Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
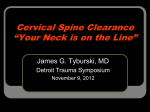
CE ......................................................................... . . . . . . . . . . . . . . . . . . . . . . . . . . . ASRT members Click Here to earn CE credit for passing the Directed Reading Quiz. DIRECTED READING Traumatic Injuries to the Cervical Spine JENNIFER MINIGH, PH.D. Nowhere in radiography are the standards for imaging more important than in dealing with traumatic spine injury. This article provides an overview of cervical spine trauma and specifically addresses various injuries and how to image them. This article is a Directed Reading. See the quiz at the conclusion. After completing this article, readers will be able to: ■ Describe the basic anatomy of the cervical spine. ■ List and describe various forces involved in spinal injury. ■ Discuss various cervical spine injuries. ■ Present recommendations, limitations and diagnostic challenges of imaging cervical spine trauma. ■ Address other patient considerations including safety and care. I n May 1995, Hollywood met heartache. Christopher Reeve, America’s favorite superhero, broke his neck when he was thrown from his horse during an equestrian competition. His resulting paralysis was not enough to hold down this hero, though. Mr. Reeve was willing to share his disability struggles and to speak out, campaigning tirelessly for spinal cord injury and research. Approximately 10 000 cervical spine fractures occur annually, comprising 2.6% of all trauma victims. These cervical spine injuries cause an estimated 6000 deaths and 5000 new cases of quadriplegia each year.1 Motor vehicle accidents and falls account for 50% and 20% of these injuries, respectively. In fact, approximately 5% to 10% of unconscious patients who present to the emergency department as the result of a motor vehicle accident or fall have a major injury to the cervical spine. Sports-related activities account for another 15% of cervical spine injuries. Participants in sporting events such as diving, equestrian activities, football and gymnastics are considered to be at a high risk for spinal trauma. Of the new cervical spine fractures each year, as many as 47% of patients suffer neurologic complications resulting RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 in devastating psychological, physical and financial losses. The mortality rate among trauma patients with cervical fractures who required intubation was 37%, with most deaths related to associated injuries, particularly head injury.2 Perhaps the most concerning statistic is that 10% of all spinal-cord injured patients arrived at the emergency department neurologically intact.3 Normal Cervical Spine Anatomy The purpose of the cervical spine is to protect the spinal cord and to support the skull while enabling diverse head movements. This is a big job considering that cervical vertebrae are smaller than the other spinal vertebrae. The normal anatomy of the cervical spine consists of 7 vertebrae separated by intervertebral disks. (See Fig. 1.). The basic parts of a vertebra are an anterior body and a posterior arch which consists of the pedicles and laminae. One distinguishing feature of the cervical vertebrae is the presence of a transverse foramen in the transverse process. The vertebrae are joined by a complex network of ligaments. These ligaments keep individual bony elements behaving as a single unit. In 1983, Denis4 proposed 53 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES Fig 1. Typical cervical vertebrae. Axial CT image (above right) showing the parts of a typical cervical vertebra (C3-C6). A 3-D reconstruction from an axial CT examination (above left). (Image courtesy of Nicholas Joseph Jr. Reprinted with permission from: www.radiographicceu.com/article5.html.) Fig. 3. Atlas (C1) and axis (C2). Fig. 2. Three-column model. (Image courtesy of Nicholas Joseph Jr. Reprinted with permission from: www.radiographicceu.com/ article5.html.) a 3-column model of the spine. One can view the cervical spine as 3 distinct columns: anterior, middle and posterior. (See Fig. 2.) The anterior column consists of the anterior longitudinal ligament and the anterior two thirds of the vertebral body. The middle column is formed by the posterior longitudinal ligament and the posterior one third of the vertebral body. The posterior column is made up of the remaining ligamentous and vertebral structures. The anterior and posterior longitudinal ligaments maintain the structural integrity of the anterior and middle columns. The posterior column is held in alignment by a more complex ligament system. 54 Upper Cervical Region: The Atlas (C1) and the Axis (C2) The atlas and the axis are atypical vertebrae. (See Fig. 3.) The atlas (C1) is ring like and somewhat kidney shaped when viewed from above or below. It has no spinous process or body and consists of 2 lateral masses connected by anterior and posterior arches. The atlas carries the cranium and rotates on C2’s large, flat superior articular facets. The axis (C2) vertebra is the strongest cervical vertebra. Its distinguishing feature is an odontoid process that is a tooth-like structure projecting from the vertebra. This odontoid process is often referred to as the dens. The dens is held tightly to C1 by the transverse ligament, thus stabilizing the atlantoaxial joint, which is a pivot joint that allows rotational movements like shaking the head when saying “no.” (See Fig. 4.) These ligaments provide further stabilization by permitting spinal column rotation and preventing posterior displacement of the dens in relation to the atlas. The C2-C3 Interface Rotation of the axis on C3 is limited by a blocking September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING Table 1 Motor Deficits and Mobility Consequences for Corresponding Cervical Fractures Level of Injury Fig. 4. Linear tomogram through C1-C2. The left image is labeled, whereas the right is not labeled to demonstrate a clear view of the atlantoaxial joints and odontoid process. (Image courtesy of Nicholas Joseph, Jr. Reprinted with permission from: www.radiographicceu.com/article5.html.) mechanism that protects the vertebral artery from excessive torsion. This blocking mechanism is also found in the subjacent cervical vertebrae. Lower Cervical Region The lower cervical vertebrae are typical in structure with some exceptions. In this region, the laminae are slender and overlap to create a shingling pattern that increases with age. The seventh cervical vertebra is considered an atypical cervical vertebra because of its long spinous process that can be seen and felt in the back of the neck. Cervical Spine Injuries and Neurologic Deficits The technologist must appreciate the fact that injury to a vertebra does not directly correlate with injury to the spinal cord. Likewise, injury to the spinal cord does not require a vertebral fracture. In other words, a person may “break his neck” yet not sustain a spinal cord injury (SCI) when only the vertebrae are damaged but the spinal cord is not affected. In these situations, the individual may not experience paralysis after the bones are stabilized; however, as many as 39% of cervical fractures have some degree of associated neurologic deficit. The effects of SCI depend on 2 factors: the type of injury and the level of injury. Furthermore, SCI can be divided into 2 types of injury — complete and incomplete. A complete injury means that there is no function below the level of the injury; there is no sensation and no voluntary movement, with both sides of the body equally affected. An incomplete injury means that there RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 Motor Deficits Mobility Consequence C1, C2, C3, C4 Paralysis of all 4 limbs Power wheelchair (chin drive or sip-n-puff) C5 Shoulder and biceps control without control of wrist or hand Power wheelchair (arm drive) C6 Wrist control without hand function Manual and/or power chair-sliding board transfers C7, T1 Dexterity problems with the hand and fingers Manual chair transfers w/o sliding board is some functioning, whether it is movement or sensation, below the primary level of injury. The level of SCI is very helpful in predicting what parts of the body might be affected. In general, the higher up the spinal column the injury occurs, the more dysfunction a person will experience. Injuries to the cervical spinal cord result in paralysis of all 4 limbs, which is termed tetraplegia or, more often, quadriplegia. Injuries below the cervical spine result in paraplegia, a paralysis of the legs and portions of the trunk. Quadriplegia is slightly more common than paraplegia. Table 1 summarizes various motor deficits and mobility consequences for corresponding cervical fractures. Beside a loss of sensation or motor function, individuals with SCI also experience other changes. Very high injuries (C1, C2) can result in a loss of many involuntary functions including the ability to breathe. SCIs may cause sexual dysfunction or dysfunction of the bowel and bladder. Other effects of SCI may include chronic pain, in addition to altered regulation of blood pressure, body temperature and the ability to sweat below the level of injury. When an SCI occurs, there usually is swelling of the spinal cord that may incur further injury and loss of function. With time, the swelling will begin to dissipate and the individual may regain some functioning. In the event of an incomplete injury, the individual may recover some functioning as late as 18 months following the injury. However, only a very small fraction of individuals sustaining SCIs completely recover. 55 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES ! " # Fig. 6. Dens fracture. A. Type I. B. Type II. C. Type III Fig. 5. Jefferson burst fracture. A. Open-mouth odontoid projection. Note bilateral displacement of lateral masses (LM) and widened lateral atlantodental interval (*). B. Lateral projection. Note bilateral posterior arch C1 fractures (arrow) and widened anterior atlantodental interval (*). (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www.uth.tmc. edu/radiology/test/er_primer/index.html.) Cervical Fractures Most cervical spine fractures occur at 2 levels. One third of fractures occur at the level of C2, while one half of injuries occur at the C6 or C7 levels. As reported in accident statistics, the most vulnerable segments to injury are the axis and C5-C6. According to the National Spinal Cord Injury Statistical Center’s 2004 annual statistical report,1 of the patients discharged with a cervical spine injury, 39% had injuries that occurred at C4-C6. According to the report, the atlas was the least involved of all cervical vertebrae. Mechanisms of Injury Nonangular stresses and rotational/angular forces are the 2 main mechanisms for spinal injury. Nonangular forces include compression and shear force. Rotational/angular forces include hyperextension, hyperflexion and hyperrotary forces. Compression Forces. This mechanism is best explained as a force produced when a heavy object is placed on top of the head. Excessive compression forces on the neck commonly lead to facet jamming and fixa- 56 tion. In addition, these forces can cause fractures of the atlas or lower cervical bodies. The fractures may be vertical, oblique or bursting in nature. Shear Forces. Undue shearing forces can disrupt ligaments and produce anterior or posterior subluxation. Also, these forces can create anterior or posterior fractures of the dens or cause anterior compressive fractures of the atlas or vertebral body. Hyperextension Forces. This mechanism is best described as the force produced when a person strains to look up by bending the head back. The effects of forceful posterior bending include ligament sprain, wedging of a vertebral body, posterior subluxation and fractures of the atlas or vertebral body. Hyperflexion Forces. An example of this mechanism is the force produced when a person strains to look down by bending the head forward. Excessive anterior bending may produce much the same effects as hyperextension forces. Lateral Hyperflexion Forces. This is best explained as the force produced when a person attempts to place his or her ear on a shoulder. The effects of excessive lateral bending include dislocation and fractures of processes, including the odontoid process. In addition, lateral wedging of vertebral bodies may occur. Hyperrotary Forces. This force is produced when a person strains to look over his or her shoulder. Extreme rotation of the longitudinal axis may produce ligament torsion, rotary subluxation, spiral loosening and atlasaxis dislocation. Upper Cervical Fractures C1 Atlas. Isolated fractures of the atlas are rare and divided into types I, II and III.5 Jefferson first described the type II fracture pattern as a “burst” pattern.6 This fracture can occur from a severe axial force causing compression. (See Fig. 5.) If the force is great enough, such as that which occurs in diving injuries, the vertebral arch or body of the adjacent vertebra literally bursts. Another fracture, the pillar fracture, is an iso- September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING Fig. 7. Hangman’s fracture, lateral view. Note the fracture (arrows) and the C2-C3 disk space (*). (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www. uth.tmc.edu/radiology/test/ er_primer/index.html.) lated fracture of the lateral mass of C1. Regardless of fracture type, stability is defined as an intact transverse longitudinal ligament. The “Rule of Spence” is used to assess the integrity of this ligament and its stability. The rule states that on an open-mouth odontoid projection, the displacement of the lateral masses to a certain degree implies a ruptured ligament. All stable patients with a C1 fracture should have a magnetic resonance (MR) image taken to assess the integrity of the ligament. If the ligament is ruptured, this is considered the most unstable of all cervical spine fractures.7 C2 Axis. Fractures of the axis also are divided into 3 types: dens, hangman’s and other.8 The dens fracture is the most common form and has 4 subtypes that are classified according to the fracture location, whether it be at the tip, base, body or some combination of the dens and vertebra. (See Fig. 6.) The hangman’s fracture, originally named to describe the effects of hanging a person from a gallows, now refers to bilateral fracture of the pedicles of the axis caused by hyperextension or sudden deceleration. (See Fig. 7.) In present times, this type of fracture most commonly results from a car accident in which the victim strikes the windshield with his forehead. A hangman’s fracture often causes death by suffocation, which nearly occurred during Reeve’s tragic equestrian accident. Axis with Atlas Fractures. In the largest case series examining combined fractures, 43% of axis fractures and 16% of atlas fractures occur in unison.9 There are 4 main fracture combinations. The most common is the C1-type II odontoid fracture, while the least common fracture pattern is the C1-hangman. Combination fractures of C1 and C2 should be evaluated by computed tomography (CT), with reconstruction whenever an isolated C1 or C2 fracture is seen.10 Lower Cervical Fractures Lower cervical spine fractures are classified into 4 RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 Fig. 8. Flexion tear drop fracture, lateral view. Arrow points to “tear drop” fragment. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www.uth.tmc. edu/radiology/test/er_ primer/index.html.) major subtypes according to the forces involved in the mechanism of injury: hyperflexion, hyperextension, compression and lateral flexion/shearing.11,12 Fractures Caused by Hyperflexion. The flexion tear drop fracture is a fracture of the inferior-anterior portion of a vertebral body, typically occurring at C2. (See Fig. 8.) It is often the result of diving into shallow water. This fracture is the most severe and unstable injury of the cervical spine. Subluxation is defined as a partial dislocation of a bone in its joint. In terms of the spine, it is displacement of a vertebra. Anterior subluxation in the cervical spine occurs when posterior ligament complexes rupture. (See Fig. 9.) The anterior longitudinal ligament remains intact and no associated bony injury is seen. Because the anterior columns remain intact, this fracture is considered mechanically stable. However, most authorities approach this injury as if it were potentially unstable because of the significant displacement that can occur. A few very rare cases have reported neurologic deficit. Subluxation between 25% and 50% of the vertebral body is generally consistent with a unilateral facet dislocation (sometimes referred to as the “locked” vertebra), whereas subluxation of more than half of the vertebral body indicates a bilateral facet dislocation. (See Fig. 10.) This is an extremely unstable condition and is associated with a high prevalence of SCI. In addition, a significant 57 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES Fig. 9. Anterior subluxation, lateral view. Crossed lines indicate the abnormal curvature (arrow) typical of anterior subluxation. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www. uth.tmc.edu/radiology/test/ er_primer/index.html). number of bilateral facet dislocations are accompanied by disk herniation. A clay shoveler’s fracture is a forcible detachment of a spinous process caused by a sudden load on a flexed spine. (See Fig. 11.) This fracture occurs most often at C6, C7 or T1 and is the most stable of the cervical spine fractures. Fractures Caused by Hyperextension. An extension tear drop fracture is radiographically similar to the flexion tear drop fracture, involving the anterior-inferior portion of a vertebral body. However, this fracture is more stable than the flexion fracture. A fracture of the neural arch of C1 occurs when the head is hyperextended and the posterior neural arch of C1 is compressed to the point of fracture. Because the transverse ligament and the anterior arch of C1 are not involved, this fracture is stable. Fractures Caused by Compression. A burst fracture occurs when a downward compressive force is transmitted to lower levels in the cervical spine, causing the body of the cervical vertebra to shatter outward in a bursting pattern. (See Fig. 12.) The Jefferson burst fracture of C1 has been discussed previously as an upper cervical fracture. Burst fractures involve disruption of the anterior and middle columns. In addition, these fractures are much more severe than simple compression fractures because the bones spread out in all directions and may damage the spinal cord. Fractures Caused by Lateral Flexion/shearing. Between 4% and 6% of cervical spine injuries occur from this mechanism. Occupants of a vehicle that has been broadsided will likely suffer this injury. The impact propels the victim’s body in 1 direction while the head 58 Fig. 10. Bilateral facet dislocation, lateral view. Note that the body of C4 (a) has an anterior translation equivalent to 50% of the diameter of the vertebral body. The arrow denotes anterior dislocation of each articular mass of C4. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www. uth.tmc.edu/radiology/test/er_primer/index.html.) and neck go in the opposite direction. Examples of fractures include uncinate fracture, isolated pillar fracture (see Fig. 13), transverse process fracture and lateral vertebral compression. Cervical Spine Stability The stability of C3-C7 fractures is based on a 3column theory described by Denis.4,13 As previously described, the 3 spinal columns (anterior, middle and posterior) work in conjunction to provide stability to the spine. (See Fig. 2.) Column disruption can lead to mechanical instability of the cervical spine. If 1 column is disrupted, other columns may provide sufficient stability to prevent SCI. If 2 columns are disrupted, the spine may move as 2 separate units, thus increasing the likelihood of SCI. Fractures are considered unstable if more than 1 column is disrupted. The degree of instability depends on several factors, including degenerative changes related to aging, arthritic conditions, spinal stenosis and spina bifida, as well as the specific mechanism and location of the injury. Trafton7 has ranked specific cervical injuries based on their degree of mechanical instability. The following list ranks cervical spine injuries September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING A. Fig. 12. Burst fracture of lower cervical spine. Axial CT scan showing a sagittal fracture of the body (a), retropulsed body fragments (arrows) and laminar fracture (c). (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www. uth.tmc.edu/radiology/test/er_primer/index.html.) B. Fig. 11. Clay-shoveler’s fracture. A. Anteroposterior view. B. Lateral view. Arrow indicates spinous process fracture line and displacement of superior fragment. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www.uth.tmc. edu/radiology/test/er_primer/index.html.) in order of instability (most stable to least stable): (See Table 2.) ■ Rupture of the transverse ligament of the atlas. ■ Fracture of the dens. ■ Flexion teardrop fracture. ■ Bilateral facet dislocation. ■ Hangman fracture. ■ Extension teardrop fracture. ■ Jefferson fracture. ■ Unilateral facet dislocation. ■ Anterior subluxation. ■ Simple wedge compression fracture. ■ Fracture of the posterior arch of C1. ■ Clay shoveler’s fracture. Imaging the Cervical Spine The first step in imaging the cervical spine is to determine if the patient actually needs imaging and, if so, which projections are appropriate. The criteria for imaging apply only to adults with no mental status changes, including drug or alcohol intoxication. The presence of the following should be noted: RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 Fig. 13. C4 pillar fracture. Arrows indicate the “doubleoutline” sign. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www.uth. tmc.edu/radiology/ test/er_primer/index. html.) ■ Neurologic deficits consistent with a cord lesion, such as sensory and motor deficits. ■ Altered sense of reality due to head injury or intoxication. ■ Complaints of neck pain or tenderness. ■ Significant other injuries that may preclude any complaints about neck pain or tenderness. Although some research suggests that these criteria also may be used in the management of verbal children,14-16 caution is in order because the studies were small, and the ability of children to complain about pain or sensory changes can vary. ACR Imaging Guidelines The American College of Radiology (ACR) Committee on Appropriateness Criteria has developed 59 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES Table 2 Common Injuries of the Cervical Spine Spinal Level C1 Injury [Figure #] Stability Cause Jefferson fracture [5] Moderately unstable Severe axial force causing compression Odontoid projection: displaced lateral masses of C1 Atlantoaxial subluxation Highly unstable Unknown but often occurs in patients with bone degeneration Odontoid projection: asymmetric lateral Hangman’s fracture [7] Unstable Hyperextension or sudden deceleration Lateral projection: bilateral pedicle fracture of C2 Odontoid fracture [6] Highly unstable Unknown May be difficult to see on plain-film radiographs; may require CT scanning C6, C7, T1 Clay shoveler’s fracture [11] Stable Sudden load on a flexed spine Forcible detachment of spinous process; frequently an incidental finding Any Flexion teardrop [8] Highly unstable Sudden and forceful flexion Large wedge off the anterior aspect of the vertebra; alignment abnormalities Bilateral facet dislocations [10] Highly unstable Flexion, or a combination with rotation Anterior displacement of more than half of the diameter of the vertebral body in the lateral view Unilateral facet dislocations Unstable Flexion or a combination with rotation Anterior dislocation of 25% of a cervical vertebra on lateral views C2 guidelines17,18 for determining appropriate imaging examinations to diagnose specified medical conditions, namely spinal injury. These criteria are intended to guide professionals in making decisions regarding radiologic imaging and treatment. The ACR cautions, however, that using the guidelines blindly in a “protocoldriven” manner may result in many unnecessary studies. Conventional Radiography The ACR states that if the above criteria are met, plain-film radiographs are the mainstay of the initial imaging evaluation. The exam should include 3 projections: a true lateral projection, an anteroposterior projection; and an open-mouth odontoid projection. (See Fig. 14.) A lateral projection using the Twining method, commonly called the “swimmer’s lateral,” for T1 is frequently needed, especially in men. The importance of obtaining all these projections, described in more detail below, and demonstrating all of the vertebrae cannot be overemphasized. Although some missed cervical fractures are the result of image misinterpretation, the most frequent cause of overlooked injury is an inadequate film series.19,20 (See Table 3.) 60 Radiologic Findings Lateral projection. Approximately 85% to 90% of cervical spine injuries are evident in a lateral projection, making it the most useful image from a clinical standpoint. (See Fig. 14a.) However, some experts believe the single portable cross-table lateral radiograph, often obtained in the trauma room, should be abandoned. This projection is insufficient to exclude a cervical spine fracture and frequently must be repeated in the radiology department.21,22 For complete imaging, the lateral projection must include all 7 cervical vertebrae as well as the C7-T1 junction. If no arm injury is present, traction of the arms may help to demonstrate all 7 vertebrae on the lateral film. If all 7 vertebrae and the C7-T1 junction are still not visible, a swimmer’s lateral, taken with 1 arm extended over the head, may remedy the problem. (See Fig. 15.) Because there is less scatter, a coned-down swimmer’s lateral gives better detail than does the full cervical spine swimmer’s projection, especially when using digital imaging. Anteroposterior projection. This projection is used to reveal the spinous processes of C2 to T1; however, it is the least useful projection from a clinical standpoint.23 (See Fig. 14b.) September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING A Fig. 15. Swimmer’s lateral projection. (Image courtesy of Nicholas C Joseph, Jr. Reprinted with permission from: www.radiographicceu. com/article5.html.) B Fig. 14. The standard radiographic image series to evaluate trauma of cervical spine. A. Lateral projection. B. Anteroposterior projection. C. Open-mouth odontoid projection. (Image courtesy of Thea Trötscher, R.N., and John H. Harris, M.D. Reprinted with permission from: Harris & Harris Emergency Radiology Primer at www.uth.tmc.edu/radiology/test/er_primer/index.html.) Odontoid projection. The open-mouth odontoid projection is used to evaluate an area that is difficult to demonstrate on a cross-table lateral image because of shadow superimposition. (See Fig. 14c.) It is used to assess trauma to C2. Occasionally, the tip of the odontoid process is not adequately visualized, and the technologist may use the Fuchs method, which is a modified projection to demonstrate the superior third of the odontoid tip. However, this projection is unreliable when the patient is in a cervical collar and the neck cannot be extended. Oblique and flexion/extension radiographs. Plainfilm imaging beyond lateral and anteroposterior projections may be useful in selected cases. Supine oblique studies aid in examining lateral masses, whereas flexion and extension projections are commonly used for patients with severe pain and tenderness but who have normal lateral and anteroposterior films.24 These additional studies are not generally used for routine protocols. Oblique projections are most valuable in adding 2 more images of the C7-T1 junction. This is considered a laminar projection because the image can reveal disruptions in the normal shingling appearance of the verte- RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 bral laminae. Because both of these functions can now be accomplished through the use of CT, the ACR states that the use of supine oblique projections is no longer necessary for patients who are undergoing cervical CT examination. According to the Eastern Association for the Surgery of Trauma (EAST), a panel created to evaluate and develop evidence-based guidelines for controversial topics in trauma, a patient with significant midline pain requires flexion/extension projections to evaluate for ligamentous injury, which commonly arises from hyperrotational injuries.25 (See Fig. 16) These radiographs should only be obtained in conscious patients who are able to cooperate. The patient should be able to limit the motion of his or her neck based on the occurrence of pain. Under no circumstances should cervical spine flexion and extension be forced, as this may result in SCI. Although the literature still recommends flexion/ extension radiographs, the ACR states that these projections are not very helpful except to ensure that minor degrees of vertebral slippage in patients with cervical spondylosis (spinal osteoarthritis) are fixed deformities.26,27 Furthermore, muscle spasms are common in injured patients and preclude an adequate examination in the acute setting. According to the ACR, flexion/ extension radiography is best reserved for follow-up of symptomatic patients, usually in 7 to 10 days after muscle spasms have subsided. Although the use of flexion/extension radiography can provide information concerning ligament instability, MR is the procedure of choice for demonstrating this anatomy. 