical indications. Mean bone mineral density (BMD) in patients of group A was 103.4 mg/ml± 32.8 with routine abdominal MDCT and 91.0 mg/ml±28.5 with QCT. Quantitative CT BMDQCT values for patients in groups B and C were calculated utilizing the BMDMDCT values derived from routine abdominal MDCT data sets and the MDCT to QCT conversion equation: BMDQCT ¼ 0:78 BMDMDCT þ 10:13 . The calculated QCT densitometric data adequately differentiated osteoporotic from healthy females (area under ROC curve 0.828, p=0.05). In conclusion, this study showed that in a group of female patients, QCT data derived from routine abdominal MDCT examinations discriminated osteoporotic from healthy subjects. Keywords Osteoporosis . Multidetector CT . Abdominal imaging . CT densitometry . Image analysis absorptiometry (DXA) and quantitative computed tomography (QCT) of the lumbar spine are currently considered by the clinical and research facilities as the methods most clinically relevant for the evaluation of BMD. The former is accepted by the World Health Organization (WHO) as the gold standard for diagnosing osteoporosis, since it is a method that is inexpensive, rapid, easy to perform, and involves low-radiation exposure. However, it is widely accepted that QCT is the most sensitive method available to detect osteoporosis [6, 7]. Each image slice of a given 173 thickness represents a tissue volume and thus a true volumetric BMD can be obtained, as opposed to areal BMD obtained with DXA. In addition, QCT is able to separately assess the trabecular and cortical BMD. Abdominal MDCT is a quite common radiologic examination, which includes densitometric data on the lumbar vertebrae. The question that arises is whether these densitometric data may be used for accurate BMD assessment. Preliminary studies have shown that high correlation between BMD, as determined with routine abdominal CT, versus lumbar QCT can be achieved [8–10]. The aim of this study was to (1) generate QCT densitometric data based on routine abdominal MDCT examinations and (2) investigate whether these data can be used to differentiate osteoporotic from healthy females. Materials and methods Patients Twenty-five female patients (mean age 61±10.7 years), 12 with history of uterine-cervix cancer and 13 with history of breast cancer, were recruited in the study (group A). These patients are considered to have a high risk of developing osteoporosis. All patients had had conformal radiotherapy and chemotherapy treatments and were referred for abdominal MDCT to rule out tumor recurrence in their long-term follow-up. These patients were additionally scanned with the standard QCT protocol to asses BMD values. The excess exposure of the QCT examination was considered negligible compared to the dose delivered from the previous radiation therapy. Twenty-one osteoporotic female patients (mean age, 69±5.9 years) referred by an orthopedic surgeon for lumbar CT to analyze a possible vertebra fracture after a low-energy trauma were also included in the study (group B). Twentythree female patients (mean age, 70±5.3 years) referred to clinically indicated, non-emergency routine abdominal MDCT were also recruited in the study (group C). Women in group C were selected to match the age range of women in group B. Moreover, they had no premature menopause, history of bone disease, low-energy bone fractures, and trauma or malignancies. They were not subjected to any medical treatment with drugs that might influence their bone metabolism. Patients in groups B and C underwent only routine abdominal MDCT examination. The study was approved by the local ethics committee, and informed consent was given by all patients who participated in the study. CT scan protocols and image analysis All CT examinations were performed with a 16-slice CT system (Somatom Sensation 16, Siemens, Erlangen, Germany). QCT examinations were performed using an application-specific QCT protocol according to the manufacturer’s instructions and a dedicated calibration phantom [11] (Osteo calibration phantom, Siemens). The QCT protocol constituted of 2×5=10-mm slice thickness sequential scans, acquired with 80 kVp tube potential and 125 mAs tube load. The S80 kernel was used for image reconstruction. Before acquiring the QCT data, a lateral scout image of the lumbar spine of the subject was obtained. For correct patient positioning, a gel pack sponge was placed in between each patient’s spine and the calibration phantom during acquisition. Four sequential QCT data sets were acquired per patient, each corresponding to the midvertebral sections of T12, L1, L2, and L3 vertebra. The gantry was tilted appropriately before each acquisition so that the orientation of the acquired image slice was always parallel to the upper and lower endplates. By using the