Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
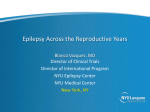
Brain Advance Access published December 1, 2004 DOI: 10.1093/brain/awh363 Brain Page 1 of 11 INVITED REVIEW Cancer risk in people with epilepsy: the role of antiepileptic drugs Gagandeep Singh,1 Pablo Hernáiz Driever2 and Josemir W. Sander1 1 Correspondence to: Ley Sander, Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, Queen Square, London WC1N 3BG, UK E-mail: [email protected] Summary There has been considerable debate about the relationship between epilepsy and cancer, in particular whether the incidence of cancer is increased in people with epilepsy and whether antiepileptic drugs promote or protect against cancer. We review available evidence from animal experiments, genotoxicity studies and clinico-epidemiological observations, and discuss proposed mechanisms underlying the association between epilepsy and cancer. A carcinoma-promoting effect has been seen unequivocally in rodent models for phenobarbital and phenytoin; phenobarbital promoted liver tumours and phenytoin caused lymphoid cell and liver tumours in rats. Early human epidemiological studies found an association between phenobarbital and hepatocellular carcinoma, and several subsequent studies suggested an association with lung cancer. An association with brain tumours has also been demonstrated. Phenytoin has been causally implicated in three human cancers: lymphoma, myeloma and neuroblastoma, the latter specifically in the setting of foetal hydantoin syndrome. However, despite considerable long-term pharmaco-epidemiological data being available for both antiepileptic drugs, evidence for human carcinogenicity is not consistent and both are considered only possibly carcinogenic to humans. Valproate, however, has been found to exert an antiproliferative effect on certain cancer cell lines both in vitro and in vivo. A corresponding cancer-suppressive effect has not been studied in human epidemiological studies, though there are now preliminary reports of the use of valproate in human haematological and solid tumours. The anticancer activity of valproate appears to be driven by histone deacetylase inhibition and to be independent of hormone or multidrug protein resistance dependant mechanisms. The newer antiepileptic drugs appear to be safe, as no carcinogenicity has been demonstrated either during regulatory testing or in post-marketing surveillance. Nevertheless, the subject of cancers and epilepsy constitutes a promising agenda for clinical and experimental research in the future. Keywords: epilepsy; cancer; co-morbidity; antiepileptic drugs; carcinogenicity Abbreviations: AED = antiepileptic drug; GSK3=glycogen synthase kinase3; HDAC = histone deacetylase; IARC = International Agency for Research in Cancer; SIR = standardized incidence ratio; SMR = standardized mortality ratio Received September 9, 2004. Revised November 16, 2004. Accepted November 17, 2004 Introduction People with a history of epilepsy represent a sizeable proportion (1–2%) of the general population (Bell and Sander, 2002; Sander, 2003). The challenge to improve their overall health status is contingent not only upon controlling seizures but also on managing several concomitant health conditions. Indeed, comorbidity is widespread in Brain # Guarantors of Brain 2004; all rights reserved epilepsy and is a focus of much recent attention (Gaitatzis et al., 2004). The concern that epilepsy or its treatment may be causally implicated in the development and subsequent course of several health conditions is an area of ongoing interest. The spectrum of comorbidity encompasses not only neuropsychiatric disorders such as dementia, learning Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, London, UK and 2Department of Pediatric Oncology and Hematology, Campus Virchow Hospital, Charité Universitätsmedizin Berlin, Berlin, Germany Page 2 of 11 G. Singh et al. Overview of carcinogenicity testing The seminal event in carcinogenesis is often the mutational transformation of proto-oncogenes, tumour-suppressor genes or other genes controlling cell proliferation. In addition, epigenetic events at translational and post-translational level, such as DNA methylation, acetylation of nuclear proteins, alternative splicing of mRNA and modification of proteins by phosphorylation or nitrosylation, may initiate carcinogenesis (Hanahan and Weinberg, 2000). One of these, regulation of acetylation of the nuclear proteins known as histones (histone deacetylation and acetylation), is mechanistically relevant to the present review, as described later (Fig. 1). The net result of the combination of these molecular events is that cancer cells are rendered self-sufficient in growth signals and insensitive to anti-growth signals, and are able to evade apoptosis, sustain angiogenesis, replicate limitlessly and invade neighbouring tissues as well as metastasize. The list of pharmaceutical agents suspected or known to be carcinogenic is long. In general, the carcinogenic potential of pharmaceutical agents is inferred from three types of Balance of genomic expression in cancer cells HDAC sensitive promoter regions Histone Acetyltransferase Histone Deacetylase Open gene / Active euchromatin Closed gene / Silent heterochromatin Histone Deacetylase Histone Acetyltransferase Arrest of cell growth Differentiation Apoptosis Cell growth Dedifferentiation Survival Valproate Note: Histone Deacetylase Acetylated Histones Deacetylated Histones Histone Acetyltransferase Fig. 1 Diagrammatic representation of the interaction between valproate and acetylation status of DNA-associated proteins known as histones in development of cancer. Ac = acetyl group; HDAC = histone deacetylase). Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 disabilities and depression, but also non-neurological conditions such as cancer. Cancer is the second most frequent cause of death worldwide. Naturally, it can complicate several chronic medical conditions, including epilepsy, fuelling concerns about the cancer risk or lack thereof associated with the underlying disorder. Pertinent to this cancer risk is the carcinogenicity of drugs used over long periods of time to treat these disorders, particularly so because drug exposure is a potentially avoidable risk. Accordingly, testing for carcinogenicity is crucial in the evaluation of drug safety. The potential for antiepileptic drugs (AEDs) to be carcinogenic was investigated in experimental, epidemiological and clinical research, particularly in the late 1960s and 1970s (Peraino et al., 1971; White et al., 1979). The issue is far from settled, however, although it has not attracted much attention recently. In this article, we review available experimental and human data on the occurrence of cancer in people with epilepsy and present an argument for further studies in this area. Cancer risk and anticonvulsants studies: (i) laboratory animal assays in which rodents are exposed to the agent, either chronically to usual doses or, more often, to discrete maximal tolerated doses; (ii) genotoxic assays, where the agent’s potential to cause chromosomal damage or aberrations is estimated in vitro; and (iii) longterm human epidemiological studies of users of the drug. Rodent