61 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES Table 3 Radiographic Evaluation of Adults Projection Cross-table lateral Assessments/Goals Visualize all 7 vertebral bodies and the C7-T1 junction Verify alignment of cervical spine by following 3-column model Check individual vertebrae thoroughly for obvious fracture or changes in bone density Evaluate changes in prevertebral spaces Check for fanning of the spinous processes Note abrupt changes in angles Swimmer’s lateral Visualize all 7 cervical bodies and, more importantly, the C7-T1 junction Oblique Verify proper shingling of vertebrae Note if interlaminar space between 2 continuous laminae is increased Odontoid Verify proper alignment of the lateral masses of C1 with respect to the odontoid process Check for fractures or lateral displacement Assess symmetry of the interspace between C1 and C2 Anteroposterior Verify that a straight line connects the spinous processes, thus bisecting the cervical spine Note vertical splitting of any spinous process Computed Tomography There are 3 situations in which CT is necessary: when a fracture is seen, when a fracture is suspected and when the spine is poorly visualized on plain films. When a fracture is seen on the plain films, a CT of the cervical spine that extends 1 level above to 1 level below the injury is recommended. A significant number of patients will have additional fractures in the surrounding areas that are not seen on the plain films.28 When radiography indicates a suspected fracture, patients should undergo CT. Research has shown that 22% to 42% of patients whose radiographs are inconclusive actually have fractures.28,29 In several studies, CT has been shown to effectively rule out a fracture.28-31 CT is also advantageous for areas of the cervical spine that are poorly visualized. Between 9% and 26% of patients have inadequate plain films, generally of C1-C2 and C6-C7.29,32 Schleehauf showed that 7% of those with inadequate plain films had positive CT scans.29 More importantly, in a meta-analysis of more than 1500 blunt trauma patients over a 3-year period, CT detected 100% of cervical spine injuries that were undiagnosed by inadequate plain films.30,29 The ACR recommends that patients who are not alert or conscious, are under the influence of a substance, or who have distracting injuries, cervical tenderness and 62 neurologic findings (eg, sensory and motor deficits) should have, at a minimum, a 3-projection cervical radiographic series followed by helical CT scan.20,33,34 The cervical CT examination should be performed immediately after a cranial CT scan while the patient is still in the CT suite. This is a time-effective and costeffective approach. 35 Magnetic Resonance According to EAST, an MR examination should be conducted within 8 hours for any patient presenting with a neurologic deficit. MR provides more information about the spinal cord than any other imaging study.36-38 Such information includes intrinsic compression (from edema or hematoma formation) or extrinsic compression (from disk herniation or bony fragments). MR should be reserved for patients who have clear-cut neurologic findings and for those suspected of ligament instability.39 The ACR states that MR should be used in cases of known or suspected soft-tissue injuries such as disc herniations, ligament tears, epidural hematoma and spinal cord edema or hematoma.40-42 A recent review article by Saifuddin43 goes further by recommending total spinal MR to screen for multiple noncontiguous injuries, which occur in about 20% of patients.43 MR, however, is not adequate for evaluation of bony trauma. September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING Other Cervical Spine Injuries Vertebral Artery This injury is seen in up to 11% of cervical blunt trauma patients and presents as an expanding cervical hematoma.48,49 Patients with vertebral subluxation, facet dislocations or foramen fractures are at increased risk for vertebral artery injury and probably should undergo additional imaging studies.50 Fig. 16. Flexion/extension projections. (Image courtesy of Michael Richardson, M.D., and the University of Washington Web site. Available at: www.rad.washington.edu/quickcases/cases/Case09/ text.html. Reprinted with permission.) Myelography with CT should be used in place of MR only if MR is not available and the patient cannot be safely transferred to a MR facility. The inherent risks of patient positioning required for myelography and CT exams are considerable; thus, supervised transport to an MR facility may pose less risk to the patient. Comparison of Techniques Plain Radiography vs CT Schenarts and colleagues compared the sensitivity of CT (at C1-C2) to plain-film radiography (5-projection) in blunt trauma patients.44 CT detected 96% of upper cervical fractures vs 54% detected by plain-film radiographs. Interestingly, no fractures were missed with the combination of radiography and CT. Other studies have shown similar results.45,46 Another group, Berne and associates,33 compared CT (at C1-T1) to plain-film radiography (3-projection) in similar patients over 8 months. Plain films were 61% sensitive in detecting cervical spine injury vs 90% with CT. As before, the combination of imaging techniques was 100% sensitive in detecting cervical spine injury. CT vs MR Velmahos and colleagues compared the sensitivity of CT and MR in detecting ligament injury in asymptomatic blunt trauma victims. The study revealed that isolated ligament injury without subluxation was detected in 25% of patients by CT vs 100% with MR.47 RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 SCIWORA SCI without radiographic abnormality (SCIWORA) is defined as the presence of neurologic symptoms in the absence of radiographic findings. Recent evidence suggests a higher incidence of adults presenting with SCIWORA than previously thought.51 The most common level of injury was C4. SCIWORA classically is seen in children with symptoms ranging from transient neuropathy to complete cord injury. Often a transient neuropathy will have a “lucid interval,” only to return hours or days later. The SCIWORA syndrome occurs when the elastic ligaments of a child’s neck stretch during trauma. This action causes the spinal cord to stretch, thus leading to neuronal injury or, in some cases, complete severing of the cord.52 This situation may account for up to 70% of SCI in children and is most common in children younger than 8 years. Ligament Injury Although the combination of CT and radiography is adequate to evaluate the bony spine, the issue of ligament injury needs to be addressed. On plain films these injuries may be seen on lateral projections as a misalignment of the cervical vertebrae. Unfortunately, not all ligament injuries are obvious. Symptoms include focal neck pain in the absence of radiographic findings. Nevertheless, it is important to correctly recognize the injury because missed cervical trauma in a neurologically intact patient can result in neurologic deterioration.20,53 Whiplash Mention should be made of whiplash patients, who have no radiologically demonstrable injuries and yet have a spinal sensory deficit or motor deficit. The clinical picture in whiplash injury varies greatly, ranging from simple headaches to neck pain and paresthesia in the hands. This syndrome was first described by Schneider,54 who called it a central SCI. It usually results from hyperextension trauma, such as a face-first fall down stairs or a motor vehicle accident. Evidence shows that 50% of patients recover within 6 weeks; however, recovery may take up to 3 years.55 63 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES Challenges in Evaluating the Stability of the Cervical Spine When a lateral film, such as a portable lateral c-spine image, is solely used to “clear” the cervical spine, approximately 15% of vertebral injuries are missed. In addition, plain-film studies have reported false-negative rates as high as 20% and a false-positive rate of 40%.31 Although some missed cervical fractures, subluxations and dislocations are the result of film misinterpretation, the most frequent cause of overlooked injury is an inadequate film series.19,20 Image quality becomes an important factor in a complete radiographic series, as well as obtaining the necessary projections to demonstrate all the vertebrae. Occasionally, it is impossible to fully