Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
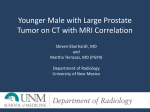
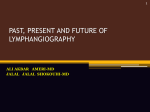
CERVICAL LYMPH NODE ENLARGEMENT ON THE RIGHT SIDE AS THE INITIAL MANIFESTATION OF METASTATIC PROSTATE CANCER international section 859 20 Arch. Esp. Urol., 56, 7 (859-861), 2003 Cervical lymph node enlargement on the right side as the initial manifestation of metastatic prostate cancer. ABDURRAHMAN ÖZGÜR, YALÇIN ILKER, LEVENT N. TÜRKERI. Marmara University School of Medicine Department of Urology. Summary.- OBJECTIVES: Cervical lymph node enlargement (LAP) due to metastatic spread is an uncommon manifestation of prostatic adenocarcinoma. In case of non-regional lymphatic spread, left supraclavicular region was found to be the most common site (1,2,3) whereas right sided metastatic lymph node involvement has been extremely uncommon. METHODS: We here in describe a case of a 75 year-old man who had an enlarged cervical lymph node for a year which subsequently proved to be involved by metastatic adenocarcinoma of the prostate. CONCLUSIONS: Although, prostate cancer rarely metastasize to the cervical lymph node chain it should always be considered in the differential diagnosis of metastatic lymph node enlargement in the cervical area of elderly men. Keywords: Prostatic neoplasms. Lymph node metastasis. Resumen.- OBJETIVOS: La adenopatía cervical secundaria a diseminación metastásica es una manifestación poco frecuente del adenocarcinoma prostático. En los casos de diseminación linfática extraregional, la región supraclavicular izquierda es la localización más frecuente (1, 2,3) mientras que las adenopatías derechas han sido extremadamente raras. MÉTODOS Y RESULTADOS: Describimos el caso de un varón de 75 años que presentaba una adenopatía cervical de un año de evolución que se demostraría posteriormente que era secundaria a una metástasis de adenocarcinoma prostático. CONCLUSIONES: Aunque el cáncer de próstata rara vez metastatiza en la cadena linfática cervical, debería siempre considerarse en el diagnóstico diferencial de los casos de adenopatías metastáticas del área cervical en ancianos. Palabras clave: Neoplasias prostáticas. Metástasis linfáticas. INTRODUCTION Address correspondence to: Levent N. Türkeri, M.D. Marmara University School of Medicine Turkey E-mail: [email protected] Accepted for publication January 20, 2003. Prostate cancer is the most common cancer diagnosed in men. Bone is the most common metastatic site in this tumor and the presence of soft tissue or visceral metastases is uncommon. In case of non-regional lymphatic spread, left supraclavicular region was found to be the most common site (1, 2, 3) whereas right sided metastatic lymph node involvement has been extremely uncommon. 860 ABDURRAHMAN ÖZGÜR, YALÇIN ILKER AND LEVENT N. TÜRKERI DISCUSSION Fig. 1. CASE REPORT A 75 year old man presented with a right-sided cervical mass with a duration of one year and cervical needle biopsy revealed metastatic adenocarcinoma in August 2000. In January 2001 he had lumbar and right flank pain. Abdominal ultrasound examination at that time revealed grade 4 hydronephrosis on the right side, para-aortic lymph node enlargement (LAP) measuring 16x8 mm and prostatic indentation to the bladder. Consequently, he was referred to a urologist and his serum PSA level wasmeasured1399ng/ml.Transrectalultrasoundguided biopsy of the prostate revealed adenocarcinoma of the prostate with a Gleason score of 8 (4+4) and perineural invasion was observed. Bone scintigraphy revealed multiple metastases and a non visualized right kidney. Subsequently, maximal androgen blockade therapy with an LHRH agonist and Bicalutamide was initiated. Seven months after the therapy the PSA level decreased to 53.4 ng/ml, without any significant change in the cervical LAP which was measuring 6.5x7.5 cm. In November2001,thepatient’scervicalLAPwasenlarged to 8x8.5 cm (Figure-1, 2), and his PSA level was > 400 ng/ml. At this point bicalutamide was discontinued and Estracyt + Mitoxantrone + Vinorelbine chemotherapy was initiated. At one month follow up of this therapy PSA level was down to 253 ng/ml and the size of the cervical LAP was decreased to 8x7 cm. Prostate cancer is the most common cancer diagnosed in men. Through the use of digital rectal examination, prostate specific antigen (PSA) and biopsy it is now possible to diagnose prostate cancer at an earlier stage. The most common metastatic site of prostate cancer is bone. Rarely, metastases are found in non-regional supradiaphragmatic lymph nodes, most commonly the leftsupraclaviculargroup,whereasrightsidedmetastatic lymph node involvement has been extremely uncommon (1, 2, 3). Most metastatic cancers to the cervical lymph nodes are from primary head and neck cancers involving the mucosal surfaces of the upper aero digestive tract (4). Our patient presented with a right sided cervical LAP which is an uncommon metastatic site for prostate cancer. Initial hormonal therapy with LHRH agonist andbicalutamidewasselectedasthetreatment.However, the response to maximal androgen blockade therapy was incomplete and of a short duration. As a second line therapy combination chemotherapy was started. Which resulted in a reduction of both serum PSA level to 253 ng/ml and the size of the metastatic lesion to 8x7 cm. Although, current literature indicates that the location or number of soft tissue metastases did not influence the response rate and survival of these patients is reported to be no different from those with skeletal metastases alone (2), our patient had a poor clinical response to Fig. 2. CERVICAL LYMPH NODE ENLARGEMENT ON THE RIGHT SIDE AS THE INITIAL MANIFESTATION OF METASTATIC PROSTATE CANCER hormonal therapy. Therefore, if the initial response to hormonal therapy is limited, it appears to be useful to continue treatment in combination with chemotherapeutic agents until more effective new treatment modalities are developed. REFERENCES AND RECOMMENDED READING (*of special interest, **of outstanding interest) **1. CHITALE, S.V.; HARRY, L.; GACHES, C.G.C.: "Presentation of prostatic adenocarcinoma with cervical 861 lymphadenopathy: Two case reports and review of the literature."Otolaryngology-HeadandNeckSurgery,October 2001. *2. SAETER, G.; SOPHIE, D.F.; OUS, S.: "Carcinoma of the prostatewithsofttissueornon-regionallymphaticmetastases at the time of diagnosis: a review of 47 cases." Br. J. Urol., 56: 385, 1984. 3. CHO, K.R.; EPSTEIN, J.I.: "Metastatic prostatic carcinoma tosupradiaphragmaticlymphnodes.Aclinicopathologicand immunohistochemical study." Am. J. Surg. Pathol., 11: 457, 1987. 4. BENJAMIN, C.J.; MADISON, C.; AMISH, S., et al.: "Prostate carcinoma metastatic to the cervical lymph nodes: Report of two cases and review of the literature." Am. J. Otolaryngol., 22: 420, 2001.