carcinogenesis is mechanistically simple and involves a limited number of oncogenic events. Distinct from this, human carcinogenesis is a complex process; in experimental situations an array of at least five different genetic events is required to render normal cells malignant (Hahn and Weinberg, 2002). Not surprisingly, animal carcinogenicity data, which suggested neoplastic development at a variety of sites for several pharmaceutical agents, have not been confirmed in human epidemiological data for many agents. Carcinogenicity studies for AEDs may be carried out in samples of people with either cancer or epilepsy. Studies in samples of persons with cancer use a retrospective case– control design. Though theoretically appealing, these are rarely feasible, being complicated by recall bias and the fact that epilepsy history is often not mentioned in records of cancer registries or death certificates of people dying of cancer (Bell et al., 2004). The alternative, estimating cancer incidence or mortality in epilepsy cohorts, is used more often (Clemmesen and Hjalgrim-Jensen, 1978; White et al., 1979; Shirts et al., 1986; Olsen et al., 1989; Lamminpaa et al., 2002). Ideally, such samples should be large, and prospectively followed up for several decades in view of the time required for the development of cancers and the low frequencies of individual cancer types. Providing necessary information is available and the sample size is sufficiently large, it might also be possible to undertake nested case-control studies within such cohorts. In reality, however, long prospective follow-ups are logistically not very feasible. Most studies so far have surmounted the problem of prospective follow-up by backdating follow-ups to several years previously (Clemmesen and Hjalgrim-Jensen, 1978; White et al., 1979; Olsen et al., 1989; Lamminpaa et al., 2002). Good examples of the latter are cohorts of institutionalized epilepsy patients, whose records may be traced back to the point of institutionalization (Clemmesen and Hjalgrim-Jensen, 1978; White et al., 1979; Olsen et al., 1989), of hospital clinic attendees, of persons applying for driving privileges (D. Lowe, A. E. M. McLean and J. Taylor, unpublished, 1986) and from prescription records of pharmacies or insurance agencies (Friedman and Ury, 1980, 1983; Selby et al., 1989; Lamminpaa et al., 2002). Cancer incidence or mortality can then be ascertained through cancer registries or demographic databases. However, it may not be possible to confirm a diagnosis of epilepsy and verify durations and compliance of AEDs taken in such cohorts. Moreover, it is often not possible to make note of the presence of confounding risk factors, such as smoking, alcohol consumption and ages at menarche and menopause, in backdated designs. Given the methodological difficulties associated with the study of cancer co-morbidity in people with epilepsy, the most practical approach appears to be the follow-up of large cohorts drawn from prescription records cross-checked against records of cancer registries (Lamminpaa et al., 2002). The ratios of observed cancer incidence or mortality to expected figures for the community, region or country provide the standardized incidence ratio (SIR) and standardized mortality ratio (SMR), respectively. A SIR/SMR greater than 1 implies a carcinogenic effect whilst a ratio less than 1 indicates a cancer-protective effect. A positive drug–cancer association should carry a large relative risk (>3), persist over time and be statistically significant (Selby et al., 1989). However, it needs to be borne in mind that a drug that is given for a condition with symptoms that may mimic that of a particular neoplasm shortly before its diagnosis may appear to be associated with the neoplasm even if it is not carcinogenic. In order to offset this apparent association, referred to as ‘protopathic bias’ (Horwitz, 1985), some authors have proposed including a time lag from exposure, after which measurement of association is made (Selby et al., 1989). An association that increases over time excludes the possibility of protopathic bias and is in keeping with the concept that carcinoma risk increases with age. The International Agency for Research in Cancer (IARC) continuously reviews experimental and human data regarding potential carcinogens (International Agency for Research in Cancer, 1987). On the strength of available evidence, the agency classifies chemical carcinogens into four groups: Group 1: definitely known to be carcinogenic to humans; Group 2A: probably carcinogenic to humans; Group 2B: possibly carcinogenic to humans; Group 3: carcinogenicity unclassifiable; Group 4: probably not carcinogenic to humans. Carcinogenicity of antiepileptic drugs Animal carcinogenicity Conventional or older AEDs are drugs that have been available since before the 1980s, and these include phenobarbital, phenytoin, carbamazepine and sodium valproate. These drugs are still the mainstay of epilepsy treatment (Sander, 2004). On a worldwide basis, over 85% of people with epilepsy are treated with these drugs, and phenobarbital is the most commonly used by far. Globally, however, the majority of people with epilepsy are not treated, as there is a huge treatment gap (Meinardi et al., 2001). Phenobarbital Phenobarbital was one of the first drugs for which carcinogenicity was demonstrated in animal experiments. In the original study, a high incidence of liver tumours was Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Epidemiological approaches to human carcinogenicity Page 3 of 11 Page 4 of 11 G. Singh et al. Phenytoin Anecdotal reports of lymphoma occurring in phenytoin users (Salztein and Ackerman, 1959; Hyman and Sommers, 1966) led to carcinogenicity studies in animals (Kruger, 1970; Kruger and Harris, 1972). A few studies in selected rodent strains demonstrated that phenytoin treatment led to the development of lymphoma through chronic antigenic stimulation and immunosuppressive effects of the drug. Drug exposure was also associated with liver tumours through a promoting mechanism similar to that of phenobarbital (Chhabra et al., 1993; Diwan et al., 2001). Other studies, however, did not support a carcinogenic potential for phenytoin (Levo et al., 1975; Maeda et al., 1988). Valproate Valproate administration caused uterine adenocarcinomas in Wistar rats (Watkins et al., 1992). In contrast, an antitumour effect of valproate was discovered serendipitously, when clinical experience with the drug raised concerns about its teratogenicity, specifically the development of human neural tube defects (Blaheta et al., 2004). Its teratogenicity was then studied in vitro using neuroectodermal cell lines, such as neuroblastoma cells (Regan, 1985; Blaheta and Cinatl, 2002). An antiproliferative and differentiating effect was revealed in these experiments and was later extended to other cell lines, such as glioma, breast cancer, prostate cancer and teratocarcinoma cell lines and leukaemia progenitors (Cinatl et al., 1997; Knupfer et al., 1998; Blaheta and Cinatl, 2002). The effect was subsequently confirmed in vivo (Michaelis et al., 2004). Carbamazepine Little has been published on the carcinogenicity of this drug. It is known, however, that carbamazepine administered