Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
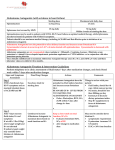
Doncaster & Bassetlaw Medicines Formulary Section 2.2.1: Thiazides and Related Diuretics Indapamide 2.5mg Tablets Metolazone 5mg Tablets Section 2.2.2: Loop Diuretics Furosemide 20mg, 40mg and 500mg Tablets Furosemide 40mg in 5ml Liquid Furosemide 20mg in 2ml Injection Furosemide 80mg in 8ml Injection Furosemide 250mg in 25ml Injection Bumetanide 1mg and 5mg Tablets Bumetanide 1mg in 5ml Liquid Bumetanide 1mg in 2ml Injection 2.2.3: Potassium Sparing Diuretics and Aldosterone Antagonists Spironolactone 25mg and 100mg Tablets Spironolactone 5mg in 5ml Suspension [UL] Spironolactone 25mg in 5ml Suspension [UL] Spironolactone 100mg in 5ml Suspension [UL] Eplerenone 25mg and 50mg tablets Amiloride 5mg Tablets Amiloride 5mg in 5ml Solution 2.2.5: Osmotic Diuretics Mannitol 10%, 20% Infusion 500ml Approved by Drug and Therapeutics Committee: September 2014 Reviewed Date: September 2017 KEY: [UL] Unlicensed Preparation; Drug – first line choice; Drug – hospital only; Drug – Amber (TLS), Drug – Red (TLS), see http://medicinesmanagement.doncasterpct.nhs.uk/ Prescribing Guidance: Thiazide Diuretics: Bendroflumethiazide should not now be initiated for the management of hypertension. Indapamide (2.5mg each morning) should be prescribed in preference. NICE Guidance (Hypertension): Diuretics are not preferred as routine initial therapy for hypertension. However, they may be considered for older people for whom calcium channel blockers are not suitable, for example because of oedema or intolerance or if there is evidence of heart failure or a high risk of heart failure. Where a diuretic is initiated this should be indapamide. From NICE Clinical Guideline 127 (via http://www.nice.org.uk/cg127) Prescribing outside this formulary should only take place via a New Product Request Metolazone should only be used in resistant oedema where large doses of loop diuretics have been used. It is a powerful synergist with loop diuretics and can produce a diuresis in patients with severely impaired renal function (creatinine clearance of less than 20mls/min). When combined with a loop diuretic, the dose should not normally exceed 5mg in the morning. A dose of 2.5mg two or three times a week can often be effective. The dose should be titrated against weight loss and renal function as appropriate. When there are problems obtaining metolazone (unlicensed preparation), bendroflumethazide can be viewed as a therapeutic alternative: http://www.bsh.org.uk/latest-news/metolazone-withdrawal/ Loop Diuretics: First line – Furosemide Second line – Bumetanide Loop diuretics are indicated for heart failure and oliguria secondary to acute renal failure. Furosemide is the drug of choice because it is considerably cheaper in the community. Bumetanide should be reserved for patients intolerant of or unresponsive to increasing doses of furosemide. Furosemide 40mg is roughly equivalent to bumetanide 1mg. However, with higher doses of furosemide, the ratio of 1 to 40 may not be appropriate (lower doses of bumetanide than the ratio suggests should be used) and the dose titrated according to symptoms. Oral Dosage: Use in Oedema: Furosemide – initially, 40mg increased according to clinical response Bumetanide – initially, 1mg increased according to clinical response Intravenous Administration: Furosemide, at doses exceeding 80mg, should be given at a rate not exceeding 4mg/minute Bumetanide should be given at a rate not exceeding 1mg/minute IV and oral doses are not equivalent and this should be considered when converting from IV to oral furosemide. The oral bioavailability of furosemide is approximately 50% and this may be further reduced in oedematous patients. Prescribing outside this formulary should only take place via a New Product Request Potassium Sparing Diuretics: Use in Heart Failure: From NICE Clinical Guideline 108 (via http://www.nice.org.uk/cg108) Prescribing outside this formulary should only take place via a New Product Request Spironolactone is the potassium-sparing diuretic of choice for all patients who have developed (or are at risk of developing) hypokalaemia, secondary to a diuretic used for the treatment of heart failure. However, if the potassium levels have not fallen severely, prescribing an ACE inhibitor – where not already prescribed – may be a better therapeutic option (providing there are no contra-indications). When used in heart failure, the dose of spironolactone is 25mg daily, halved if potassium levels rise above 5.5mmol/l. The drug should be stopped where hyperkalaemia persists despite this dose reduction. Spironolactone should also be stopped if potassium levels rise above 6.0mmol/l or if a significant deterioration in renal function is noted. On consultant advice, doses of 50mg daily can be used if heart failure deteriorates and there are no issues with hyperkalaemia. Use Post STEMI: Long-term aldosterone blockade should also be prescribed in STEMI patients who are already receiving therapeutic doses of ACE inhibitor with an ejection fraction of less than 40% and either symptomatic heart failure or diabetes. Monitoring of Spironolactone: Potassium levels must be monitored prior to starting therapy with spironolactone at baseline, after 1, 4, 8 and 12 weeks, then 3 monthly for the first year and 6 monthly thereafter. Patients with impaired renal function function or those with potassium levels at the higher end of the usual range are at greater risk of developing hyperkalaemia and indeed patients with hyperkalaemia