Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
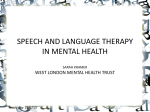
ROYAL BERKSHIRE HOSPITAL Report Type Self Assessment Trust Guide National Benchmark Position: Key Overall Compliance (% score) ● ● ● ROYAL BERKSHIRE NHS FOUNDATION TRUST Service This service Highest Performing Team Lowest Performing Team Performance range for the majority urology specialist cancer services Urology Specialist Team Measures ———— National middle score Publication Date 3rd July 2015 This benchmark is based on the 48 urology specialist cancer services who have completed their assessment in 2015-2016 Quality and Performance Summary Overall Compliance Serious Concerns and Immediate Risks A Serious Concern was identified when the service was last assessed 86% Self Assessment SEE BELOW FOR PROBLEM RESOLUTION No assessment took place in 2014-15 cycle 2015 Patient Experience Survey National Tumour Results Patient understood what was wrong Easy to contact CNS Patient had confidence in doctors Patient contact post discharge Patient given enough care The Service has a complete team Members cover all relevant disciplines. 76% 85% 84% 90% 44% Trust Results 2015 Patient Experience Survey Trust Tumour Results Given complete explanation Patient told sensitively Treatment options explained Patient involved in decisions Taking part in research discussed Waiting Times for Trust - All Cancer Services April - June 2016 71% 89% 91% 81% 12% Any queries please contact [email protected] Treated in targeted time 2 Weeks 31 Days 62 Days 92% 98% 82% www.mycancertreatment.nhs.uk Structure and function of the service Measure There is a lead clinician and the core team includes all relevant members Each role needs to attend 95% of the MDT meetings MDT will discuss the treatment plan of all patients All MDT core members attend two thirds of the meetings There are additional members who don't need to attend as part of the core team Operations and post operative care take place on a single hospital site Surgeons meet the required minimum workload The MDT discusses the reuired number of patients a year Met Y N Y Y Y N N Y The MDT is led by Mr Adam Jones, Consultant Urological Surgeon. 2013 was a difficult year for the local MDT members with regard to their SMDT input. The RBH local MDT raised concerns at the SMDT peer review in 2013 and as a result the SMDT was put on immediate risk. Since then one of the RBH consultants has relocated and the 2 senior WPH consultants have resigned. Everyone agrees that the SMDT is now functioning very well. The MDT has a complete and diverse core and extended membership. Improvements this year have included the very successful repatriation of WPH cystectomies to the RBH site, the successful introduction of robotic cystectomy and robotic partial nephrectomy and excellent National Cancer Patient Experience Survey results. All major cancers are covered by at least two consultant members. The four CNS and one Macmillan sponsored nurse practitioner provide comprehensive supportive services to patients greatly enhancing the quality of their holistic care. The MDT meets every Wednesday morning from 8.00am until 9.30am. The first part of the meeting is devoted to the sMDT and then the other local cases. Last year only one meeting was cancelled because of the British Association of Urological Surgeons annual meeting. All core members attended at least 66% as evidenced by the weekly attendance records of the meetings. An annual operational meeting is held (last meeting June 18th 2014) and the operational policy is continuously evolving. The 2 week and 31 day targets were met last year and the 62 day target was only very narrowly missed. (see below). Two week wait 94.3% (Target 93 %) Thirty one day wait 97.5% (Target 96 %) Sixty two day wait 83.2%. (Target 85 %) Any queries please contact [email protected] www.mycancertreatment.nhs.uk 807 cases have been discussed at the MDT of which 389 were new cases. 969 Two-week-wait flexible cystoscopies have been performed. 301 Two-week-wait trus biopsies of the prostate have been performed. Members of the MDT participate actively in the sMDT and also the PbODG (provider based operational delivery group) the successor of the network TSSG meetings. Coordination of care/patient pathway Measure Network agreed clinical guidelines are in place There is a regular clinic for patients for prostate There is a regular clinic for patients with blood in their urine Patients are encouraged to discuss their treatment options with the MDT Network-agreed patient pathways are specified MDT agrees an individual patient's treatment plans Lead clinician attends at least two thirds of the network group meetings Met Y Y Y Y Y Y Y The MDT chairman ensures the role of the MDT is in full accordance with guidelines Network guidelines are contributed to (i.e. this year the RBH MDT were responsible for updating the guidelines with respect to prostate cancer) and these guidelines, are based on those laid out by the European Association of Urology. MDT discussions are recorded as formal minutes and a copy of patient consultation letters are offered to all patients. All new patients with a diagnosis of urological cancer are discussed in the MDT (irrespective of age and stage of disease). All patients who fulfil the criteria for sMDT discussion under IOG are referred to that meeting. All patients are allocated a named key worker and a written confirmation of this is placed in the patients notes. Patient Experience Measure A key worker is in place MDT provides written material for patients and carers The patient is offered a record of the consultation MDT looks at patient feedback in the last two years and act on at least one point Met Y Y Y Y The RBFT are a national site for the enhanced recovery programme. The urology team runs a very active Any queries please contact [email protected] www.mycancertreatment.nhs.uk prostate and a separate bladder cancer support group and this year we are planning to introduce a kidney cancer support group. Support group initiatives include arranging meetings with patients who have previously undergone treatment and also for prostate cancer visiting the department to specifically look at the robot and brachytherapy set ups. Many members of the support group are now active fundraisers for us. Specific service improvements relating