in doses in excess of 25 mg/kg/day for more than 2 years caused hepatocellular tumours in female, and benign interstitial tumours of the testes in male, Sprague–Dawley rats (Ciba Geigy, Product Information, 1987). Newer AEDs Newer AEDs are those that have been launched in the last 20 years. These include vigabatrin, lamotrigine, gabapentin, felbamate, topiramate, tiagabine, zonisamide, levetiracetam and pregabalin (Sander, 2004; Bialer et al., 2004). While conventional AEDs were never formally tested for carcinogenicity prior to clinical use, carcinogenicity was evaluated during drug development for these newer drugs. Male Wistar rats fed on high doses (250–2000 mg/kg) of gabapentin for long durations developed non-invasive, nonmetastatic, acinar pancreatic carcinoma (Sigler et al., 1995). The effect, however, was not considered representative of human carcinogenic risk since human pancreatic carcinomas are ductal rather than acinar. Similarly, pregabalin, a drug structurally similar to gabapentin, was shown to produce an increased incidence of haemangiosarcoma in mice fed on high doses of the drug. This was, however, felt to be speciesspecific and there is no evidence to suggest a related risk in humans (European Medicines Evaluation Agency, 2003; Pfizer, 2004). Felbamate was found to produce testicular interstitial cell tumours in male rats (McGee et al., 1998). None of the other newer AEDs have been found to be carcinogenic to animals in experiments that preceded their use in human trials. Genotoxicity studies Several genotoxicity studies using a variety of approaches have been performed for the conventional AEDs (phenobarbital, phenytoin and sodium valproate). The majority of these did not show significant derangements in genotoxic assays for these drugs (Schaumann et al., 1989a, b; Schaumann et al., 1990; Whysner et al., 1996). However, others have found an increased frequency of sister chromatid exchanges in phenytoin-treated individuals with epilepsy (Hu et al., 1990; Taneja et al., 1992; Kaul and Goyle, 1999; Kaul et al., 2001). Genotoxicity testing is now a regulatory requirement for approval of all pharmaceutical agents and has been performed ab initio for the newer AEDs. Human carcinogenicity Phenobarbital We reviewed one large multidrug, community-based, screening study (Friedman and Ury, 1980, 1983; Selby et al., 1989), five historical cohort studies that evaluated cancer risk among people with epilepsy presumably given phenobarbital (Clemmesen and Hjalgrim-Jensen, 1978, 1981; White et al., 1979; Olsen et al., 1989, 1995; Lamminpaa Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 noted when phenobarbital administration followed exposure to 2-acetyl-aminoflourene but not when given alone (Peraino et al., 1971). The hepatocarcinogenicity was reproduced in subsequent studies (Driver and McLean, 1986; Becker, 1985; Diwan et al., 1988). However, it was influenced by species, sex and age of the animal. On the basis of the above studies, it was concluded that phenobarbital is not in itself carcinogenic but is an indirectly acting, genotoxic, liver tumour promoter (Yamagi et al., 1984; Diwan et al., 1995). Phenobarbital has also been found to promote neoplasms of the thyroid (Becker, 1985). These initial animal experiments were significant because they fuelled concerns about carcinogenicity among clinicians prescribing barbiturates and led to epidemiological studies that examined carcinoma incidence or mortality in subjects receiving barbiturates (Clemmesen and HjalgrimJensen, 1978; Gold et al., 1978; Annegers et al., 1979; White et al., 1979; Shirts et al., 1986; Olsen et al., 1989, 1990, 1995; Selby et al., 1989; Goldbaher et al., 1990; Gurney et al., 1997; Lamminpaa et al., 2002). Cancer risk and anticonvulsants Phenytoin In the past, several clinical case reports and series have suggested an association between phenytoin treatment and at least three cancers (lymphoma, myeloma and neuroblastoma). An assessment of the carcinogenicity of phenytoin with specific regard to lymphoreticular malignancies was complicated by its potential to cause a variety of lymph node lesions that may mimic lymphoma upon presentation. In a review of over 100 cases of lymphadenopathy secondary to anticonvulsant use, lymph node histology was reported to be consistent with Hodgkin’s disease or even lymphoblastic lymphoma in a small, unspecified proportion; treatment with radiotherapy and chemotherapy followed, but the lymphadenopathy regressed on withdrawal of phenytoin treatment (Anthony, 1970). In an earlier report, lymphadenopathy was described in association with fever, skin rash and hepatosplenomegaly, usually developing within 3 months of phenytoin treatment (Salztein and Ackerman, 1959). The condition was characterized on histopathology by obliteration of lymph node architecture, hyperplasia and diffuse infiltration by atypical lymphoid cells, and was appropriately termed ‘pseudolymphoma’. This closely mimics mycosis fungoides, a T-cell lymphoma with cutaneous involvement, in its clinical and pathological features (Rijlaarsden et al., 1991; Cooke et al., 1998). Drug withdrawal, in order to document regression of lymphadenopathy (Anthony, 1970), or immunohistochemical studies for the demonstration of clonality (Jeng et al., 1996; Choi et al., 2003), may be the only means of distinguishing the two conditions. An initial report described six cases of lymphoma in association with phenytoin use (Hyman and Sommers, 1966). Since then, the development of lymphoma has been noted in relation to long-term phenytoin use by several authors (Gams et al., 1968; Li et al., 1975; Matzner and Polliack, 1978; Garcia Suarez et al., 1996). It is difficult to infer carcinogenicity on the basis of these clinical reports alone, particularly as some of the early descriptions of lymphoma may have been pseudolymphoma or vice versa (Hyman and Sommers, 1966). The issue is further complicated by reports of development of frankly malignant lymphoma after a period of time in what unequivocally is pseudolymphoma (Gams et al., 1968; Li et al., 1975). The occurrence of lymphoma after a quiescent period following phenytoin withdrawal for pseudolymphoma was referred to as ‘pseudo-pseudolymphoma’ (Gams et al., 1968). Recently, progression from paracortical and follicular hyperplasia to frank malignant lymphoma in two out of five cases of pseudolymphoma has been reported (Abbondanzo et al., 1995). In a larger review of 25 cases of phenytoinassociated lymphadenopathy, it was observed that, whilst benign lymphadenopathy occurred early, within weeks to months, lymphomas typically occurred after long periods of exposure. A few epidemiological studies, in particular those performed in institutionalized cohorts of patients with epilepsy, noted increased SIRs/SMRs due to lymphomas, but the Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 et al., 2002) and four studies that assessed the association between barbiturate exposure in the perinatal period and childhood brain tumours (Gold et al., 1978; Annegers et al., 1979; Goldbaher et al., 1990; Olsen et al., 1990; Gurney et al., 1997). Three studies were in hospitalized or institutionalized cohorts (Clemmesen and Hjalgrim-Jensen, 1978, 1981; White et al., 1979; Olsen et