should not be started on aldosterone antagonists. Patients (particularly male patients) should be monitored for signs of gynaecomastia, which may affect up to 9% of patients. If this develops, spironolactone should be discontinued and use of eplerenone as an alternative aldosterone antagonist considered. Combination with an ACE Inhibitor: Aside from where spironolactone is clinically indicated for heart failure (above), potassium-sparing diuretics should only be used if significant hypokalaemia develops, or in patients at risk of developing hypokalaemia. Spironolactone is also used for the treatment of primary hyperaldosteronism, and oedema and ascites in hepatic cirrhosis. The dosage for these indications is 100 to 200mg daily, increasing gradually to 400mg daily where required. Eplerenone is the second line formulary aldosterone antagonist for: Prescribing outside this formulary should only take place via a New Product Request Heart failure patients who remain moderately to severely symptomatic despite already receiving a diuretic and appropriately titrated doses of an ACE inhibitor and a beta blocker Post STEMI in patients already receiving therapeutic doses of ACE inhibitor with an ejection fraction of less than 40% and either symptomatic heart failure or diabetes It should be used as an alternative to spironolactone in those patients intolerant to, or unsuitable for, spironolactone therapy (usually due to gynaecomastia – which is more common with spironolactone) As with spironolactone patients with impaired renal function or those with potassium levels at the higher end of the usual range are at greater risk of developing hyperkalaemia. Indeed patients with hyperkalaemia (or those with a creatinine clearance < 50ml/min) should not be started on eplerenone. Treatment with eplerenone should be initiated at 25mg daily and titrated to the target dose of 50mg once daily within 4 weeks. Potassium levels must be monitored prior to starting therapy with eplerenone at baseline, after 1, 4, 8 and 12 weeks, then 3 monthly for the first year and 6 monthly thereafter. After initiation, the dose should be adjusted based on the serum potassium level as shown in the table below: Serum potassium (mmol/L) Action Dose adjustment < 5.0 Increase 25 mg on alternate days to 25 mg OD 25 mg OD to 50 mg OD 5.0 – 5.4 Maintain No dose adjustment 5.5 – 5.9 Decrease 50 mg OD to 25 mg OD 25 mg OD to 25 mg alternate days 25 mg on alternate days to withhold > 5.9 Withhold N/A Eplerenone is licensed only in addition to standard therapy to reduce cardiovascular risk in stable patients with left ventricular dysfunction and clinical evidence of heart failure following recent myocardial Infarction. Prescribing outside this formulary should only take place via a New Product Request Significant pharmacokinetic interaction can occur resulting in large increases in eplerenone concentration when eplerenone is co-administered with strong CYP3A4 inhibitors such e.g. clarithromycin or ketoconazole. Coadministration of these agents is contra-indicated. Amiloride: Given the evidence backing the use of spironolactone in heart failure (although only in NYHA class III and IV patients), amiloride should now only be used in those patients who are prescribed potassium sparing diuretics for indications other than heart failure. A course of amiloride may often be sufficient (e.g. 3 to 5 days), after which the potassium level can be checked and the drug stopped if appropriate. Where clinically indicated, amiloride should be added as a separate drug to increase flexibility. Combination products (e.g. Co-Amilofruse 5/40) should not be used unless compliance is considered to be a significant problem. Mannitol: For raised intracranial pressure: Administered by intravenous infusion over 30 to 60 minutes at a dose of 0.25 to 2g/kg, usually using a 20% mannitol solution (20% ≡ 0.2g/ml). Central administration is preferred as extravasation can cause skin necrosis, thrombophlebitis and oedema. Infusion sets should incorporate an in-line filter. For the oliguric phase of renal failure or those suspected of inadequate renal function after correction of plasma volume: A test dose of 0.2g/kg should be administered by infusion using a 20% solution over 5 minutes. Providing this produces a diuresis of at least 30 to 50ml/hour over the next 2 to 3 hours further doses can be given. The usual dose ranges from 50 to 100g* in a 24-hour period of either a 10% or 20% solution (20% solution ≡ 0.2g/ml, 10% solution ≡ 0.1g/ml, therefore *100g ≡ 500ml Mannitol 20% solution). The dose is adjusted to maintain urine flow at 30 to 50ml/hour. If the initial test dose delivers an inadequate response one further test dose can be tried. Central administration is preferred as extravasation can cause skin necrosis, thrombophlebitis and oedema. Infusion sets should incorporate an in line filter. Prescribing outside this formulary should only take place via a New Product Request Adverse effects: The most common adverse effect is fluid and electrolyte imbalance. The shift in fluid from intracellular to extracellular can cause tissue dehydration and dehydration of the brain particularly in patients with renal failure. All patients on mannitol should be carefully monitored for signs of fluid and electrolyte imbalance and renal function closely monitored. Note that infusions may crystallise at low temperatures. The crystals can be dissolved before administration by gently warming to room temperature. Prescribing outside this formulary should only take place via a New Product Request