visualize all 7 cervical vertebrae and, more importantly, the C7-T1 junction in a true lateral image. This may be due to limitations of patient mobility or, perhaps, shadow superimposition over questionable areas. A swimmer’s lateral may adequately expose these areas. If the original film series is inadequate or there are still questionable areas, the technologist may have to perform additional projections. If there is any question of an abnormality on the plain radiograph or if the patient has neck pain that seems to be disproportionate to the findings on plain films, a CT scan of the area in question should be obtained. Failure to fully demonstrate the spine has resulted in patient morbidity. Aside from inadequate film series, there are other challenges of clearing the cervical spine. For example, the patient’s neck should remain immobilized until a full cervical spine series can be obtained. However, the need for immobility often hinders completion of the series. Another imaging challenge is the radiography of uncommon cervicocranial injuries such as occipitoatlantal dissociation and atlantoaxial rotation. These conditions deserve special consideration because they are difficult to diagnose radiographically. Occipitoatlantal dissociation is the generic term that includes occipitoatlantal dislocation and occipitoatlantal subluxation. While dislocations are more common and uniformly fatal, the subluxation is less frequent, and is rarely fatal. Procedure Limitations Although they may be considered adequate to rule out a fracture, cervical spine radiographs have limitations. Reportedly, up to 20% of fractures are missed on plain radiographs.21,31,45 Many projections have unique disadvantages. The swimmer’s lateral projection 64 requires patient cooperation for positioning, which may pose a problem for the radiologic technologist. In addition, the superimposition of the clavicles, upper ribs and shoulder joints may obscure visualization of some of the vertebrae. The open-mouth odontoid projection is considered unreliable for intubated patients due to its false-negative rate of approximately 16%. In addition, artifacts caused by the teeth overlying the dens may give the appearance of a fracture through the process. If there is any question of a fracture, the projection should be repeated without the teeth in the field of view. If it is not possible to exclude a fracture of the dens, CT can be used. CT and MR imaging have limitations too. For example, fractures in the axial plane, including base of odontoid and some subluxations, may not be readily apparent with CT.56 Also, CT is excellent for identifying fractures, but its ability to show ligament injuries is limited.56 MR is used as an adjunct to plain-film radiography and CT scanning, especially to demonstrate soft tissue injury. Although MR approaches 100% sensitivity for the detection of ligament injury, there are several problems with this approach. First, there is a high falsepositive rate.57 Second, the clinical implications of many of these injuries are not yet known. Other problems with MR involve the physical nature of the procedure. Lack of availability and the time required for MR scanning limits its usefulness in the acute setting.37,58 Often, MR involves the transportation of an unstable patient to a remote part of the hospital where resuscitation is difficult. Furthermore, resuscitation equipment with metal parts may not function properly within the magnetic field generated by the MR scanner. In addition, the radiologic technologist must be aware if a patient has any metallic implants or devices, which can be difficult to determine if the patient is unconscious or unable to communicate. Diagnostic Imaging Challenges The following situations place special demands on radiologic technologists when they perform a complete radiography study for patients with cervical spine trauma: ■ Unconscious or uncooperative patients. These patients may not be able to communicate about their pain or remain still for various positions. ■ Intubated patients. The odontoid projection may be compromised in these patients. Similarly, if airway anesthesia is inadequate, conscious patients may cough or vomit when the endotracheal tube is manipulated, causing significant patient move- September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING ■ ■ ■ ■ ■ ■ ■ ment. The vast majority of cervical motion is produced at the occipitoatlantal and atlantoaxial joints. The subaxial cervical segments are displaced only minimally.59 Cervical collar problems. Not all collars are radiolucent. Area of injury. Localizing the area of injury may become a problem in several circumstances. For example, there may be multiple areas of injury that require imaging. Also, other injuries may mask a SCI and mislead the trauma team. Degenerative changes. Spondylosis is a degenerative disorder that may cause loss of normal spinal structure and function. Symptoms may mimic those of spinal injury. Pain without obvious finding. “Significant” neck pain is not defined and is determined by the treating physician. Extreme pain to 1 patient may feel like a simple itch to another. In addition, pain may be present in cases of SCIWORA, as discussed previously. Furthermore, neck pain from spondylosis is common and often mistaken for acute injury. Congenital changes. Congenital deformities of the spine are caused by anomalous vertebral development in the embryo. These changes in the spine shape and size may make it difficult to accurately assess vertebral damage. The 3 major patterns of congenital spinal deformity are hyperlordosis (exaggerated lumbar curve), kyphosis (a progressive spinal disorder that may cause a deformity described as humpback or hunchback) and scoliosis (abnormal curvature of the spine). Old injuries. Following a fracture, most vertebrae will “heal” and form a new union of bone. However, many conditions predispose bones to nonunion (eg, Down syndrome and rheumatoid arthritis). Furthermore, new trauma may be superimposed on old injuries. These old injuries may confound a diagnosis. It is important to get an accurate medical history of the patient to properly assess the injury. Adequate evaluation of the C7-T1 junction. The C7-T1 junction is a unique area that deserves much attention. It is a common site of developmental anomalies; it is a major site of arterial, lymphatic and neurologic traffic; and it is the juncture of the highly mobile cervical spine and the very limited thoracic spine. The features of the C7-T1 junction highlight the area’s importance and contribute to the difficulty of adequately visu- RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 ■ ■ ■ ■ alizing this region. Radiographs of this region are technically difficult to obtain, and in at least 26% of all trauma patients, this space is not visualized on the 3-view series.60 Swimmer’s lateral projection. If a patient’s arms are in traction, a swimmer’s lateral may have limited value. Pseudosubluxation. In physiologic misalignment caused by ligamentous laxity, pseudosubluxation can be confusing. Pseudosubluxation can occur at the C2-C3 level and, less commonly, at the C3-C4 level. Pseudosubluxation usually occurs in children, but it also may be seen in adults. Flexion-extension radiographs. A recent study noted that up to one third of all flexion/extension studies are inadequate due to limited range of motion.61 According to the ACR, flexion/extension radiographs are not very helpful except to ensure that minor degrees of vertebral slippage in patients with cervical spondylosis are fixed deformities.26,27 Furthermore, muscle spasms in acutely injured