al., 1989, 1995), two, including the screening study, were AED- or barbiturate prescription-linked (Friedman and Ury, 1980, 1983; Selby et al., 1989; Lamminpaa et al., 2002) and one study was population incidence-based (Shirts et al., 1986). All except one (Clemmesen and Hjalgrim-Jensen, 1978, 1981), reported increased SIRs (from 1.1 to 1.5) for cancer, though the risk was statistically significant in only one study (White et al., 1979). Most of the increased risk was due to brain tumours, and this was significant in all five studies (SIR 2.9–5.7). This risk was, however, elevated only for the initial years of study, conforming to a protopathic bias (Feinstein, 1985) and implying that brain tumours were the cause of seizures and not a drug effect. Data regarding the risk of other systemic cancers associated with phenobarbital administration are not consistent. The Nordic studies (Clemmesen and Hjalgrim-Jensen, 1978, 1981; Olsen et al., 1989, 1995; Lamminpaa et al., 2002) demonstrated increased SIRs for hepatocellular carcinoma; however, in two of these studies the risk was confounded by other known risk factors for hepatic carcinoma, including thorotrast exposure and cirrhosis (Clemmesen and Hjalgrim-Jensen, 1978, 1981; Olsen et al., 1989, 1995). By contrast, in England, an inverse association between epilepsy and hepatocellular carcinoma was found (White et al., 1979). Several studies have reported increased SIRs for lung cancers (White et al., 1979; Friedman and Ury, 1980; Olsen et al., 1989, 1995; Selby et al., 1989; Shirts et al., 1986; Lamminpaa et al., 2002). Interestingly, in the multidrug screening community study of North California, an association was noted between prescriptions of most types of barbiturates (including phenobarbital, pentobarbital and secobarbital) and lung cancer (Friedman and Ury, 1980; Selby et al., 1989). An increased SIR for lung cancer was also noted in one population-based survey; however, smoking was a confounding factor in this study (Shirts et al., 1986). A few studies noted decreased risk of cancer in certain sites, notably urinary bladder and skin, in association with phenobarbital administration (Clemmesen and Hjalgrim-Jensen, 1978, 1981; Olsen et al., 1989, 1995). An early study reported a three-fold increased risk of childhood brain tumours with peri- or postnatal barbiturate exposure (Gold et al., 1978). Others have since questioned the strength of the association owing to confounding factors and wide confidence intervals (Annegers et al., 1979). The association between in utero barbiturate exposure and paediatric brain tumours has not been replicated in several later studies (Annegers et al., 1979; Goldbaher et al., 1990; Olsen et al., 1990; Gurney et al., 1997). Page 5 of 11 Page 6 of 11 G. Singh et al. Valproate The lack of pharmacoepidemiological data in the specific case of valproate notwithstanding, indirect evidence for a cancer-protective effect was recently presented in the form of a small, uncontrolled trial that reported therapeutic benefit with valproate administration alone or in combination with all-trans retinoic acid in myelodysplastic syndromes (Kuendgen et al., 2004). Several Phase I and II trials evaluating the role of valproate alone and in combination with other chemotherapeutic agents in malignant disorders are under way. The German-Speaking Society of Paediatric Oncology and Haematology is currently examining potential oncological benefits of valproate use in paediatric malignant glioma in a multicentre trial (Driever et al., 1999). Epilepsy and cancer survival Since several AEDs, including phenobarbital, phenytoin and carbamazepine are potent inducers of hepatic drugmetabolizing enzymes and many of the cancer chemotherapeutic agents are either metabolized in the liver or converted from prodrugs to active drugs in the liver, an increased SMR due to cancer and possibly decreased cancer survival may be attributed to induction of metabolism of the chemotherapeutic agents by enzyme-inducing AEDs (Vecht et al., 2003). Drug interactions between AEDs and cytotoxic agents were the subject of a few early anecdotal reports (Baker et al., 1992; Hassan et al., 1993; Zamboni et al., 1998) and, more recently, of systematic pharmacokinetic studies (Crews et al., 2002; Grossman et al., 1998; Kuhn, 2002; Chang et al., 2003). These interactions were recently reviewed elsewhere (Vecht et al., 2003); those relevant to the efficacy of cancer chemotherapeutic agents are summarized in Table 1. Enzyme-inducing AEDs were shown to reduce the area under the plasma concentration–time curves, decrease maximal plasma concentrations and enhance hepatic clearance of many cytotoxic agents (Baker et al., 1992; Zamboni et al., 1998; Villikka et al., 1999; Mathijssen et al., 2002; Table 1 Cancer chemotherapeutic agents that are substrates for enzyme-inducing action of AEDs Agent Reference Methotrexate Busulfan Thiotepa* Cyclophosphamide* Ifosfamide* CCNU* Vincristine Doxorubicin* Tenoposide Paclitaxel Irinotecan Relling et al., 2000 Hassan et al., 1993 Chang et al., 1995 Alberts et al., 1976, 1978 Lu et al., 1998 Levin et al., 1979 Villikka et al., 1999 Cusack et al., 1988; Sturgill et al., 2000 Baker et al., 1992; Relling et al., 2000 Fetell et al., 1997; Chang et al., 1998 Crews et al., 2002; Kuhn, 2002; Mathijssen et al., 2002; Murry et al., 2002 Zamboni et al., 1998 Grossman et al., 1998 Moorthy et al., 1997 Chang et al., 2004 Topotecan 9-Aminocampothecin Tamoxifen* y CCI-779 *Demonstrated only in animal studies; y investigational drug. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 association with phenytoin exposure was not statistically significant (White et al., 1979; Olsen et al., 1989). Moreover, no association was observed in the Northern Californian multidrug screening, Finnish AED prescription and Rochester community studies between phenytoin use and lymphoma (Friedman and Ury, 1980; Shirts et al., 1986; Selby et al., 1989; Lamminpaa et al., 2002). Multiple myeloma was anecdotally reported following phenytoin use (Matzner and Polliack, 1978; Rymard et al., 1981). However, two case–control studies of patients with multiple myeloma did not find any association between prior phenytoin use and development of myeloma (Friedman, 1986; Linet et al., 1987). Several reports describe the occurrence of neuroblastoma among children with foetal hydantoin syndrome following prenatal exposure to phenytoin (Pendergrass, 1976; Sherman and Roizen, 1976; Seeler et al., 1979; Ramilo and Harris, 1979; Allen et al., 1980; Ehrenbard and Chaganti, 1981; Jiminez et al., 1981; Lipson and Bale, 1985; Koren et al., 1989; Al-Shammri et al., 1992; Satge et al., 1998). Ten cases of neuroectodermal tumours reported up to 1992 have been reviewed (Al-Shammri et al., 1992). There were six cases of neuroblastoma (Pendergrass, 1976; Sherman and Roizen, 1976; Ramilo and Harris, 1979; Allen et al., 1980; Ehrenbard and Chaganti, 1981; Koren et al., 1989; Al-Shammri et al., 1992), one ganglioblastoma of the adrenal gland (Seeler et al., 1979), one ectodermal tumour of the cheek (Jiminez et al., 1981) and one ependymoblastoma (Lipson and Bale, 1985). Tumours were diagnosed between 1 day and 36 months after birth. They developed in the setting of a characteristic