implemented Osteo software (Siemens), automatic contour tracing of the trabecular and the cortical bone was performed on each image slice. An easy manual interaction for contour tracing modification was allowed. The trabecular and cortical bone regions of each vertebra are automatically divided into the left and the right subregions. Images with artifact structures within the vertebral region were excluded from the measurements. Trabecular and cortical BMD values are calculated based on the comparison with a standard table, which includes a healthy bone reference group with age- and sex-specific data from three European centers (Siemens, QCT Reference). The BMDs per subject were derived by averaging four vertebral bodies (T12, L1-L3). A routine abdominal MDCT protocol was used for the examination of all patients (groups A, B, and C). CT parameters were as follows: tube voltage 120 kVp, tube load 160 mAs, beam collimation 16×1.5 mm, table feed 24 mm, reconstruction image slice 10 mm, and reconstruction kernel B31. The dedicated calibration phantom was used as in QCT. Before MDCT, all patients had been given 1,000 ml of oral contrast medium (0.3 g/ml, Iopamiro Gastro, Bracco, Italy). Based on the scout image and by analyzing the series of the acquired images, the slices closest to the midvertebral sections of T12, L1, L2, and L3 vertebra were selected for BMD assessment. In these slices, BMD values of the trabecular and the cortical bone were calculated following the same automated procedure described above for the QCT. All data acquisition and analyses were performed by a radiology technologist who was supervised by an experienced radiologist. During this procedure investigators were blinded to each patient’s history, fracture status, and BMD as determined with QCT. To give an indication of the error introduced in the calculation of the BMDQCT, we have examined an anthropomorphic Rando phantom (Alderson Research Laboratories, Stanford, CA) with the QCT and abdominal CT protocols. This phantom consists of human skeleton embedded in lung- and tissue-equivalent material and 174 corresponds to a young male individual with average anatomical characteristics. The Rando was examined on top of the osteo calibration phantom. To study the effect of table height on BMD, the Rando anthropomorphic phantom was also scanned in different table heights, i.e., 125 mm, 135 mm, 145 mm, and 155 mm. At each table height, the QCT and the abdominal CT were repeated three times. Mean BMD values averaged over T12, L1, L2, and L3 were calculated at each table height. Statistical analysis Mean BMD values and standard deviations (SDs) were calculated for all patients. The relationship between measurements obtained with QCT and abdominal MDCT in group A was assessed based on a linear regression analysis. The correlation parameters between QCT and abdominal MDCT calculated for group A were used to predict the BMDQCT values for groups B and C. A twotailed Student’s t-test was applied to compare mean BMD values among groups. The capability of QCT and abdominal MDCT to discriminate between fractured and nonfractured subjects was assessed by calculating ROC curves. Statistical significance was taken at P<0.05. All statistical computations were processed using the MedCalc software package (MedCalc software, Belgium). Results Figure 1 illustrates the BMD values obtained from standard QCT as a function of the corresponding values obtained from abdominal MDCT in patients with history of radiotherapy (group A). Each point in the scatter plot is an average of the trabecular BMD value over the T12 and L1 through L3 vertebrae for each patient. The linear BMDQCT ¼ 0:78 BMDMDCT þ 10:13 The correlation coefficient r was 0.90 (p<0.0001). Table 1 lists the mean BMDMDCT values derived from the abdominal MDCT of the patients in the three groups, the mean BMDQCT values derived from the QCT of the patients in group A, and the mean BMDQCT values of the patients in groups B and C. The latter values were calculated utilizing the measured BMDMDCT values and the above equation. The difference between the mean BMDQCT values of the osteoporotic (group B) and healthy patients (group C) was statistically significant (p=0.0001; 95% CI: 9.41 to 25.94). Moreover, the receiving-operator characteristic curve (ROC), shown in Fig. 2, indicated that abdominal MDCT may adequately discriminate healthy and osteoporotic women. Area under the curve is 0.828 with 0.063 standard error at the 95% confidence interval. Mean BMD values averaged over the T12, L1, L2, and L3 vertebra of the Rando anthropomorphic phantom for QCT and abdominal CT were 209.5 mg/ml and 231.5 mg/ml, respectively. If the above equation is applied to calculate the anticipated BMDQCT value,it would be: BMDQCT ¼ 0:78 231:5 þ 10:13 ¼ 190:7 