patients preclude an adequate examination in the acute setting. Additionally, cord injuries have been reported as a result of this maneuver.62 Evaluation of stability. Stability can be difficult to assess in an acutely injured patient because the degree of instability depends on several factors, including degenerative changes and the specific mechanism and location of the injury. Pediatric Considerations Children and adults have structural differences in the cervical spine. These differences can alter injury patterns and cause distinct pathology in young children. Children have more elastic intervertebral ligaments and more horizontally aligned facet joints. This anatomy predisposes them to subluxation of the cervical spine without bony injury. To further compound this problem, immature neck muscles and a proportionally large head make pediatric cervical spines act like a fulcrum and thus increase the chance of injury. As the pediatric cervical spine matures, the fulcrum effect migrates from the upper cervical levels to the lower ones until it reaches C5. Most injuries occur at the C1-C3 levels in children younger than 8 years. Other Patient Safety Considerations Emergency Procedures When a cervical spine injury is suspected, the first step in the protocol is to minimize neck movement and 65 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES further injury. The management of a patient with a potential SCI begins with the care of paramedics prior to transport. Ideally, the patient is immobilized in the neutral position on a full spine board with a cervical collar and side head supports. In addition, the shoulders and pelvis are strapped so that the neck is not the center of the body’s rotation. The patient must be treated as if the spinal column were fractured, even when there is no external evidence. If a spinal misalignment or fracture is identified, the patient should be placed in skeletal traction with tongs as soon as possible, even if no evidence of neurologic deficit exists. In addition, steroids should be administered to the patient. The use of steroids for neurologic injury has become the standard to prevent secondary causes of SCI such as swelling. According to 3 North American Spinal Cord Injury Study reports, the recommended management for patients with SCI is administration of methylprednisolone within 3 hours of injury.63-68 All in all, the number 1 treatment for spinal injury is prevention. Radiation Protection As with any radiologic study, the major overall goal is to produce high quality films without exposing the patient to excessive radiation. Collimation is important to radiographic detail and is a part of the overall practice of the ALARA (as low as reasonably achievable) principle. However, care should be taken not to collimate anatomic structures of the neck out of the radiographic image during the trauma survey. The Role of the Radiologic Technologist Education is the key to a good radiology department response to trauma. Often an emergency room physician must make a rapid initial diagnosis. Therefore, it is imperative that these studies be performed correctly and completely. Technologists should be aware of the indications for special projections of the cervical spine, including how to adequately visualize all vertebrae (especially C2 and the C7-T1 junction). Trauma imaging requires the technologist to be aware of the patient’s history and to know the sequence of diagnostic imaging. For example, a gunshot injury or stabbing may require the chest to be imaged before neck and spine imaging. But, as a rule, spine imaging is the priority for motor vehicle accidents and diving injuries. The technologist must work quickly and decisively to complete imaging while the patient is treated by the trauma team. By remaining knowledgeable about current radiographic imaging standards, the radiologic technologist is armed 66 with the proper knowledge that translates into safe quality patient care. Nowhere in radiography are the standards for imaging more important than when dealing with traumatic spine injury. References 1. The 2004 Annual Statistical Report for the Model Spinal Cord Injury Care Systems. University of Alabama at Birmingham: National Spinal Cord Injury Statistical Center; 2004. 2. Scannell G, Waxman K, Tominaga G, et al. Orotracheal intubation in trauma patients with cervical fractures. Arch Surg. 1993;128:903-906. 3. Rogers WA. Fractures and dislocations of the cervical spine: an end result study. J Bone Joint Surg Am. 1957;39:341-376. 4. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983;8:817-831. 5. Isolated fractures of the atlas in adults. Neurosurgery. 2002;50:S120-S124. 6. Jefferson G. Fracture of the atlas vertebra: report of four cases, and a review of those previously recorded. Brit J Surg. 1920;7:407-422. 7. Trafton PG. Spinal cord injuries. Surg Clin North Am. 1982;62:61-72. 8. Isolated fractures of the axis in adults. Neurosurgery. 2002;50:S125-S138. 9. Gleizes V, Jacquot FP, Signoret F, et al. Combined injuries in the upper cervical spine: clinical and epidemiological data over a 14-year period. Eur Spine J. 2000;9:386-392. 10. Management of combination fractures of the atlas and axis in adults. Neurosurgery. 2002;50:S140-S147. 11. Allen BL, Ferguson RL, Lehmann TR, et al. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine. 1982;7:1-27. 12. Harris JH Jr, Eideken-Monroe B, Kopaniky DR. A practical classification of acute cervical injuries. Orthop Clin North Am. 1986;17:15-30. 13. Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984;189:65-76. 14. Lally KP, Senac M, Hardin WD Jr, et al. Utility of the cervical spine radiograph in pediatric trauma. Am J Surg. 1989;158:540-541. 15. Rachesky I, Boyce WT, Duncan B, et al. Clinical prediction of cervical spine injuries in children. Am J Dis Child. 1987;141:199-201. 16. Laham JL, Cotcamp DH, Gibbons PA, et al. Isolated head injuries versus multiple trauma in pediatric patients: do the same indications for cervical spine evaluation apply? Pediatr Neurosurg. 1994;221-226. 17. Suspected cervical spine trauma. American College of Radiology. 2002. Available at: www.acr.org/ac_pda. Accessed May 1, 2005. September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CE ... DIRECTED READING 18. Spine trauma. American College of Radiology. 1999. Available at: www.acr.org/ac_pda. Accessed May 1, 2005. 19. Gerrelts BD, Petersen EU, Mabry J, et al. Delayed diagnosis of cervical spine injuries. J Trauma. 1991;31:1622-1626. 20. Davis JW, Phreaner DL, Hoyt DB, et al. The etiology of missed cervical spine injuries. J Trauma. 1993;34:342-346. 21. Woodring JH, Lee C. Limitations of cervical radiography in the evaluation of acute cervical trauma. J Trauma. 1993;34:32-39. 22. Spain DA, Trooskin SZ, Flancbaum L, et al. The adequacy and cost effectiveness of routine resuscitation-area cervicalspine radiographs. Ann Emerg Med. 1990;19:276-278. 23. Belaval E, Roy S. Fractures, cervical spine. eMedicine. January 9, 2005. Available at: www.emedicine.com/emerg/ topic189.htm. Accessed August 11, 2005. 24. Turetsky DB, Vines FS, Clayman DA, et al. Technique and use of supine oblique views in acute cervical spine trauma. Ann Emerg Med. 1993;22:685-689. 25. Marion DW, Domeier R, Dunham CM, et al. Practice management guidelines for identifying cervical spine injuries following trauma. Eastern Association for the Surgery of Trauma; 1998. 26. Brady WJ, Moghtader J, Cutcher D, et al. ED use of flexionextension cervical spine radiography in the evaluation of blunt trauma. Am J Emerg Med. 1999;17:504-508. 27. Dwek JR, Chung CB. Radiography of cervical spine injury in children: are flexion-extension radiographs useful for acute trauma? AJR. Am J Rentgenol. 