foetal hydantoin syndrome in seven cases (Pendergrass, 1976; Sherman and Roizen, 1976; Seeler et al., 1979; Ramilo and Harris, 1979; Allen et al., 1980; Ehrenbard and Chaganti, 1981; Jiminez et al., 1981), one child had unclassifiable dysmorphic features (Lipson and Bale, 1985), another coincidentally had ornithine transcarbamylase deficiency and one was apparently normal (Al-Shammri et al., 1992). In many of the reported cases, however, there was antenatal exposure to multiple AEDs, smoking or alcohol (Sherman and Roizen, 1976; Ramilo and Harris, 1979; Jiminez et al., 1981). The incidence of both foetal hydantoin syndrome and neuroblastoma has been calculated, and it was estimated that it would take 45 years for four cases of the two to occur together by coincidence rather than the four observed over 5 years (Ehrenbard and Chaganti 1981). However, other authors did not find prenatal phenytoin exposure in any of 188 cases of childhood neuroblastoma seen over 17 years in one centre in Canada (Koren et al., 1989). Our review of the literature did not find any report of neuroblastoma from 1992 onwards. Nonetheless, given the rarity of childhood neuroectodermal tumours, these case reports of neuroblastoma associated with phenytoin exposure assume significance. Cancer risk and anticonvulsants Mechanistic considerations Cancer risk The classical mechanistic view of hepatocarcinogenicity of phenobarbital was that the agent, through its enzyme-inducing properties on the cytochrome P450 system, induced the conversion of xenobiotics to activated compounds that were carcinogenic (White et al., 1979; Olsen et al., 1993). Recently, however, the tumour-promoting action of phenobarbital was attributed to its effect on gap junction-mediated intercellular communication, a process by which cells interact with each other and inhibit the growth of surrounding cells (Sugie et al., 1987). Indeed, phenobarbital was shown to decrease gap junction intercellular communication, thereby liberating tumour precursor cells from the inhibiting effects of other cells (Warner et al., 2003). Phenytoin can cause a spectrum of immunological reactions in man. A reduction in immunoglobulin levels has been noted in 20% of its long-term users (Bardana et al., 1983). Moreover, it inhibits the endogenous production of interferon-g (Fleischmann et al., 1990). The combination of these effects is thought to be the basis of its carcinogenic potential with specific regard to lymphoreticular neoplasia (Kruger, 1972). Phenytoin also modulates immune milieu in utero, as shown by increased glucocorticoid receptor expression by peripheral blood lymphocytes of children with the foetal hydantoin syndrome, perhaps explaining the tendency of children with foetal hydantoin syndrome to develop neuroectodermal tumours. Teratogenicity studies suggest, however, that phenytoin modulates the cellular responses to oxidative damage. Accordingly, oxidative mechanisms have been proposed as inherent to phenytoin’s carcinogenic and teratogenic potentials (Wells et al., 1997). Consistent with this, phenytoin is found co-oxidized during prostaglandin biosynthesis to a reactive free radical intermediate that is potentially culpable in embryopathies. The generation of this intermediate is regulated by a microsomal epoxide hydrolase, EPHX1. If cancer incidence were truly increased among patients with epilepsy, AEDs would be potential culprits. Other mechanisms need to be considered, however, as patients’ lifestyles may render them more vulnerable to, or protect them from, malignancies. Theoretically, cancer incidence would be elevated if smoking rates were higher among people with epilepsy, perhaps due to anxiety triggered by the unpredictability of seizures. The premise is supported by limited evidence of high smoking rates among people with epilepsy (Kobau et al., 2004). On balance, however, there seems to be insufficient explanation for an increased cancer incidence from lifestyle patterns associated with epilepsy. Undoubtedly, the association of brain cancers with epilepsy is a reflection of the fact that brain tumours cause epilepsy, though there are still some concerns about a milder persistent association being due to tumour-promoting effects of AEDs (Shirts et al., 1986). A biological basis—for instance, a genetic predisposition— may in part underlie the association between epilepsies and cancer. Indeed, mutations in the tumour suppressor gene, leucine-glioma-inactivated-1, were recently found to be the basis of autosomal dominant familial temporal lobe epilepsy with either aphasic or auditory seizures (Gu et al., 2002; Fertig et al., 2003). However, none of the families with this particular genotype showed an increased risk of malignancies (Brodtkorb et al., 2003). Finally, there are certain disorders that cause epilepsy and simultaneously predispose persons with the disorder to cancers. Such conditions as Down’s syndrome (Zipursky and Doyle, 1993; Ravindranath, 2003), tuberous sclerosis (Fatihi et al., 2003) and neurofibromatosis (Creange et al., 1999) are too rare to account for much of the association between cancer and epilepsy. Cancer protection In some of the cohort studies reviewed, the observed cancer incidence was found to be less than expected for certain sites. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Murry et al., 2002). For instance, in Phase I and II clinical trials of paclitaxel, people with cancer who were on enzymeinducing AEDs were shown to tolerate maximal tolerated doses that were 1.5–1.7 times routine doses (Fetell et al., 1997; Chang et al., 1998). In addition, concomitant administration of enzyme-inducing AEDs altered the profile of toxicity of paclitaxel from myelosuppression and gastrointestinal toxicity to peripheral neuropathy (Chang et al., 1998). On the basis of these studies, a 50% increase in the dose of paclitaxel was recommended when administered in conjunction with enzyme-inducing AEDs (Baker and Dorr, 2001). The clinical implications of these drug interactions are not clear at the moment. A single study determined remission and relapse rates in patients with acute lymphoblastic leukaemia who received cancer chemotherapy and AEDs concomitantly, the latter for control of seizures (Relling et al., 2000). Subgroup analysis revealed that AED administration was associated with significantly higher relapse rates in B-cell leukaemias but not in the more aggressive T-cell leukaemias. Drug interactions between AEDs and cytotoxic drugs are of particular concern in the management of brain tumours, where AEDs are commonly used to prevent seizures. It is possible that the generally poor response of malignant brain neoplasia to cytotoxic drugs may partly be due to low levels of the latter owing to induction by AEDs. In recognition of these interactions, clinical trials of developing cytotoxic agents now employ a different set of, usually higher, maximal tolerated doses of the agents in people on enzyme-inducing AEDs (Grossman et al., 1998; Kuhn, 2002; Chang et al., 2003). Further studies are required to determine whether the drug interactions between AEDs and cytotoxic agents translate into reduced cancer survival. Of the newer AEDs, oxcarbazepine and topiramate in higher doses have weak enzyme-inducing