Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
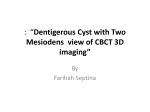
Ir J Med Sci DOI 10.1007/s11845-008-0264-6 CASE REPORT Extratesticular epidermoid cyst mimicking enlarged testis H.-W. Kao Æ C.-J. Wu Æ M.-F. Cheng Æ W.-C. Chang Æ C.-Y. Chen Æ G.-S. Huang Received: 23 September 2008 / Accepted: 4 November 2008 Ó Royal Academy of Medicine in Ireland 2008 Abstract Epidermoid cysts are benign simple epithelial tumors usually appearing as hypoechoic lesions with scattered echogenic reflectors on sonography. Herein, we present a 53-year-old man with an extratesticular epidermoid cyst in the right scrotum which shows confusing sonographic findings, normal-appearing echogenicity of the lesion and atrophied testis, which lead to a diagnostic dilemma. With a variety of sonographic presentations in extratesticular epidermoid cysts, magnetic resonance (MR) imaging could play a complementary role in difficult cases. intratesticular ones, which are the most common benign testicular neoplasms. They usually present as hypoechoic masses that are easily to be recognized and differentiated from normal testes. As an exception to the general rule, the diagnosis of our case was ambiguous until MR imaging was performed. With this case, we stress not only the importance of being familiar with various sonographic presentations of epidermoid cysts, but also the crucial role of MR imaging in challenging circumstances. Keywords Epidermoid cyst Extratesticular Magnetic resonance imaging Sonography Case report Introduction Sonography is usually the first imaging modality to investigate scrotal disorders, and it can help differentiate extratesticular lesions from intratesticular ones with very high accuracy [1]. However, the differentiation may seldom be a challenge in certain situations. The extratesticular epidermoid cysts are relatively rare, in contrast to the H.-W. Kao C.-J. Wu (&) W.-C. Chang C.-Y. Chen G.-S. Huang Department of Radiology, Tri-Service General Hospital and National Defense Medical Center, 325, Cheng-Kung Rd., Sec. 2, Taipei 114, Taiwan, Republic of China e-mail: [email protected] M.-F. Cheng Department of Pathology, Tri-Service General Hospital and National Defense Medical Center, Taipei, Taiwan, Republic of China A 53-year-old man presented with a 3-year history of painless enlargement of the right scrotum. He did not seek medical treatment until urinary difficulty developed. Clinical examination revealed a firm mass in the right scrotum, while the left scrotum was normal. Gray-scale sonography of the right scrotum showed a large solid mass with homogeneous echogenicity similar to the contralateral normal testis, findings initially been regarded as orchitis or a disseminated testicular tumor (Fig. 1). MR imaging showed a septate cyst, 9 cm in length, with homogeneous low signal on T1-weighted images and high signal on T2-weighted images (Fig. 2). The right testis was small and pushed inferomedially by the cyst. A series of laboratory examination showed normal values, including alfafetoprotein and beta-human chorionic gonadotropin. Surgical excision found a well-defined extratesticular cystic lesion without rupture. Pathologic examination depicted an epidermoid cyst lined by a stratified squamous epithelium and filled with keratinous debris (Fig. 3). The cyst showed no evidence of inflammation or infection. The final diagnosis was extratesticular epidermoid cyst. The patient was stable in 1-year follow-up. 123 Fig. 1 Axial sonography of both testes showed similar and homogeneous echogenicity with enlargement of the right (arrow) Discussion Epidermoid cysts are common benign epithelial cysts. They are well encapsulated with keratinized squamous epithelial walls and filled with sebaceous material. The lack of cutaneous adnexal structures, such as hair follicles or teeth, make epidermoid cysts different from dermoid ones [2]. They may be monolayer teratomas originating from germ cells or result from traumatic implantation of epidermal tissue into the dermis or subcutis. These are usually asymptomatic, unless they become infected, enlarged to compress adjacent structure, or rupture [3]. Extratesticular epidermoid cysts are usually subcutaneous and frequently located at the median raphe from the distal penis to the anus [4]. In the scrotum, they should be differentiated from other paratesticular lesions, including cystic and solid ones such as spermatocele, complex cyst, or rhabdomyosarcoma. On sonography, epidermoid cysts most often appeared as hypoechoic masses with scattered reflectors and posterior sound enhancement but no color Doppler signals. However, the echogenicity of the cysts may vary widely from anechoic to heterogeneous solid appearing, depending on their content [5]. They may be ovoid, spherical, lobulated or tubular in shape. In our case, the echogenicity of the cyst was unique in that it simulated the normal testis. Furthermore, the large size of the cyst and the atrophic 123 Fig. 2 Axial MR imaging of the scrotum demonstrated a large cystic lesion (thick arrow) in the right scrotum with low signal and no contrast enhancement on T1-weighted images (a) and high signal on T2-weighted images (b). The atrophic testis (thin arrow) was pushed inferomedially testis hidden below made the sonographic diagnosis even more challenging. In this circumstance, color Doppler ultrasound may help to differentiate true solid lesions from the solid-appearing ones by the presence of blood flow [6]. But it should be noticed that some ruptured epidermoid cysts also have color Doppler signals inside [5]. Ultimately, the sonographic findings are not specific and surgical exploration is required. MR imaging, in some situations like ours, may provide more supportive findings of epidermoid cyst [3]. It typically appears as a well-defined mass with low signal on T1-weighted images and high signal on T2-weighted images. There may be low-signal-intensity foci in the cyst, representing keratin debris, and no contrast enhancement. Furthermore, MR imaging can depict the atrophic testis which may be missed on sonography. In our case, the valuable information of MR imaging did lead to correct preoperative diagnosis which helps a lot in treatment and surgical planning. In conclusion, we presented a pitfall of sonography in diagnosing and extratesticular epidermoid cyst, and stressed the value of MR imaging in this clinical dilemma. References 1. Kim W, Rosen MA, Langer JE, Banner MP, Siegelman ES, Ramchandani P (2007) US MR imaging correlation in pathologic conditions of the scrotum. Radiographics 27(5):1239–1253. doi: 10.1148/rg.275065172 2. Dilworth JP, Farrow GM, Oesterling JE (1991) Non-germ cell tumors of testis. Urology 37(5):399–417. doi:10.1016/0090-4295 (91)80100-L 3. Cho JH, Chang JC, Park BH, Lee JG, Son CH (2002) Sonographic and MR imaging findings of testicular epidermoid cysts. AJR Am J Roentgenol 178(3):743–748 4. Picanco-Neto JM, Lipay MA, D’Avila CL, Verona CB, ZeratiFilho M (1997) Intrascrotal epidermoid cyst with extension to the rectum wall: a case report. J Pediatr Surg 32(5):766–767. doi: 10.1016/S0022-3468(97)90030-0 5. Lee HS, Joo KB, Song HT, Kim YS, Park DW, Park CK et al (2001) Relationship between sonographic and pathologic findings in epidermal inclusion cysts. J Clin Ultrasound 29(7):374–383. doi:10.1002/jcu.1052 6. Langer JE, Ramchandani P, Siegelman ES, Banner MP (1999) Epidermoid cysts of the testicle: sonographic and MR imaging features. AJR Am J Roentgenol 173(5):1295–1299 Fig. 3 Bilobed specimen showed a well-capsulated lesion with white keratin content (a). Pathologic examination (b, H&E, 9100) depicted a typical picture of epidermoid cyst with stratified squamous epithelial walls (thick arrow) and keratin (thin arrow) 123