to patient experience have included; The introduction of a one stop cystectomy clinic for patients referred from WPH. We appreciate that although single site surgery is an IOG requirement, it does have some inconvenience to patients coming from WPH so for those patients we have introduced a dedicated clinic where they meet the surgical and anaesthetic team, the local CNS team, stoma therapists, pre-operative clerking and visit the ward all in one visit. This is the 3rd successive year that RBH has scored highest of all the Thames Valley urology departments in the National Cancer Patient Experience Survey. Highlights included Q 15 Patient given a choice of different types of treatment? RBH 96 % (nat ave 91 %). Q21 Patient given the name of the CNS in charge of their care? RBH 98 % (nat ave 88 %). Q38 Patient had confidence and trust in all doctors treating them? RBH 96% (nat ave 87 %). Examples of ‘anything good?’ responses in the National Cancer Survey include; “During my stay in RBH and follow up appointments, I have always been treated with the utmost respect and dignity by both doctors and nurses, also HCA”. “I receive very personal attention in a friendly and welcoming environment. I do not believe I would have been similarly treated elsewhere except, perhaps at the Royal Marsden Hospital. Hence I am reluctant to move away from the Reading area” “My care and treatment has been first class at all times”. “Yes. From initial GP referral to surgery was just 3 weeks. Most impressive. I was seen by a hospital doctor who referred me for a CT scan. I was then seen by another doctor in urology who notified me of the diagnosis and arranged for me to undergo surgery just less than one week later during which period, I underwent pre-op assessment. The speed and efficiency with which I was treated was beyond my wildest expectation. Absolutely first rate”. Areas where we were below national average have been discussed at an operational meeting and addressed in the work plan Any queries please contact [email protected] www.mycancertreatment.nhs.uk Clinical Outcomes Measure MDT reviews clinical indicators and/or audit data each year and discuss at the network meeting MDT produces an annual report on clinical trials and discuss with the network group Met Y Y In this year the team have performed 68 nephrectomies and partial nephrectomies, 67 radical prostatectomies and 33 radical cystectomies. The team have also completed 56 surgical prostate brachytherapy procedures. There has been one death after a prostatectomy and one death after a cystectomy. 100% of new cases were discussed at the MDT or sMDT and 100% of new cases see a CNS prior to their treatment. National database and local audits have demonstrated very good results; 1. Nephrectomies : BAUS national audit data shows that compared to national average the RBH rates of 1. complications, 2. transfusions, 3. mortality are all lower than national average. Furthermore these results are achieved with a case mix that appears more difficult than average. For RBH patients WHO performance status >=2 is 66 % compared to 10 % nationally. Patient age > 70 is 36 % (30 % Nationally) and below normal Hb pre-op 42 % vs 33 % nationally. The median LoS is 3d ( 4d nationally). 2. Prostates; BAUS data shows that RBH is at the higher end of the distribution for numbers of procedures performed. T2 positive margin rates are regarded as a marker of technical proficiency. The national average is 13.5%. RBH rates are around 10 % (full audit in process). 3. Partial nephrectomies. Since changing from open partial nephrectomies to robotic in April 2014 there has been 1. Less blood loss 400 ml vs 620 2. Less reduction in post op renal function. 3. Reduced length of stay 3.5 d vs 6.5d and 4 . Greater proportion with no complications (Clavian 0 ) 75 % vs 55% 4. Cystectomy since repatriation (April –Dec 2014 including robotic cases). 1. < 500 ml blood loss 72% (nat ave 23 %). 2. Not transfused 89% (nat ave 43 %). 3. Average LN count 22 (nat ave 8). 4. Average Length of Stay 6 (nat ave 15). 5. Cystectomy patient satisfaction survey since repatriation (initial results n =14). 1. Were you involved as much as you wanted to be in decisions about your care and treatment? Yes, definitely 93% 2. Did you have confidence and trust in the doctors treating you? In all of them 93 %, In some of them 7%. 3. Were you able to discuss any worries or fears with staff during your hospital visit? As much as I wanted 93%. The team have an ongoing prospective data collection programme on all major surgery and review Any queries please contact [email protected] www.mycancertreatment.nhs.uk complications according to the Clavian system. There is always a trials nurse at the MDT meeting and the team actively recruits to national trials including RADICALS, STAMPEDE, GENETICS study as well as undertaking local trials in collaboration with pharmaceutical companies e.g. Enthuse. STAMPEDE Pt approached 18 Pt recruited 4 RADICALS Pt approached 3 Pt recruited 1 UK Genetics Prostate cancer Pt approached 22 Pt recruited 7 UK Genetics Testicular cancer Pt approached 21 Pt recruited 12 Good Practice The major achievement of 2014 has been the improved IOG compliance with a very successful repatriation of cystectomies to RBH. Coupled with this and following personnel changes the SMDT is now a well functioning unit. In addition highlights included; • Passed case number 650 in brachytherapy • Excellent National Cancer Patient Experience Survey results (best in Thames Valley for third year running) • Continued development of RFA as a treatment option for small kidney tumours. • Introduction of robotic cystectomy and robotic partial nephrectomy. • Successful incorporation of Mr Paul Hadway as new cancer consultant Any queries please contact [email protected] www.mycancertreatment.nhs.uk Immediate Risks No Immediate Risk was identified Serious Concerns Cystectomies are now done at a single site and work is in progress for prostatectomies to move across to RBFT for a 6 month period. Whilst it is recognised that this is improving, it remains a serious concern until all urological cancer surgery is done at a single site. No Serious Concern Resolution was identified Other Concerns General Comments No general comments given. Any queries please contact [email protected] www.mycancertreatment.nhs.uk