mg ml . Given that the measured by the QCT scan BMDQCT value is 209.5 mg/ml, the error introduced by the conversion equation in estimating BMDQCT value is 8.9%. Although this error is not negligible, we consider that it is partly due to the fact that the above phantom represents a young male individual, while the conversion equation was generated on female patients aged 61±10.7 years. The coefficient of variation in the mean BMD among scans performed at different table heights was less than 1.5%. Discussion The advent of multi-detector CT has significantly increased the number of CT examinations. Surveys performed in the US reveal that the annual number of CT examinations has increased almost ten-fold in less than 2 decades [12]. Quantitative CT is a well-established technique used to 160 BMDQCT (mg Ca-HA/ml) regression analysis relating the two BMD measurement methods provided the following equation: 140 120 100 Table 1 Mean densitometric measurements in different group populations obtained from standard abdominal MDCT and QCT 80 60 40 Abdominal MDCT mg/ml a QCT mg/ml 103.4±32.8 84.7±15.3 109.9±15.6 91.0±28.5 76.3±11.9 96.08±12.2 20 40 60 80 100 120 140 160 180 BMDMDCT (mg Ca-HA/ml) Fig. 1 Correlation between bone mineral densities determined with QCT (BMDQCT) and abdominal MDCT (BMDMDCT); r=0.90, P<0.0001 Group A Group B Group C a QCT values for groups B and C were calculated based on the QCTabdominal CT calibration equation derived from patients in group A 175 100 Sensitivity 80 60 40 20 0 0 20 40 60 80 100 100-Specificity Fig. 2 ROC curve of abdominal MDCT in differentiating osteoporotic (group B) from healthy women (group C) measure BMD. With optimized acquisition parameters and dedicated software, the method has been widely used to detect patients with osteoporosis. The results of this study show that the densitometric data generated from routine abdominal MDCT can be additionally used to differentiate osteoporotic from healthy females. Hopper et al. [9] analyzed contrast-enhanced and unenhanced abdominal CT and QCT to assess BMD in the L1, L2, and L3 vertebral bodies. That study aimed to establish a baseline that could be used as a reference for subsequent bone density studies. The findings of Hopper et al. [9] showed that BMD values obtained with QCT (90.6 mg/ml) are lower than those obtained with unenhanced abdominal CT (98.5 mg/cm3). These findings are in agreement with those of our study. However, that study was performed with a single-slice CT system. Lang et al. [7] showed that BMD values derived from the standard helical scan of L1 and L2 vertebral bodies may adequately discriminate patients with vertebral factures from healthy individuals. However, Lang et al. [7] did not recruit any population for the generation of a helical vs. QCT correlation coefficient. Link et al. [8] evaluated if nondedicated standard spiral CT can be used to obtain reliable bone mineral density data. That study showed that there is a significant correlation in the densitometric measurements between routine spiral CT and QCT. Quantitative CT BMD values can be derived using BMD values from routine spiral CT multiplied by a conversion factor. That factor was generated based on the correlation between standard spiral CT and QCT. The results presented in the current study are in agreement with those presented by Link et al. [8]. The current study is differentiated from that of Link et al. [8]. First, the generation of the abdominal MDCT to QCT conversion equation was based on non-contrastenhanced abdominal MDCT scans. On the contrary, the patients examined by Link et al. [8] underwent both intravenous and oral administration of contrast medium before abdominal CT, which alters the BMD of the bone marrow in the vertebrae. The alteration in BMD depends on the amount of intravenously administered contrast media, which may vary from patient to patient according to the specifications. Therefore, we believe that an abdominal MDCT to QCT conversion based on densitometric data not affected by contrast interference, similar to those presented in this study, is more appropriate. Second, the CT system used in our study is a modern 16-slice scanner as opposed to the 4slice CT machine used by Link et al. [8]. CT systems with different configuration technologies (beam geometry, tube potential, tube filtration, etc.) may be associated with diverse MDCT-to-QCT conversion equations. Hence, the conversion equation presented in the current study may be used from all institutions equipped with a similar 16-slice system to generate QCT densitometric data from routine abdominal MDCT. Several studies on the comparison of bone densitometry methods and measurement techniques have shown that QCT exhibits the highest sensitivity [13, 14]. One of the fundamental advantages of