2000;174:1617-1619. 28. Acheson MB, Livingston RR, Richardson ML, et al. Highresolution CT scanning in the evaluation of cervical spine fractures: comparison with plain film examinations. AJR. Am J Rentgenol. 1987;148:1179-1185. 29. Schleehauf K, Ross SE, Civil ID, et al. Computerized tomography in the initial evaluation of the cervical spine. Ann Emerg Med. 1989;18:815-817. 30. Borock EC, Gabram SG, Jacobs LM, et al. A prospective analysis of a two-year experience using computerized tomography as an adjunct for cervical spine clearance. J Trauma. 1991;31:1001-1006. 31. Mace SE. Emergency evaluation of cervical spine injuries: CT versus plain radiographs. Ann Emerg Med. 1985;14:973-975. 32. Nichols CG, Young DH, Schiller WR. Evaluation of cervicothoracic junction injury. Ann Emerg Med. 1987;16:640-642. 33. Berne JD, Velmahos GC, El-Tawil Q, et al. Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries. J Trauma. 1999;47:896-903. 34. Daffner RH. Cervical radiography for trauma patients: a time-effective technique? AJR. Am J Rentgenol. 2000;175:1309-1311. 35. Daffner RH. Cervical helical CT for trauma patients: a time analysis. AJR. Am J Rentgenol. 2001;177:677-679. RADIOLOGIC TECHNOLOGY September/October 2005, Vol. 77/No. 1 36. Selden NR, Quint DJ, Patel N, et al. Emergency magnetic resonance imaging of cervical spinal cord injuries: clinical correlation and prognosis. Neurosurgery. 1999;44:785-793. 37. Schaefer DM, Flanders A, Northrup BE, et al. Magnetic resonance imaging of acute cervical spine trauma: correlation with severity of neurologic injury. Spine. 1989;14:1090-1095. 38. Shepard MJ, Bracken MB. Magnetic resonance imaging and neurological recovery in acute spinal cord injury: observations from the national acute spinal cord injury study. Spinal Cord. 1999;37:833-837. 39. Vaccaro AR, Kreidl KO, Pan W, et al. Usefulness of MRI in isolated upper cervical spine fractures in adults. J Spinal Disord. 1998;11:289-293. 40. El-Khoury GY, Kathol MH, Daniel WW. Imaging of acute injuries of the cervical spine: value of plain radiography, CT, and MR imaging. AJR. Am J Rentgenol. 1995;164:43-50. 41. Kathol MH. Cervical spine trauma. What is new? Radiol Clin North Am. 1997;35:507-532. 42. Cornelius RS, Leach JL. Imaging evaluation of cervical spine trauma. Neuroimaging Clin North Am. 1995;5:451-463. 43. Saifuddin A. MRI of acute spinal trauma. Skeletal Radiol. 2001;30:237-246. 44. Schenarts PJ, Diaz J, Kaiser C, et al. Prospective comparison of admission computed tomographic scan and plain films of the upper cervical spine in trauma patients with altered mental status. J Trauma. 2001;51:663-669. 45. Kirshenbaum KJ, Nadimpalli SR, Fantus R, et al. Unsuspected upper cervical spine fractures associated with significant head trauma: role of CT. J Emerg Med. 1990;8:183-198. 46. Blacksin MF, Lee HJ. Frequency and significance of fractures of the upper cervical spine detected by CT in patients with severe neck trauma. AJR. Am J Rentgenol. 1995;165:1201-1204. 47. Velmahos GC, Theodorou D, Tatevossian R, et al. Radiographic cervical spine evaluation in the alert asymptomatic blunt trauma victim: much ado about nothing. J Trauma. 1996;40:768-774. 48. Anon. Management of vertebral artery injuries after nonpenetrating cervical trauma. Neurosurgery. 2002;50:S173-S178. 49. Biffl WL, Moore EE, Elliott JP, et al. The devastating potential of blunt vertebral arterial injuries. Ann Surg. 2000;231:672-681. 50. Wills BK, Greiner F, Orrison WW, et al. The incidence of vertebral artery injury after midcervical spine fracture of subluxation. Neurosurgery. 1994;34:435-442. 51. Hendey GW, Wolfson AB, Mower WR, et al. Spinal cord injury without radiographic abnormality: results of the national emergency X-radiography utilization study in blunt cervical trauma. J Trauma. 2002;53:1-4. 52. Grabb PA, Pang D. Magnetic resonance imaging in the evaluation of spinal cord injury without radiographic abnormality in children. Neurosurgery. 1994;35:406-414. 53. Reid DC, Henderson R, Saboe L, et al. Etiology and clinical 67 .CE . . . . . . . . . . . . . . . . . . . . . . . . . . . ........................................................................ TRAUMATIC SPINE INJURIES course of missed spine fractures. J Trauma. 1987;27:980-986. 54. Schneider RC, Kahn EA. The syndrome of acute central cervical spinal cord followed by chronic anterior cervical cord injury (or compression) syndrome. J Bone Joint Surg Am. 1960;42A:253-260. 55. Norris SH, Watt I. The prognosis of neck injuries resulting from rear-end collisions. J Bone Joint Surg Am. 1983;65B:608-611. 56. Woodring JH, Lee C. The role and limitations of computed tomographic scanning in the evaluation of cervical trauma. J Trauma. 1992;33:698-708. 57. Silberstein M, Tress BM, Hennessy O. Prevertebral swelling in cervical spine injury: identification of ligament injury with magnetic resonance imaging. Clin Radiol. 1992;46:318-323. 58. Levitt MA, Flanders AE. Diagnostic capabilities of magnetic resonance imaging and computed tomography in acute cervical spinal column injury. Am J Emerg Med. 1991;9:131-135. 59. Sawin PD, Todd MM, Traynelis VC, et al. Cervical spine motion with direct laryngoscopy and orotracheal intubation: an in vivo cinefluoroscopic study of subjects without cervical abnormality. Anesthesiology. 1996;85:26-36. 60. Kaneriya PP, Schweitzer ME, Spettell C, et al. The costeffectiveness of oblique radiography in the exclusion of C7-T1 injury in trauma patients. AJR Am J Roentgenol. 1998;171:959-962. 61. Wang JC, Hatch JD, Sandhu HS, et al. Cervical flexion and extension radiographs in acutely injured patients. Clin Orthop Relat Res. 1999;364:111-116. 62. Lewis LM, Docherty M, Ruoff BE, et al. Flexion-extension views in the evaluation of cervical-spine injuries. Ann Emerg Med. 1991;20:117-121. 63. Bracken MB, Collins WF, Freeman DF, et al. Efficacy of methylprednisolone in acute spinal cord injury. JAMA. 1984;51:45-52. 64. Bracken MB, Shepard MJ, Collins WF, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. N Engl J Med. 1990;322:1405-1411. 65. Bracken MB, Shepard MJ, Collins WF Jr, et al. Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study. J Neurosurg. 1992;76:23-31. 66. Bracken MB, Shepard MJ, Hellenbrand KG, et al. Methylprednisolone and neurological function 1 year after spinal cord injury. Results of the National Acute Spinal Cord Injury Study. J Neurosurg. 1985;63:704-713. 67. Bracken MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. JAMA. 1997;77:1597-1604. 68 68. Bracken MB, Shepard MJ, Holford TR, et al. Methylprednisolone or tirilazad mesylate administration after acute spinal cord injury: 1-year follow-up. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. J Neurosurg. 1998;89:699-706. Acknowledgement The images from the Harris & Harris Emergency Radiology Primer, found at www.uth.tmc.edu/radiology/test/ er_primer/index.html, were acquired from work supported by the John S. Dunn Research Foundation. Jennifer Minigh, Ph.D., has more than 10 years of research and teaching experience in the areas of pharmacology, toxicology, molecular genetics, signal transduction and oncology. Dr. Minigh is the director of Medical Communication Consultants and serves as secretary and immediate past-president of the Ohio Valley Chapter of the American Medical Writers Association. Reprint requests may be sent to the American Society of Radiologic Technologists, Communications Department, 15000 Central Ave. SE, Albuquerque, NM 87123-3917. © 2005 by American Society of Radiologic Technologists. September/October 2005, Vol. 77/No. 1 RADIOLOGIC TECHNOLOGY