Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
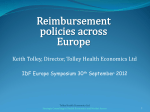
0021-972X/04/$15.00/0 Printed in U.S.A. The Journal of Clinical Endocrinology & Metabolism 89(6):2756 –2762 Copyright © 2004 by The Endocrine Society doi: 10.1210/jc.2003-031780 Comparison of Efficacy of Spironolactone with Metformin in the Management of Polycystic Ovary Syndrome: An Open-Labeled Study M. ASHRAF GANIE, M. L. KHURANA, M. EUNICE, M. GULATI, S. N. DWIVEDI, AND A. C. AMMINI Departments of Endocrinology and Metabolism (M.A.G., M.L.K., M.E., A.C.A.), Radiology (M.G.), and Biostatistics (S.N.D.), All India Institute of Medical Sciences, New Delhi 110029, India We compared the efficacy of spironolactone (50 mg/d) with metformin (1000 mg/d) after random allocation in 82 adolescent and young women with polycystic ovary syndrome (PCOS) on body mass index (BMI), waist-to-hip ratio, blood pressure, menstrual cyclicity, hirsutism, hormonal levels, glycemia, and insulin sensitivity at baseline and at the 3rd and 6th months of treatment. Sixty-nine women who completed the follow-up had a mean age of 22.6 ⴞ 5.0 yr and mean BMI of 26.8 ⴞ 4.0 kg/m2. The number of menstrual cycles in the spironolactone and metformin groups increased from 6.6 ⴞ 2.1 and 5.7 ⴞ 2.3 at baseline to 9.0 ⴞ 1.9 and 7.4 ⴞ 2.6 at 3rd month and to 10.2 ⴞ 1.9 and 9.1 ⴞ 2.0/ year at the 6th month (P ⴝ 0.0037), respectively. The hirsutism score decreased from T HE POLYCYSTIC OVARY syndrome (PCOS), a heterogeneous disorder, is characterized by oligo-anovulation, menstrual disturbances, and androgen excess. The disorder, first described by Stein and Leventhal (1), is now believed to be the most common hormone condition affecting reproductive age group women (2, 3). Earlier, most of the therapeutic modalities were devised to antagonize or decrease androgen production (ovarian wedge resection, ovarian suppression by estrogen and progesterone, LHRH analogs, or antiandrogens), because androgen excess is the most common abnormality detected in these subjects (4 – 6). For the last two decades many authors have shown that insulin resistance and the consequent hyperinsulinemia is the driving factor for increased androgen production (7–12). The insulin resistance has been demonstrated in nonobese women even at younger ages (7, 9). This has been used as a rationale for using insulin sensitizers such as metformin (13– 18) and thiazolidinediones (19 –21) in the management of PCOS. Metformin improves insulin sensitivity and various aspects of glucose homeostasis such as reduction in enteral glucose absorption, inhibition of gluconeogenesis, and increase in glucose utilization in muscle and fat (22). In women Abbreviations: AUC-I, Area under the curve for insulin; BMI, body mass index; BP, blood pressure; DHEAS, dehydroepiandrosterone sulfate; FGIR, fasting glucose/insulin ratio; HOMA, homeostasis model assessment; IGT, impaired glucose tolerance; OGTT, oral glucose tolerance test; PCOS, polycystic ovary syndrome; PRL, prolactin; WHR, waist-to-hip ratio. JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the endocrine community. 12.9 ⴞ 3.2 and 12.5 ⴞ 4.9 at baseline to 10.1 ⴞ 3.1 and 11.4 ⴞ 4.1 at the 3rd month and to 8.7 ⴞ 1.9 and 10.0 ⴞ 3.3 at the 6th month, respectively. Both groups showed improvement in glucose tolerance and insulin sensitivity, although the metformin effect was significant in the latter. Serum LH/FSH and testosterone decreased in both groups. BMI, waist-to-hip ratio, and blood pressure did not change with either drug. We conclude that both drugs are effective in the management of PCOS. Spironolactone appears better than metformin in the treatment of hirsutism, menstrual cycle frequency, and hormonal derangements and is associated with fewer adverse events. (J Clin Endocrinol Metab 89: 2756 –2762, 2004) with PCOS, many authors have demonstrated the efficacy of metformin in improving menstrual cycle pattern (13, 17, 18, 23), ovulation (24 –28), cervical scores (27), and pregnancy outcomes (15). Although these effects are attributed to enhanced insulin sensitivity, metformin has also been shown to directly inhibit human thecal cell androgen synthesis, suggesting an insulin-independent mechanism (29, 30). Recently published meta-analyses including 12 controlled and 16 uncontrolled trials demonstrated a beneficial effect of metformin on menses and spontaneous or clomiphene citrateinduced ovulation (31). A subsequent systemic review of 13 randomized controlled trials also suggested a significant effect of metformin on various components of PCOS such as fasting insulin levels, low-density lipoprotein cholesterol, blood pressure (BP), ovulation, and pregnancy rates with little or no effect on body mass index (BMI) and waist-to-hip ratio (WHR). Nausea, vomiting, and other gut disturbances were noted as major adverse effects (18, 