properties (Benedetti, 2000). Other newer AEDs, such as levetiracetam and gabapentin, may be preferable as firstline treatment in people with cancer who require treatment with chemotherapeutic agents. Page 7 of 11 Page 8 of 11 G. Singh et al. similar functional effects by influencing signalling mechanisms upstream of GSK3 (Mai et al., 2002). Many of these pathways are now recognized as being involved in the biological effects of several AEDs in mood disorders (Rogawski and Loscher, 2004), but may also be relevant to potential carcinoma-suppressing actions of these AEDs (Blaheta and Cinatl, 2002). Conclusions Based on available evidence, phenobarbital is carcinogenic in mice and rats and possibly carcinogenic to humans (Group 2B) (International Agency for Research on Cancer, 1987). There is evidence of carcinogenicity of phenytoin in animals; however, evidence in humans is inadequate and it also is considered possibly carcinogenic to humans (Group 2B) (International Agency for Research on Cancer, 1987). The current view of the IARC, however, does not preclude further carcinogenicity evaluation and the issue deserves more rigorous investigation. Studies so far have had limitations, particularly in view of the long duration needed to assess cancer incidence and the lack of proper control for possible confounders. In addition, in the relatively small number of studies available, selection of subjects, choice of controls, methods of ascertaining cancer incidence, duration and type of AED treatment and coding procedures have varied. Although not based upon carcinogenicity concerns, newer, non-hepatic drug metabolizing enzyme-inducing AEDs should preferentially be used rather than enzyme-inducing medications in people with cancer who undergo treatment with cytotoxic drugs. The issue of cancer incidence in people with epilepsy remains an open question. In the specific case of valproate, epidemiological studies and clinical trials of an antiproliferative effect are warranted. Acknowledgements The authors are grateful to Dr Jeremy Rees, UCL Institute of Neurology, Queen Square, London for critically reviewing the manuscript and Dr Gail Bell, University College London Hospitals, NSH Foundation Trust for her help in preparing the manuscript. No funding source was involved in the preparation of this review. G. S. is the recipient of a Commonwealth Fellowship. Conflict of interest The authors have declared no conflicts of interest. References Abbondanzo SL, Irey NS, Frizzera G. Dilantin-associated lymphadenopathy. Spectrum of histopathological patterns. Am J Surg Pathol 1995; 119: 675–85. Alberts DS, van Daalen Wetters T. The effect of phenobarbital on cyclophosphamide antitumor activity. Cancer Res 1976; 36: 2785–9. Alberts DS, Peng YM, Chen HS, et al. Effect of phenobarbital on plasma levels of cyclophosphamide and its metabolites in the mouse. Br J Cancer 1978; 38: 316–24. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 An inverse association between enzyme-inducing AED use and urinary bladder carcinoma was explained by the induction of metabolism to non-carcinogenic compounds of carcinogenic chemicals in cigarette smoke that could otherwise be implicated in the development of carcinoma at this site (Olsen et al., 1989, 1995). A low SIR of melanomas in one pharmacoepidemiological study was attributed to reduced exposure of institutionalized people with epilepsy to sunlight (Clemmesen and Hjalgrim-Jensen, 1978). Mechanisms underlying the anti-tumour effect of valproate have been the subject of intense study and were reviewed recently (Blaheta and Cinatl, 2002; Gottlicher, 2004). From the pharmacological standpoint, valproate is one of several histone deacetylase (HDAC) inhibitors, an emerging class of pharmaceutical agents in oncological treatment. Briefly, histones are DNA-associated fusion proteins which determine the relative compactness of the nucleosomes and hence the tertiary structure of DNA and its permissiveness to transcription factors (Fig. 1). Inhibition of HDAC activity leads to hyperacetylation of histones, which alters the tertiary structure of DNA and enhances the accessibility of transcription factors, resulting in the differentiation of progenitor cells. HDAC inhibitors induce cell differentiation and apoptosis and inhibit cell cycle progression in a wide range of tumour cell lines in vitro and in vivo (Gottlicher, 2004; Blaheta et al., 2004). Valproate preferentially inhibits catalytic activity of class 1 HDACs and also induces degradation of class 2 HDACs. It also inhibits angiogenesis in vitro and in vivo, manifesting as reduced expression of endothelial nitric oxide synthase (Michaelis et al., 2004). In the breast cancer cell line MCF-7, valproate induces clearance of oestrogen receptor-a through mechanisms that exclude oestrogen hormone pathways (Olsen et al., 2004). However, subtherapeutic concentrations of valproate favour tumour cell growth, an effect that is abolished by the addition of an oestrogen receptor antagonist (Olsen et al., 2004). The antiproliferative effect of valproate appears to be independent of expression by cancer cells of P-glycoprotein and multidrug resistance protein-1 (Tang et al., 2004), these being a group of proteins that are overexpressed in multidrug resistance states of cancer. It appears that the effect of sodium valproate on HDACs is independent of its antiepileptic action, though indirect evidence has recently emerged for a role of HDACs in epileptogenesis (Eyal et al., 2004). Other AEDs—for instance, topiramate and 2-pyrrolidinone-n-butyric acid, a metabolite of levetiracetam—have also been shown to possess HDAC inhibitory properties (Eyal et al., 2004). Valproate has also been shown to downregulate protein kinase C in several tumour cell lines (Yao et al., 1999; Chen et al., 2000). It also increases the expression of genes regulated by the extracellular regulated kinase-activated protein-1 pathway (Cinatl et al., 2002) and inhibits glycogen synthase kinase 3b (GSK3) (Rogawski and Loscher, 2004), an enzyme that negatively regulates signalling pathways involved in cellular proliferation. Lamotrigine has similar effects on GSK3, whereas carbamazepine may produce Cancer risk and anticonvulsants Choi TS, Doh KS, Kim SH, Jang MS, Suh KS, Kim ST. Clinicopathological and genotypic aspects of anticonvulsant-induced pseudolymphoma syndrome. Br J Dermatol 2003; 148: 730–6. Ciba Geigy. Product monograph—Tegretol; 1987. Cinatl J Jr, Cinatl J, Driever PH, Kotchetkov R, Pouckova P, Kornhuber B, Schwabe D. Sodium valproate inhibits in vivo growth of human neuroblastoma cells. Anticancer Drugs 1997; 8: 958–63. Cinatl J Jr, Kotchetkov R, Blaheta R, et al. Induction of differentiation and suppression of malignant phenotype of human neuroblastoma BE(2)-C cells by valproic acid: enhancement by combination with interferon. Int J Oncol 2002; 20: 97–106. Clemmesen J, Hjalgrim-Jensen S. Is phenobarbital carcinogenic? A follow-up of 8078 epileptics. Ecotoxicol Environ Saf 1978; 1: 457–70. Clemmesen J, Hjalgrim-Jensen S. Does phenobarbital cause brain tumors? A follow-up through 35 years. Ecotoxicol Environ Saf 1981; 5: 255–60. Cooke LE, Hardin TC, Hendrickson DJ. Phenytoin-induced pseudolymphoma with mycosis fungoides like manifestations. Clin Pharm 