QCT is that selective measurement of the trabecular region excludes sources of error such as osteophytes and hypertrophic posterior elements that artificially elevate BMD values, thus reducing their diagnostic efficacy. In spite of QCT’s high sensitivity and valuable power in diagnosing osteoporosis, DXA has dominated in the routine clinical practice. This is attributed to the (1) lack of availability of CT systems that are equipped with the appropriate hardware and software required for image acquisition and densitometric analysis, (2) high cost of a MDCT examination, and (3) the inconvenience of use compared to DXA, which is a more automated procedure and requires less operator intervention for image analysis and result derivation. Radiation exposure may be considered as another reason why DXA has dominated over QCT. The effective dose delivered by DXA is lower than background radiation and is considered to be negligible. The findings presented in the current study suggest that routine abdominal MDCT may detect osteoporotic women without an excess of radiation burden due to QCT or DXA. Thus, patients undergoing routine abdominal MDCT could, at the same time, be potentially evaluated for bone densitometry if clinically indicated. The present study has its limitations. The patients participated in the current study did not undergo DXA. Further studies are required to validate that patients are correctly classified as osteoporotic. These studies need to incorporate parameters such as the patient’s medical history, physical examination, as well as DXA findings. The correlation between QCT and abdominal MDCT could 176 be ideally validated using anthropomorphic phantoms. However, commercially available anthropomorphic phantoms represent only young healthy individuals. Female anthropomorphic phantoms in a wide range of ages should be constructed to verify patient data. Moreover, this study was performed with 16-slice CT. This is a widespread modern system that is installed in many clinical institutions around the world. However, it would be interesting to evaluate the results on 64-slice CT systems, which are now quite widely available. In conclusion, this study showed that densitometric data derived from routine abdominal MDCT examinations differentiated osteoporotic from healthy females. Further studies are needed before routine abdominal MDCT can be considered as a useful method to diagnose spinal osteoporosis in everyday clinical practice. References 1. Lau EMO (2001) Epidemiology of osteoporosis. Best Pract Res Clin Rheumatol 15:335–344 2. Guglielmi G, Lang TF (2002) Quantitative computed tomography. Semin Musculoskelet Radiol 6:219–227 3. Karantanas AH, Kalef-Ezra JA, Glaros DC (1996) Quantitative computed tomography for bone mineral measurement: technical aspects, dosimetry, normal data and clinical applications. Br J Radiol 64:298–304 4. Link TM, Majumdar S, Grampp S, Guglielmi G, van Kuijk C, Imhof H, Gluer C, Admas JE (1999) Imaging of trabecular bone structure in osteoporosis. Eur Radiol 9:1781–1788 5. Link TM, Guglielmi G, van Kuijk C, Adams JE (2005) Radiologic assessment of osteoporotic vertebral fractures. Eur Radiol 15:1521–1532 6. Grampp S, Genant HK, Mathur A, Lang P, Jergas M, Takada M, Gluer CC, Lu Y, Chavez M (1997) Comparisons of non-invasive bone mineral measurements in assessing age-related loss, fracture discrimination and diagnostic classification. J Bone Min Res 12:697–711 7. Lang TF, Guglielmi G, van Kuijk C, De Serio A, Cammisa M, Genant HK (2002) Measurement of bone mineral density at the spine and proximal femur by volumetric quantitative computed tomography and dual-energy X-ray absorptiometry in elderly women with and without vertebral fractures. Bone 30:247–250 8. Link T, Koppers B, Licht T, Bauer J, Lu Y, Rummeny EJ (2004) In vitro and in vivo spiral CT to determine bone mineral density: initial experience in patients at risk for osteoporosis. Radiology 231:805–811 9. Hopper KD, Wang MO, Kunselman AR (2000) The use of clinical CT for baseline bone density assessment. J Comput Assist Tomogr 24:896–899 10. Weishaupt D, Schweitzer A, DiCuccio M, Whitley P (2001) Relationships of cervical, thoracic, and lumbar bone mineral density by quantitative CT. J Comput Assist Tomogr 25:146–150 11. Kalender W, Suess C (1987) A new calibration phantom for quantitative computed tomography. Med Phys 14:863–866 12. Kalra M, Maher M, Toth T et al (2004) Strategies for CT radiation dose optimization. Radiology 230:619–628 13. Brown JP, Josse RG, for the Scientific Advisory Council of the osteoporosis Society of Canada (2002) 2002 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ 167(suppl.10):S1–S34 14. Blake GM, Fogelman I (1998) Applications of bone densitometry for osteoporosis. Endocrinol Metab Clin N Am 27:267–288