32). Spironolactone is a steroid chemically related to the mineralocorticoid aldosterone. The drug is primarily used as a diuretic by virtue of its aldosterone antagonist effect. It is known to act as an antiandrogen and also blocks androgen synthesis to an extent (33, 34). The drug has long been used in the treatment of hyperandrogenism (primarily hirsutism) and anovulation (35–39). Although the experience of spironolactone in PCOS is limited, it has a good safety record when used in smaller doses (37, 40, 41). To the best of our knowledge, there is no study that compares the efficacy of metformin with the antiandrogen spironolactone. Here we report an open-labeled, randomized study that compares the efficacy and safety of spironolactone with metformin in the management of women with PCOS. 2756 Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 Ganie et al. • Spironolactone vs. Metformin in PCOS Women Subjects and Methods Subjects Women attending the Endocrine and Metabolism Clinics of the All India Institute of Medical Sciences between 2000 and 2001 and meeting the National Institutes of Health National Institute of Child Health and Human Development 1990 consensus conference criteria for diagnosis of PCOS (42) were informed about the study. Of 168 women who met the above criteria, 82 volunteered to enter the study and were asked to give informed consent. The study was approved and conducted according to the guidelines of the Institute’s ethics committee. The inclusion criteria used to enroll the subjects were presence of menstrual disturbances and hirsutism after ruling out disorders such as Cushing’s syndrome, nonclassical adrenal hyperplasia, thyroid dysfunction, hyperprolactinemia, and androgen-secreting tumors. Menstrual disturbances were classified as oligo-/amenorrhea (ⱕ8 cycles/yr or menstrual interval ⱖ 35 d) and amenorrhea (absence of menses in last 6 or more months). Modified Ferriman-Gallwey score (43) by a single observer was used to assess the degree of hirsutism. A score of at least 8 of a total of 36 was taken as significant. This scoring system has been used previously in our population (44). The same observer, while being blind to the previous score, did follow-up scoring. Anthropometric assessment included measurement of body weight (kg), height (cm), BMI (kg/m2), and WHR. In addition to exclusion of the above mentioned disorders, patients volunteering use of any hormonal preparations or drug(s) known or suspected to affect reproductive or metabolic functions within 60 d of study entry or those having known diabetes mellitus or renal, hepatic, or cardiac dysfunction were also excluded. All married/sexually active women were advised to use barrier contraception throughout the study. Study protocol Blood samples were collected from the patients after an overnight fast for the estimation of T4, TSH, LH, FSH, prolactin (PRL), testosterone, J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 2757 dehydroepiandrosterone sulfate (DHEAS), cortisol (morning/evening or overnight dexamethasone suppression test, if needed), blood counts, electrolytes, lipids, liver, and kidney functions. Blood samples for hormonal investigations were collected from d 3–7 (early follicular phase) in subjects with spontaneous menstrual cycles. Safety evaluation included recording of vital signs and any adverse events in addition to the above workup. The oral glucose tolerance test (OGTT) was performed at 0800 h after an overnight fast with 75 g anhydrous glucose dissolved in 250 –300 ml water, and blood samples were collected before and 60 and 120 min later for plasma glucose and insulin. For insulin estimation, samples were collected in ice and plasma was separated immediately in cold centrifuge and stored at –20 C until the assay. For other hormones, serum was separated at room temperature and stored in a similar manner. A single observer did transabdominal ultrasonography to demonstrate any suggestion of polycystic ovarian morphology, i.e. presence of 10 or more peripheral follicles each measuring 2– 8 mm in size with echogenic ovarian stroma and/or increased ovarian volume (45). The echogenic theca was considered the most specific finding. All subjects were given a standard diet (35 kcal/kg comprising of 55– 60% carbohydrate, 20 –25% protein, and 20 –25% fat and high fiber content) and lifestyle advice (120-min brisk walking per week) at the beginning of the study. After baseline evaluation, eligible patients were randomized in an open-labeled manner by a simple randomization process using computer-generated random number allocation according to CONSORT guidelines (46). The allocation concealment was maintained until OGTT was done. Two groups received either metformin or spironolactone with the objective to compare the efficacy and safety of these drugs in the management of women with PCOS. Metformin (Glyciphage, FRANCO India Pharma Ltd., Mumbai, India) and spironolactone (Aldactone, RPG Life Sciences Ltd., Mumbai, India) were administered orally in a dose of 500 mg and 25 mg twice a day, respectively, and followed up for 6 months. The progress of subjects during the trial is shown in the CONSORT chart (Fig. 1). FIG. 1. CONSORT chart showing progress of subjects in both arms of the trial. Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 2758 J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 Ganie et al. • Spironolactone vs. Metformin in PCOS Women Laboratory analysis Hormonal assays were done in duplicate by RIA (T4, testosterone, DHEAS, 17-hydroxyprogesterone, cortisol, and insulin) and immunoradiometric assay (TSH, PRL, LH, and FSH). Commercial kits were supplied by Diagnostic Products Corp. (Los Angles, CA) (cortisol, 17hydroxyprogesterone, testosterone, and insulin), Immunotech (Marseilles, France) (DHEAS), and Medicorp Inc. (Montreal, Canada) (T4, TSH, LH, FSH, and PRL). Sensitivity, specificity, interassay, and intraassay coefficients of variation were within the prescribed limits given in the manufacturer’s protocol. Plasma glucose was measured by glucose oxidase-peroxidase method (Nicholas-Piramal India Ltd., Mumbai, India). Glucose tolerance was categorized according to WHO 1999 criteria (47). Insulin sensitivity was determined by homeostasis model assessment (HOMA) [(fasting insulin in mIU/liter ⫻ fasting glucose in mmol/liter)/22.5] (48), area under the curve for insulin (AUC-I), and fasting glucose/insulin ratio (FGIR) (mmol/liter/mIU/liter) (49). Statistical analysis The results are expressed as mean ⫾ sd. For comparison of all quantitative variables, clinical, biochemical, and hormonal parameters between metformin and spironolactone groups at baseline 3rd and 6th months, unpaired t test was used. The ANOVA for repeated measures was used to compare the clinical, biochemical, and hormonal parameters within each group. The Bonferroni test was used for multiple comparisons. Post hoc analysis was done, wherever necessary, to identify pairs of observations having significantly different levels of observations. Furthermore, to compare distribution of qualitative variables between groups, 2 test was used. A P value of ⬍0.05 was taken as significant. SPSS version 10.0 was used for statistical analysis. Results Baseline parameters Of 82 subjects recruited (n ⫽ 41 in each group) between 2000 and 2001, six subjects dropped out (two in the spironolactone and four in the metformin group), four had incomplete data, and three were lost to follow-up. Sixty nine subjects completed the 6-month follow-up for the final analysis (Fig. 1). Baseline clinical and anthropometric variables of these subjects in the spironolactone (n ⫽ 34) and metformin (n ⫽ 35) groups are compared in Table 1. Age, BMI, Ferriman-Gallwey score, and biochemical and hormonal profiles were comparable in the groups (Table 2). In all, 16 of 69 subjects had impaired glucose tolerance (IGT) and nine of 69 subjects were diabetic (blood glucose levels did not warrant pharmacological intervention) using World Health Organi- zation 1999 criteria. Of these, four diabetic and seven IGT subjects were in the spironolactone group. The BMI of subjects with diabetes mellitus/IGT was higher than those with normal glucose tolerance (27.53 ⫾ 5.56 vs. 25.98 ⫾ 5.09). Follow-up Metformin. Menstrual cycle frequency improved significantly with metformin, from 5.7 ⫾ 2.3 to 7.4 ⫾ 2.6 at 3 months and to 9.1 ⫾ 2.0 cycles/yr at 6 months (P ⫽ 0.001). The cycles regularized in the majority of subjects, although six of 35 cases persisted with oligo-/amenorrhea (Table 1). The hirsutism score decreased very gradually from 12.5 ⫾ 4.9 at baseline to 11.4 ⫾ 4.1 and 10.0 ⫾ 3.3 at the 3rd and 6th months of therapy, respectively (P ⫽ 0.001) (Table 1). Serum testosterone levels showed a significant decrease from a baseline of 3.25 ⫾ 1.59 to 2.53 ⫾ 1.9 and to 1.7 ⫾ 0.86 nmol/liter after the 3rd and 6th months (P ⫽ 0.001), respectively (Table 2 and Fig. 2). Serum DHEAS levels also showed a significant decrease (Table 2). Insulin sensitivity (HOMA, AUC-I, and FGIR) showed a significant decrease (Fig. 3). OGTT results revealed no major changes except a downward trend in the 2-h glucose (Table 2). There was no significant effect on BMI, WHR, BP, and LH levels with 6 months of metformin therapy (Tables 1 and 2). Spironolactone. Menstrual cycle frequency increased from 6.6 ⫾ 2.1 to 9.0 ⫾ 1.9 at 3 months and to 10.2 ⫾ 1.9 cycles/yr at 6 months (P ⫽ 0.001) (Table 1). The menstrual irregularity persisted in six of 34 subjects, and new cycle irregularity developed in five of 34 subjects. The irregularity, however, was not significant enough to cause drug withdrawal. The hirsutism score decreased from 12.9 ⫾ 3.2 at baseline to 10.1 ⫾ 3.1 at 3 