1998; 7: 153–7. Creange A, Zeller J, Rostaing-Rigattieri S, Brugieres P, Degos JD, Revuz J, Wolkenstein P. Neurological complications of neurofibromatosis type 1 in adulthood. Brain 1999; 122: 473–81. Crews KR, Stewart CF, Jones-Wallace D, Thompson SJ, Houghton PJ, Heideman RL, Fouladi M, Bowers DC, Chintagumpala MM, Gajjar A. Altered irinotecan pharmacokinetics in pediatric high-grade glioma patients receiving enzyme-inducing anticonvulsant therapy. Clin Cancer Res 2002; 8: 2202–9. Cusack BJ, Tesnohlidek DA, Loseke VL, Vestal RE, Brenner DE, Olson RD. Effect of phenytoin on the pharmacokinetics of doxorubicin and doxorubicinol in the rabbit. Cancer Chemother Pharmacol 1988; 22: 294–8. Diwan BA, Rice JM, Nims RW, Lubet RA, Hu H, Ward JM. P-450 enzyme induction by 5-ethyl-5-phenylhydantoin and 5,5-diethylhydantoin, analogues of barbiturate tumor promoters phenobarbital and barbital, and promotion of liver and thyroid carcinogenesis initiated by N-nitrosodiethylamine in rats. Cancer Res 1988; 48: 2492–7. Diwan BA, Henneman JR, Rice JM. Further evidence for promoterdependent development of hepatoblastoma in the mouse. Cancer Lett 1995; 89: 29–35. Diwan BA, Henneman JR, Nims RW. Enhancement of N-nitrosodiethylamine-initiated hepatocarcinogenesis by phenytoin in male F344/Ner rats at a dose causing maximal induction of CYP2B. Int J Toxicol 2001; 20: 81–7. Driever HP, Knüpfer M, Cinatl J, Wolff J. Valproic acid for the treatment of pediatric malignant glioma. Klin Pädiat 1999; 211: 323–8. Driver HE, McLean AEM. Dose response relationship for phenobarbitone promotion of liver tumors initiated by single dose dimethylnitrosamine. Br J Exp Pathol 1986; 67: 131–9. Ehrenbard LT, Chaganti K. Cancer in foetal hydantoin syndrome. Lancet 1981; 8237: 97. European Medicine Evaluation Agency. Pregabalin (Lyrica). www. emea.eu.int/humandocs/PDFs/EPAR/lyrica/084504en6.pdf. Accessed 16 November 2004. Eyal S, Yagen B, Sobol E, AltschulerY, Shmuel M, Bialer M. The activity of antiepileptic drugs as histone deacetylase inhibitors. Epilepsia 2004; 45: 737–44. Fatihi el M, Khanfri N, Niang A, et al. Renal manifestations of tuberous sclerosis complex. Ann Med Interne 2003; 154: 255–8. Fertig E, Lincoln A, Martinuzzi A, et al. Novel LGI1 mutation in a family with autosomal dominant partial epilepsy with auditory features. Neurology 2003; 60: 1687–90. Fetell MR, Grossman SA, Fisher JD, et al. Preirradiation paclitaxel in glioblastoma multiforme: efficacy, pharmacology, and drug interactions. New Approaches to Brain Tumor Therapy Central Nervous System Consortium. J Clin Oncol 1997; 15: 3121–8. Fleischmann WR Jr, Ramarathinam N, Fields EE. Effects of phenytoin on the production of interferons: differential effects on type I and type II interferons. J Biol Regul Homeost Agents 1990; 4: 107–16. Friedman G. Multiple myeloma: relation to propoxyphene and other drugs, radiation and occupation. Int J Epidemiol 1986; 15: 424–6. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Al-Shammri SA, Guberman A, Hsu E. Neuroblastoma and foetal exposure to phenytoin in a child without dysmorphic features. Can J Neurol Sci 1992; 19: 243–5. Allen RW, Ogden B, Bentley FL, Jung AL. Foetal hydantoin syndrome, neuroblastoma and hemorrhagic disease in a neonate. J Am Med Assoc 1980; 244: 1464–5. Anthony JJ. Malignant lymphoma associated with hydantoin drugs. Arch Neurol 1970; 22: 450–4. Annegers JF, Kurland LT, Hauser WA. Brain tumors in children exposed to barbiturates. J Natl Cancer Inst 1979; 63: 3. Aymard JP, Lederlin P, Witz F, Colomb JN, Faure G, Guerci O, Herbeuval R. Multiple myeloma after phenytoin therapy. Scand J Haematol 1981; 26: 330–2. Baker AF, Dorr RT. Drug interactions with the taxanes: clinical implications. Cancer Treat Rev 2001; 27: 221–33. Baker DK, Relling MV, Pui CH, Christensen ML, Evans WE, Rodman JH. Increased teniposide clearance with concomitant anticonvulsant therapy. J Clin Oncol 1992; 10: 311–5. Bardana EJ, Gabourel JD, Davies GH, Craig S. Effect of phenytoin on man’s immunity. Evaluation of changes in serum immunoglobulins, complement and antinuclear antibody. Am J Med 1983; 74: 289–96. Becker FF. Tumor phenotype and susceptibility to progression as an expression of subpopulations of initiated murine cells. Cancer Res 1985; 45: 768–73. Bell GS, Sander JW. The epidemiology of epilepsy: the size of the problem. Seizure 2001; 10: 306–14. Bell GS, Gaitatzis A, Johnson AL, Sander JW. Predictive value of death certification in the case ascertainment of epilepsy. J Neurol Neurosurg Psychiatry 2004; 75: 1756–8. Benedetti MS. Enzyme induction and inhibition by new antiepileptic drugs: a review of human studies. Fundam Clin Pharmacol 2000; 14: 301–19. Bialer M, Johannessen SI, Kupferberg HJ, Levy RH, Perucca E, Tomson T. Progress report on new antiepileptic drugs. Epilepsy Research 2004; 61: 1–48. Blaheta RA, Cinatl J Jr. Anti-tumour mechanisms of valproate: a novel role for an old drug. Med Res Rev 2002; 22: 492–511. Blaheta R, Hernáiz Driever P, Michaelis M, Cinatl J. The evolving anticancer drug Valproic acid: Insights into the mechanism and clinical studies—an update. Curr Med Chem. In press 2004. Brodtkorb E, Nakken KO, Steinlein OK. No evidence for a seriously increased malignancy risk in LGI1-caused epilepsy. Epilepsy Res 2003; 56: 205–8. Chhabra RS, Bucher JR, Haseman JK, Elwell MR, Kurtz PJ, Carlton BD. Comparative carcinogenicity of 5,5-diphenylhydantoin with or without perinatal exposure in rats and mice. Fundam Appl Toxicol 1993; 21: 174–86. Chang TK, Chen G, Waxman DJ. Modulation of thiotepa antitumor activity in vivo by alteration of liver cytochrome P450-catalyzed drug metabolism. J Pharmacol Exp Ther 1995; 274: 270–5. Chang SM, Kuhn JG, Rizzo J, Robins HI, Schold SC, Spence AM, Berger MS, Mehta MP, Bozik ME, Pollack I, Gilbert M, Fulton D, Rankin C, Malec M, Prados MD. Phase I study of paclitaxel in patients with recurrent malignant glioma: a North American Brain Tumor Consortium report. J Clin Oncol 1998; 16: 2188–94. Chang SM, Kuhn J, Wen P, Greenberg H, Schiff D, Conrad C, Fink K, Robins HI, Cloughesy T, De Angelis L, Razier J, Hess K, Dancey J, Prados MD. Phase I/pharmacokinetic study of CCI-779 in patients with recurrent malignant glioma on enzyme-inducing antiepileptic drugs. Invest New Drugs 2004; 22: 427–35. Chen G, Manji MK, Hawver DB, Wright CB, Potter WZ. Chronic sodium valproate selectively decreases protein kinase C alpha and epsilon in vitro. J Neurochem 1994; 63: 2361–4. Chen G, Masana MI, Manji HK. Lithium regulates PKC-mediated intracellular cross-talk and gene expression in the CNS in vivo. Bipolar Disord 2000; 2: 217–36. Page 9 of 11 Page 10 of 11 G. Singh et al. Koren G, Demitrakoudis D, Weksberg R, et al. Neuroblastoma after prenatal exposure to phenytoin; cause or effect. Teratology 1989; 40: 157–62. Kruger G. Effect of Dilantin in mice. I. Changes in lymphoreticular tissue after acute exposure. Virchows Arch A Pathol Anat 1970; 349: 297–311. Kruger GRF, Harris D. Is phenytoin carcinogenic? Lancet 1972; 1: 323. Kuendgen A, Strupp C, Aivado M, et al. Treatment of myelodysplastic syndromes with valproic acid alone or in combination with all-trans retinoic acid. Blood 2004; 104: 1266–9. Kuhn JG. Influence of anticonvulsants on the metabolism and elimination of