months and to 8.7 ⫾ 1.9 at 6 months of therapy (P ⫽ 0.034) (Table 1). Serum testosterone levels showed a significant decrease (P ⫽ 0.001) from 3.57 ⫾ 0.34 to 1.94 ⫾ 1.0 at the 3rd month and did not change much thereafter (to 1.94 ⫾ 1.00 nmol/liter at the 6th month) (Fig. 3). Serum DHEAS levels decreased significantly, whereas LH levels showed a nonsignificant decrease. Like metformin, OGTT parameters and insulin sensitivity (by HOMA, AUC-I, and FGIR) showed a decreasing trend (Table 2 and Fig. 3). Sim- TABLE 1. Clinical parameters of the subjects before and during treatment Metformin group (n ⫽ 35) 0 months Age (yr) BMI (kg/m2; normal range, 20 –25) WHR (normal range ⬍ 0.80) Age of menarche (yr) No. of menstrual cycles/yr (normal range ⱖ 8) Hirsutism score (normal range ⱕ 8) Hirsutism duration (yr) BP systolic (mm Hg; normal range ⱕ 120) BP diastolic (mm Hg; normal range ⱕ 90) 22.9 ⫾ 5.3 26.5 ⫾ 5.6 (17–34)a 0.9 ⫾ 0.1 12.9 ⫾ 1.3 5.7 ⫾ 2.3 3 months 25.7 ⫾ 4.5 0.85 ⫾ 0.1 Spironolactone group (n ⫽ 34) 6 months 25.6 ⫾ 4.7 0.85 ⫾ 0.1 0 months 23.3 ⫾ 5.2 25.9 ⫾ 5.0 (18 –35)a 0.86 ⫾ 0.1 13.0 ⫾ 1.2 6.6 ⫾ 2.1 3 months 6 months 25.7 ⫾ 4.8 0.85 ⫾ 0.1 25.5 ⫾ 4.6 0.86 ⫾ 0.1 7.4 ⫾ 2.6b 9.1 ⫾ 2.0b 9.0 ⫾ 1.9b 12.5 ⫾ 4.9 11.4 ⫾ 4.1b 10.0 ⫾ 3.3b 12.9 ⫾ 3.2 10.1 ⫾ 3.1 8.7 ⫾ 1.9 4.0 ⫾ 2.5 122.9 ⫾ 14.9 118.3 ⫾ 18.8 122.2 ⫾ 14.9 4.4 ⫾ 2.7 122.7 ⫾ 8.50 123.1 ⫾ 6.4 122.9 ⫾ 14.7 81.1 ⫾ 5.0 81.2 ⫾ 6.4 79.6 ⫾ 14.3 82.9 ⫾ 4.8 80.3 ⫾ 6.8 81.4 ⫾ 5.6 Results are given as mean ⫾ SD. a BMI range. b P ⬍ 0.05 for comparison within the group. Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 10.2 ⫾ 1.9b 90 ⫾ 15.6 (5 ⫾ 0.8) 135.2 ⫾ 49.5 (7.51 ⫾ 2.75) 132.8 ⫾ 48.1 (7.38 ⫾ 2.67) 11,235.71 ⫾ 4,328 18.47 ⫾ 18.93 (132.52 ⫾ 135.8) 122.61 ⫾ 14.37 (879.7 ⫾ 103.1) 84.65 ⫾ 9.69 (607.4 ⫾ 68.9) 10,926.6 ⫾ 6,855 4.0 ⫾ 4.18 7.9 ⫾ 0.74 7.83 ⫾ 5.72 3.65 ⫾ 2.37 2.72 ⫾ 0.5 83.9 ⫾ 45.8 (3.25 ⫾ 1.59) 257.9 ⫾ 122.3 (7.0 ⫾ 3.32) 91.4 ⫾ 13.1 (5.08 ⫾ 0.7) 135.7 ⫾ 36.9 (7.54 ⫾ 2.05) 122.2 ⫾ 36.5 (6.79 ⫾ 2.03) 11,960.4 ⫾ 3,208 13.29 ⫾ 17.6 (95.36 ⫾ 125.9) 79.54 ⫾ 8.5 (570.7 ⫾ 60.9) 56.35 ⫾ 6.7 (404.3 ⫾ 48.1) 6,862.14 ⫾ 4,015a 3.35 ⫾ 4.12 10.0 ⫾ 0.59a 7.22 ⫾ 5.06 4.08 ⫾ 1.92 2.21 ⫾ 0.36 72.9 ⫾ 54.8 (2.53 ⫾ 1.90) 241.7 ⫾ 110.5 (6.56 ⫾ 3.0) 3 months Metformin group (n ⫽ 35) 95.9 ⫾ 12.9 (5.33 ⫾ 0.7) 135.4 ⫾ 33.3 (7.52 ⫾ 1.85) 115.7 ⫾ 24.7 (6.43 ⫾ 1.37) 11,927 ⫾ 3,652 14.28 ⫾ 17.5 (102.5 ⫾ 125) 55.85 ⫾ 6.09 (400.7 ⫾ 43.7)b 43.81 ⫾ 6.5b (314.3 ⫾ 46.6) 4,990.8 ⫾ 3,132a 2.55 ⫾ 1.44a 10.83 ⫾ 0.69a 5.34 ⫾ 3.34a 6.06 ⫾ 8.38 1.38 ⫾ 0.18a 49.9 ⫾ 24.8 (1.7 ⫾ 0.86)a 225.5 ⫾ 101.3 (6.1 ⫾ 2.7)b 6 months 90.5 ⫾ 11.7 (5.03 ⫾ 0.6) 133.6 ⫾ 45.4 (7.42 ⫾ 2.52) 116.1 ⫾ 34.6 (6.45 ⫾ 1.92) 11,649.1 ⫾ 3,645 22.17 ⫾ 49.02 (159.0 ⫾ 351.7) 103.88 ⫾ 15.16 (745.3 ⫾ 108.8) 76.34 ⫾ 14.95 (547.7 ⫾ 107.3)d 9,203.2 ⫾ 8,667 5.32 ⫾ 13.12 9.1 ⫾ 0.7d 6.67 ⫾ 3.34 4.12 ⫾ 1.77 1.73 ⫾ 0.19b 55.9 ⫾ 28.8 (1.94 ⫾ 1.0)a 253.1 ⫾ 140.0 (6.87 ⫾ 3.8) 3 months 6 months 93.8 ⫾ 12.4 (5.21 ⫾ 0.7) 135.4 ⫾ 33.3 (7.52 ⫾ 1.85) 115.7 ⫾ 24.6 (6.43 ⫾ 1.37) 11,775.5 ⫾ 2,459 10.37 ⫾ 5.7 (74.4 ⫾ 40.7) 84.51 ⫾ 14.2 (606.4 ⫾ 101.9)a,d 66.97 ⫾ 14.4 (480.5 ⫾ 103.3)a,d 7,450.5 ⫾ 7,141 5.27 ⫾ 8.81c 9.7 ⫾ 0.69d 6.3 ⫾ 3.54a 4.68 ⫾ 1.70 1.29 ⫾ 0.18b 55.9 ⫾ 28.8 (1.94 ⫾ 1.0)a 229.5 ⫾ 73.7 (6.23 ⫾ 2.0)a Spironolactone group (n ⫽ 34) 87.3 ⫾ 14.9 (4.85 ⫾ 0.8) 131.6 ⫾ 44.6 (7.31 ⫾ 2.48) 121.9 ⫾ 40.8 (6.77 ⫾ 2.27) 11,704.6 ⫾ 3,792 26.67 ⫾ 45.8 (191.4 ⫾ 328.5) 139.43 ⫾ 23.9 (1,000.4 ⫾ 171) 91.02 ⫾ 16.7 (653.1 ⫾ 119.8) 11,349.1 ⫾ 1,113 4.92 ⫾ 6.94 8.1 ⫾ 0.7 9.01 ⫾ 5.42 3.72 ⫾ 2.13 2.7 ⫾ 0.35d 102.9 ⫾ 9.8 (3.57 ⫾ 0.34) 255.3 ⫾ 101.3 (6.93 ⫾ 2.75) 0 months Results are given as mean ⫾ SD. Conversion factors are as follows: insulin, pmol/liter ⫽ U/ml ⫻ 7.175; LH and FSH, IU/liter ⫽ mIU/ml ⫻ 1; testosterone, nmol/liter ⫽ ng/dl ⫻ 0.03467; glucose, mmol/liter ⫽ mg/dl ⫻ 0.0555; DHEAS, mol/liter ⫽ g/dl ⫻ 0.02714. BG, Blood glucose; ref., reference. a P ⬍ 0.05 and b P ⬍ 0.001 for comparison within the group. c P ⬍ 0.05 and d P ⬍ 0.001 for comparison between metformin and spironolactone groups. DHEAS, mg/dl (mol/liter) (0.81– 8.91) AUC-I HOMA (ref. range ⱕ 2) FGIR (ref. range ⱕ 4.5) LH, mIU/ml (IU/liter; ref. range ⫽ 0.5–15) FSH, mIU/ml (IU/liter; ref. range ⫽ 0.2–10) LH/FSH ratio (ref. range ⱕ 2) Testosterone, ng/dl (nmol/liter; ref. range ⬍ 2.25) Insulin 2 h, U/ml (pmol/liter) Insulin 1 h, U/ml (pmol/liter) AUC-glucose Insulin fasting, U/ml (pmol/liter, ref. range 35–145) BG 2 h, mg/dl (mmol/liter; ref. range ⬍ 7.78) BG 1 h, mg/dl (mmol/liter; ref. range ⬍ 7.7) BG fasting; mg/dl (mmol/liter; ref. range ⬍ 6.1) 0 months TABLE 2. Biochemical and hormonal parameters of the subjects before and during treatment Ganie et al. • Spironolactone vs. Metformin in PCOS Women J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 2759 Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 2760 J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 Ganie et al. • Spironolactone vs. Metformin in PCOS Women less common with spironolactone. Polyuria (four of 34), abdominal pain (one of 34, leading to drug withdrawal), and menstrual irregularity (nine of 34) were noted in the spironolactone group. One subject had hyperuricemia, which persisted after drug withdrawal and was probably unrelated. The metformin group had vomiting, nausea (four of 35), diarrhea (eight of 35), and hyperadrenergic symptoms but not a documented hypoglycemia (two of 35) leading to drug withdrawal in four subjects. Discussion FIG. 2. Comparing the effect of spironolactone and metformin on serum testosterone levels before and after treatment (conversion factor, nmol/liter ⫽ ng/dl ⫻ 0.03467). FIG. 3. Comparing the effect of spironolactone and metformin on blood glucose and plasma insulin levels before and after treatment (as shown by AUC) (conversion factor for insulin, pmol/liter ⫽ U/ml ⫻ 7.175; for glucose, mmol/liter ⫽ mg/dl ⫻ 0.0555). ilarly, there was no significant effect of spironolactone on BMI, WHR, and blood pressure (Table 1). Metformin vs. spironolactone. Compared with metformin, spironolactone was more effective in increasing the frequency of menstrual cycles both at the 3rd (P ⫽ 0.006) and the 6th month (P ⫽ 0.03), although at the cost of some menstrual irregularity. This irregularity, however, did not affect the patient satisfaction with this drug. There was a significant fall in testosterone with both drugs, although the effect was rapid (i.e. by the 3rd month) with spironolactone. The difference in LH and testosterone disappeared by the 6th month due to an equal but delayed effect of metformin (Table 2). Interestingly, glucose intolerance improved by the same magnitude in both groups (P ⫽ 0.79). At the end of the study, one diabetic and five IGT subjects were in the metformin group compared with no diabetic and four with IGT in the spironolactone group. At the beginning of the study, nine IGT and five diabetics were in the metformin group vs. seven IGT and four diabetics in the spironolactone group. There was no statistically significant difference between the groups regarding BMI, WHR, or blood pressure (Table 1). Adverse events were Insulin resistance is now considered as one of the essential components in the pathogenesis of PCOS (7–12, 22). Although the precise molecular basis of insulin resistance has not been elucidated, the defects can occur at insulin binding, receptor, or postreceptor levels and may be disproportionate to the degree of obesity (11, 22, 50). The excess insulin has been postulated to partly augment LH-stimulated androgen secretion from the ovarian tissues and partly to increase free androgens by decreasing circulating SHBG levels (50, 51). Based on this mechanism, metformin has been lately in vogue for the treatment of menstrual disturbances, hirsutism, ovulation induction, cervical scores, pregnancy outcomes, etc. in PCOS (18, 22–29, 31, 32). Spironolactone, an antiandrogen, has been in use for the treatment of hyperandrogenism for nearly 21⁄2 decades. Its main benefit stems from blocking androgen receptors with a minor contribution from a decrease in androgen synthesis (33–36). Although experience with the drug in PCOS is limited, it has a good safety record at doses of 50 –100 mg both on a short- and a long-term basis (37– 41). This randomized, open-labeled study compared the efficacy and safety of these two drugs (metformin, 1000 mg daily, and spironolactone, 50 mg daily) with diverse mechanisms of action. Sixty-nine subjects completed 6 months of the study and were analyzed. Clinical, hormonal, and biochemical profiles of the two groups were comparable at baseline. With metformin, the menstrual pattern regularized in the majority of the subjects, and these findings are in agreement with most recent clinical trials with metformin (18, 31, 32). The hirsutism score decreased very gradually, and the benefit was significant and appreciable by 6 months. Kelly and Gordon (52) observed a similar improvement in quantitative hair parameters, although the effect was noted earlier, i.e. by the 3rd month. Serum testosterone and DHEAS levels showed a significant decrease by the 6th month of therapy as shown earlier (32). Although severity of glucose tolerance abnormalities showed a positive trend, it did not reflect in any improvement in individual OGTT parameters. Insulin sensitivity demonstrated a significant increase with metformin as has been demonstrated earlier (13, 15, 18, 31, 32). There was no significant effect on BMI, WHR, and blood pressure with 6 months of metformin therapy. Most of the studies have shown variable results on these parameters (31, 32). Most of the data on metformin available have been generated with doses ranging from 1.5–2 g/d, which is higher than the dose used in our study. Although the efficacy of the drug at this dose in Western subjects has been inferior (16, 53), we found comparable efficacy to higher doses with Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 Ganie et al. • Spironolactone vs. Metformin in PCOS Women a fewer number of adverse effects. This may be attributed to the lower body mass of our subjects. With spironolactone, the number of cycles per year increased with 6 months of therapy. The menstrual irregularity persisted in six of 34 subjects, and new cycle irregularity developed in five of 34 subjects. This drug is known to cause such irregularity in menstrual cycles (39, 40, 54, 55), although the irregularity was not significant enough to cause drug withdrawal in this study. The hirsutism score decreased significantly by 6 months. Our results are similar to many studies, although the dose used was higher (38 – 40). The serum testosterone and LH levels and LH/FSH ratio showed a significant decrease compared with variable effects observed earlier (36 – 40). There was no significant effect on BMI, WHR, blood pressure, OGTT parameters, and insulin sensitivity, although a significant fall was observed in 1- and 2-h insulin levels. Both these drugs showed significant improvement in menstrual cycle pattern, hirsutism score, and androgen levels, suggesting their efficacy in the treatment of PCOS. Spironolactone appears to be a better choice than metformin in view of better efficacy on hair growth and patient acceptance; however, metformin was superior in menstrual regularization and improving insulin sensitivity. Although spironolactone induced mild menstrual cycle irregularity as reported (37– 40), in the present study the abnormality was too subtle to cause any patient dissatisfaction or drug withdrawal. This may be because of a smaller dose of the drug used in the present study. However, the efficacy was comparable with earlier studies using higher doses (37–39, 54, 55). Both agents showed a similar effect on glucose tolerance abnormalities. Of four diabetics and seven IGT subjects in the spironolactone group at baseline, only four persisted with IGT and none was diabetic at the end of the study. In the metformin group at the end of 6 months, five patients persisted with IGT and one subject continued to be diabetic from a baseline figure of nine IGT and five diabetics. This comparable benefit can be attributed to diet and lifestyle modification, which was similar in both groups. Insulin sensitivity improved in both groups, although it reached statistical significance only in the metformin group. This is in agreement with earlier reports (13–15, 18, 31, 32). In the present study comparing metformin and spironolactone in countering insulin resistance, metformin is definitely superior, but this effect did not seem to translate into commensurate clinical benefits such as a fall in androgens or alterations in blood glucose levels during this short-term study. Instead, we observed that spironolactone ameliorated most of the clinical features of PCOS in addition to some fall in insulin levels. If insulin resistance was the basic pathogenic factor, then metformin should have shown superior effects on glucose tolerance, serum androgen levels, and hair parameters. Recent evidence that metformin causes direct inhibition of androgen synthesis by thecal cells (29, 30) lends support to our observations that the insulin-lowering effect of metformin probably is not the entire mechanism of the clinical benefit of metformin in PCOS. We conclude that both spironolactone and metformin are effective agents in the management of various components of PCOS. Spironolactone appears to be better than metformin in the treatment of hirsutism and hormonal derangements of J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 2761 PCOS and has a better patient tolerance at the dose used. The fact that superior positive effects of metformin on insulin sensitivity did not translate into the proportionate clinical benefit in these PCOS subjects raises doubts about insulin resistance as the sole pathogenetic factor. Acknowledgments We gratefully acknowledge Dr. Nandita Gupta for her help in insulin estimation and Dr. Rajvir for statistical analysis. Received October 10, 2003. Accepted February 23, 2004. Address all correspondence and requests for reprints to: Dr. A. C. Ammini, Department of Endocrinology and Metabolism, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029, India. E-mail: [email protected]. References 1. Stein IF, Leventhal ML 1935 Amenorrhoea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 29:181–191 2. Franks S 1995 Polycystic ovary syndrome. N Engl J Med 333:853– 861 3. Homberg R 1996 Polycystic ovary syndrome: from gynaecological curiosity to multisystem endocrinopathy. Hum Reprod 11:29 –39 4. Gjonnaess H 1984 Polycystic ovarian syndrome treated by ovarian electrocautery through the laparoscope. Fertil Steril 41:20 –25 5. Wang CF, Gemzell C 1980 The use of human gonadotropins for the induction of ovulation in women polycystic ovary disease. Fertil Steril 33:479 – 486 6. Gorlitsky GA, Case NG, Speroff L 1978 Ovulation and pregnancy rates with clomiphene citrate. Obstet Gynecol 51:265–269 7. Ibanez L, Vallus C, Ferrer A, Marcos MV, Rodriguez-Hierro, de Zegher F 2001 Sensitization of insulin induces ovulation in nonadolescents with anovulatory hyperandrogenism. J Clin Endocrinol Metab 86:3595–3598 8. Dunaif A, Graf M, Mendeli J, Laumas U, Dobrjansky A 1987 Characterization of groups of hyperandrogenic women with acanthosis nigricans, impaired glucose tolerance, and/or hyper insulinemia. J Clin Endocrinol Metab 65:499 – 507 9. Chang RJ, Nakamura RM, Judd HL, Kaplan SA 1983 Insulin resistance in non-obese patients with polycystic ovarian disease. J Clin Endocrinol Metab 57:356 –359 10. Pasquali R, Casimiri F, Vincennati V 1997 Weight control and its beneficial effects on fertility in women with obesity and polycystic ovary syndrome. Hum Reprod 12(Suppl 1):82– 87 11. Dunaif A, Segal K, Futterweit W, Dobrjansky A 1989 Profound peripheral insulin resistance independent of obesity in polycystic ovary syndrome. Diabetes 38:1165–1169 12. Barberri RL, Makris A, Randall RW, Daniels G, Kistner RW, Ryan KJ 1986 Insulin stimulates androgen accumulation in incubations of ovarian stroma obtained from women with hyperandrogenism. J Clin Endocrinol Metab 62: 904 –910 13. Moghetti P, Castello R, Negri C, Tosi F, Perrone F, Caputo M, Zanolin E, Muggeo M 2000 Metformin effects on clinical features, endocrine and metabolic profiles, and insulin sensitivity in polycystic ovary syndrome: a randomized, double-blind, placebo-controlled 6-month trial, followed by open, long-term clinical evaluation. J Clin Endocrinol Metab 85:139 –146 14. Nestler JE, Jakubowicz DJ, Evans WS, Pasquali R 1998 Effects of Metformin on spontaneous and clomiphene-induced ovulation in the polycystic ovary syndrome. N Engl J Med 338:1876 –1880 15. Glueck CJ, Wang P, Kobayashi S, Phillips H, Sieve-Smith L 2002 Metformin therapy throughout pregnancy reduces the development of gestational diabetes in women with polycystic ovary syndrome. Fertil Steril 77:520 –525 16. Vrbikova J, Bicikova M, Tallova J, Hill M, Starka L 2002 Homocystine and steroid levels in metformin treated women with polycystic ovary syndrome. Exp Clin Endocrinol Diabetes 110:74 –76 17. Haas DA, Carr BR, Attia GR 2003 Effects of metformin on body mass index, menstrual cyclicity, and ovulation induction in women with polycystic ovary syndrome. Fertil Steril 79:469 – 481 18. Lord JM, Flight IH, Norman RJ 2003 Metformin in polycystic ovary syndrome: systemic review and meta-analysis. BMJ 327:951–955 19. Hasegawa I, Murakawa H, Suzuki M, Yamamoto Y, Kurabayashi T, Tanaka K 1999 Effect of troglitazone on endocrine and ovulatory performance in women with insulin resistance related polycystic ovary syndrome. Fertil Steril 71:323–327 20. Azziz R, Ehrmann D, Legro RS, Whitcomb RW, Hanley R, Fereshetian AG, O’Keefe M, Ghazzi MN 2001. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome: a multicenter, double-blind, and placebocontrolled trial. J Clin Endocrinol Metab 86:1626 –1632 21. Ehrmann DA, Schneider DJ, Sobel BE, Cavaghan MK, Imperial J, Rosenfield Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009 2762 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. J Clin Endocrinol Metab, June 2004, 89(6):2756 –2762 RL, Polonsky KS 1997 Troglitazone improves defects in insulin action, insulin secretion, ovarian steroidogenesis and fibrinolysis in women with polycystic ovary syndrome. J Clin Endocrinol Metab 82:2108 –2116 De Leo V, la Marca A, Petraglia F 2003 Insulin-lowering agents in the management of polycystic ovary syndrome. Endocr Rev 24:633– 667 Kolodziejczyk B, Duleba AJ, Spaczynski RZ, Pawelczyk L 2000 Metformin therapy decreases hyperandrogenism and hyperinsulinemia in women with polycystic ovary syndrome. Fertil Steril 73:1149 –1154 Batukan C, Baysal B 2001 Metformin improves ovulation and pregnancy rates in patients with polycystic ovary syndrome. Arch Gynecol Obstet 265:124 –127 Malkawi HY, Qublan HS 2002 The effect of metformin plus clomiphene citrate on ovulation and pregnancy rates in clomiphene citrate resistant women with polycystic ovary syndrome. Saudi Med J 23:663– 666 Flemming R, Hopkinson ZE, Wallace AM, Greer IA, Sattar N 2002 Ovarian function and metabolic factors in women with oligomenorrhea treated with metformin in randomized double blind placebo-controlled trial. J Clin Endocrinol Metab 87:569 –574 Kocak M, Caliskan E, Simsir C, Haberal A 2002 Metformin therapy improves ovulatory rates, cervical scores, and pregnancy rates in clomiphene citrate resistant women with polycystic ovary syndrome. Fertil Steril 77:101–106 Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW, Nestler JE 2001 Metformin increases ovulatory rate and pregnancy rates from clomiphene citrate in patients with polycystic ovary syndrome who are resistant to clomiphene citrate alone. Fertil Steril 75:310 –315 Attia GR, Rainey WE, Carr BR 2001 Metformin directly inhibits androgen production in human thecal cells. Fertil Steril 76:517–524 Manfield R, Galea R, Brincat M, Hole D, Mason H 2003 Metformin has direct effects on human ovarian steroidogenesis. Fertil Steril 79:956 –962 Castello MF, Eden JA 2003 A systemic review of the reproductive system effects of metformin in patients with polycystic ovary syndrome. Fertil Steril 79:1–13 Lord JM, Flight IH, Norman RJ 2003 Insulin-sensitising drugs (metformin, troglitazone, rosiglitazone, pioglitazone, d-chiro-inositol) for polycystic ovary syndrome. Cochrane Database Syst Rev 3:CD003053 Stripp B, Taylor AA, Bartter FC, Gillette JR, Loriaux DL, Easly R, Menard RH 1974 Effect of spironolactone on sex hormone in man. J Clin Endocrinol Metab 41:777–779 Corvol P, Michaud A, Menard J, Friefeld M, Mahoudean J 1975 Antiandrogenic effect of spironolactone: mechanism of action. Endocrinology 97:52–54 Spritzer PM, Lisboa KO, Mattiello S, Lhullier F 2000 Spironolactone as a single agent for long-term therapy of hirsute patients. Clin Endocrinol (Oxf) 52:587–594 Lobo RA, Shoupe D, Serafini P, Brinton D, Horton R 1985 The effects of two doses of spironolactone on serum androgens and anagen hair in hirsute women. Fertil Steril 43:200 –205 Cumming DC, Yang JC, Rebar RW, Yen SS 1982 Treatment of hirsutism with spironolactone. J Am Med Assoc 247:1295–1298 Lee O, Farquhar C, Toomath R, Jepson R 2000 Spironolactone versus placebo Ganie et al. • Spironolactone vs. Metformin in PCOS Women 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. or in combination with steroids for hirsutism and/or acne. Cochrane Database Syst Rev 4:CD000194 Milewicz A, Silber D, Kirschner MA 1983 Therapeutic effects of spironolactone in polycystic ovary syndrome. Obstet Gynecol 61:429 – 432 Shaw JC, White LE 2002 Long-term safety of spironolactone in acne: results of an 8-year followup study. J Cutan Med Surg 6:541–545 Helfer EL, Miller JL, Rose LI 1988 Side-effects of spironolactone in the hirsute woman. J Clin Endocrinol Metab 66:208 –211 Zawadzki JK, Dunaif A 1992 Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. In: Dunaif A, Givens JR, Haseltine FP, Merriam GR, eds. Polycystic ovary syndrome: current issues in endocrinology and metabolism, Vol. 4. Boston: Blackwell Scientific; 377–384 Ferriman D, Gallwey JD 1961 Clinical assessment of body hair growth in women. J Clin Endocrinol Metab 21:1440 –1447 Mathur SK, Ammini AC 1996 Body hair distribution of women attending Endocrine OPD. Indian J Dermatol Venerol Leprol 62:268 Adams J, Polson DW, Franks S 1986 Prevalence of polycystic ovaries in women with an ovulation and idiopathic hirsutism. BMJ 293:355–359 Altman DG, Schulz KF, Moher DE, Egger M, Davidoff F, Elbourne D, Gotzsche PC, Lang T 2001 The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med 134:663– 691 World Health Organization 1999 Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a World Health Organization Consultation, part I: diagnosis and classification of diabetes mellitus. Geneva: World Health Organization Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC 1985 Homeostasis model assessment (HOMA): insulin resistance and -cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412– 419 Legro RS, Finegood D, Dunaif A 1998 A fasting glucose to insulin ratio is a useful measure of insulin sensitivity in women with polycystic ovary syndrome. J. Clin Endocrinol Metab 83:2694 –2698 Cibula D, Skrha J, Hill M, Fanta M, Haakova L, Vrbikova J, Zivny J 2002 Prediction of insulin sensitivity in nonobese women with polycystic ovary syndrome J Clin Endocrinol Metab 87:5821–5825 Patel K, Coffler M S, Dahan M H, Yoo RY, Lawson M A Malcom PJ, Chang R J Increased luteinizing hormone secretion in women with polycystic ovary syndrome is unaltered by prolonged insulin infusion. J Clin Endocrinol Metab 88:5456 –5461 Kelly C J, Gordon D 2002 The effect of metformin on hirsutism in polycystic ovary syndrome. Eur J Endocrinol 147:217–221 Unluhizarci K, Kelestimur F, Bayram F, Sahin Y, Tutus A 1999 The effects of metformin on insulin resistance and ovarian steroidogenesis in women with polycystic ovary syndrome. Clin Endocrinol (Oxf) 51:231–236 Trembly RR 1986 Treatment of hirsutism with spironolactone. Clin Endocrinol Metab 15:363–371 Kelestimur F, Sahin Y 1998 Comparison of Diane 35 and Diane 35 plus spironolactone in the treatment of hirsutism. Fertil Steril 69:66 – 69 JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community. Downloaded from jcem.endojournals.org at Indonesia:Endo Jnls Sponsored on January 7, 2009