irinotecan. A North American Brain Tumor Consortium preliminary report. Oncology (Huntingt) 2002; 16(8 Suppl 7): 33–40. Lamminpaa A, Pukkala E, Teppo L, Neuvonen PJ. Cancer incidence among patients using AEDs: a long-term follow-up of 28,000 patients. Eur J Clin Pharmacol 2002; 58: 137–41. Levin VA, Stearns J, Byrd A, et al. The effect of phenobarbital pretreatment on the antitumor activity of 1,3-bis(2-chloroethyl)-1-nitrosourea (BCNU), 1-(2-chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU) and 1(2-chloroethyl)-3-(2,6-dioxo-3-piperidyl-1-nitrosourea (PCNU), and on the plasma pharmacokinetics and biotransformation of BCNU. J Pharmacol Exp Ther 1979; 208: 1–6. Levo Y, Markowitz O, Trainin N. Hydantoin immunosuppression and carcinogenesis. Clin Exp Immunol 1975; 19: 521–7. Li FP, Willard DR, Goodman R, et al. Malignant lymphoma after diphenylhydantoin (dilantin) therapy. Cancer 1975; 36: 1359–62. Linet MS, Harlow SD, McLaughlin JK. A case control study of multiple myeloma in whites: chronic antigen stimulation, occupation and drug use. Cancer Res 1987; 47: 2978–81. Lipson A, Bale P. Ependymoblastoma associated with prenatal exposure to diphenylhydantoin and methylphenobarbitone. Cancer 1985; 55: 1859–62. Lu H, Wang JJ, Chan KK, Young D. Effects of phenobarbital on stereoselective metabolism of ifosfamide in rats. Drug Metab Dispos 1998; 26: 476–82. Maeda T, Sano N, Togei K, Shibata M, Izumi K, Otsuka H. Lack of carcinogenicity of phenytoin in (C57BL/6 3 C3H) F1 mice. J Toxicol Environ Health 1988; 24: 111–9. Mai L, Jope RS, Li X. BDNF-mediated signal transduction is mediated by GSK3 beta and mood stabilizing agents. J Neurochem 2002; 82: 75–83. Mathijssen RH, Sparreboom A, Dumez H, van Oosterom AT, de Bruijn EA. Altered irinotecan metabolism in a patient receiving phenytoin. Anticancer Drugs 2002; 13: 139–40. McGee JH, Butler WH, Erikson DJ. Oncogenic studies with felbamate (2-phenyl 1,3-propanediol dicarbamate). Toxicol Sci 1998; 45: 146–51. Matzner Y, Polliack Y. Lymphoproliferative disorders in four patients receiving chronic diphenylhydantoin therapy: etiological correlation or chance association. Isr J Med Sci 1978; 14: 865–9. Meinardi H, Scott RA, Reis R, Sander JW. The treatment gap in epilepsy: the current situation and ways forward. Epilepsia 2001; 42: 136–49. Michaelis M, Michaelis UR, Fleming I, Suhan T, Cinatl J, Blaheta RA, Hoffmann K, Kotchetkov R, Busse R, Nau H, Cinatl J. Valproic acid inhibits angiogenesis in vitro and in vivo. Mol Pharmacol 2004; 65: 520–7. Moorthy B, Sriram P, Randerath E, Randerath K. Effects of cytochrome P450 inducers on tamoxifen genotoxicity in female mice in vivo. Biochem Pharmacol 1997; 53: 663–9. Murry DJ, Cherrick I, Salama V, Berg S, Bernstein M, Kuttesch N, Blaney SM. Influence of phenytoin on the disposition of irinotecan: a case report. J Pediatr Hematol Oncol 2002; 24: 130–3. Oslen CM, Meussen-Elholm ET, Roste LS, Tauboll E. Antiepileptic drugs inhibit cell growth in human breast cancer cell line MCF7. Mol Cell Endocrinol 2004; 213: 173–9. Olsen JH, Boice JD Jr, Jensen JP, Fraumeni JF Jr. Cancer among epileptic patients exposed to anticonvulsant drugs. J Natl Cancer Inst 1989; 81: 1753–4. Olsen JH, Boice JD, Fraumeni JF Jr. Cancer in children of epileptic mothers and the possible relation to maternal anticonvulsant therapy. Br J Cancer 1990; 62: 996–9. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Friedman GD, Ury HK. Initial screening for carcinogenicity of commonly used drugs. J Natl Cancer Inst 1980; 65: 723–33. Friedman GD, Ury HK. Screening for possible drug carcinogenicity. Second report of findings. J Natl Cancer Inst 1983; 71: 1165–75. Gaitatzis A, Caroll K, Majed A, Sander JW. The epidemiology of comorbidity of epilepsy in the general population. Epilepsia 2004; 45: 1518–25. Gams RA, Neal JA, Conrad FG. Hydantoin induced pseudopseudolymphoma. Ann Intern Med 1968; 69: 557–68. Garcia Suarez J, Dominguez-Franjo P, Del Campo JF. EBV-positive nonHodgkin’s lymphoma developing after phenytoin treatment. Br J Haematol 1996; 95: 376–9. Gold EB, Gordis L, Tonascia JA, et al. Increased risk of brain tumors in children exposed to barbiturates. J Natl Cancer Inst 1978; 61: 1031–4. Goldbaher MK, Selby JV, Hiatt RA. Exposure to barbiturates in utero and during childhood and risk of intracranial tumors. Cancer Res 1990; 50: 4600–3. Gottlicher M. Valproic acid: an old drug newly discovered as inhibitor of histone deacetylases. Ann Hematol 2004; 83: S91–S92. Gottlicher M, Minucci S, Zhu P, et al. Valproic acid defines a novel class of HDAC inhibitors inducing differentiation of transformed cells. EMBO J 2001; 20: 6969–78. Grossman SA, Hochberg F, Fisher J, et al. Increased 9-aminocamptothecin dose requirements in patients on anticonvulsants. NABTT CNS Consortium. The New Approaches to Brain Tumor Therapy. Cancer Chemother Pharmacol 1998; 42: 118–26. Gu W, Brobtkorb E, Steinlien OK. LGI1 is mutated in familial temporal lobe epilepsy characterized by aphasic seizures. Ann Neurol 2002; 52: 364–7. Gurney JG, Mueller BA, Preston-Martin S, et al. A study of pediatric brain tumors and their association with epilepsy and anticonvulsant use. Neuroepidemiol 1997; 16: 248–55. Hahn WC, Weinberg RA. Rules for making human tumor cells. N Engl J Med 2002; 347: 1593–603. Hanahan D, Weinberg RA. The hallmarks of cancer. Cell 2000; 100: 57–70. Hassan M, Oberg G, Bjorkholm M, et al. Influence of prophylactic anticonvulsant therapy on high-dose busulphan kinetics. Cancer Chemother Pharmacol 1993; 33: 181–6. Horwitz RI, Feinstein AR. Exclusion bias and the false relationship of reserpine and breast cancer. Arch Intern Med 1985; 145: 1873–5. Hu LJ, Lu XF, Lu BQ, et al. The effect of valproic acid on SCE and chromosomal aberrations in epileptic children. Mut Res 1990; 243: 63–6. Hyman GA, Sommers SC. The development of Hodgkin’s disease and lymphoma during anticonvulsant therapy. Blood 1966; 28: 416–27. International Agency for Research on Cancer. Overall evaluations of carcinogenicity. An updating of IARC monographs, volumes 1–42. In: IARC monographs on evaluation of carcinogenic risk to humans (Suppl 7). Lyons, France: IARC; 1987. International Agency for Research on Cancer. http://193.51.164.11/ monoeval/preamble.html. Accessed 01 September 2004. Jeng YM, Tien MF, Su IJ. Phenytoin-induced pseudolymphoma; revaluation using modern biology techniques. Epilepsia 1996; 37: 104–7. Jiminez JF, Seibert RW, Char F, et al. Melanotic neuroectodermal tumor of infancy and foetal hydantoin syndrome. Am J Pediatr Hematol Oncol 1981; 3: 9–15. Kaul A, Goyle S. Genotoxicity of anticonvulsant drug phenytoin (PHT): a follow up study of PHT-untreated epileptic patients. I. Sister chromatid exchange (SCE) analysis. Teratog Carcinog Mutagen 1999; 19: 61–72. Kaul A, Kaller NR, Goyle S II. An altered proliferation response due to the anticonvulsant phenytoin in epileptic patients. Taratog Carcinog Mutagen 2001; 21: 151–64. Knupfer MM, Hernaiz-Driever P, Poppenborg H, et al. Valproic acid inhibits proliferation and changes expression of CD44 and CD56 of malignant glioma cells in vitro. Anticancer Res 1998; 18: 3585–9. Kobau R, DiIorio CA, Price PH, et al. Prevalence of epilepsy and health status of adults with epilepsy in Georgia and Tennessee Behavioral Risk Factor Surveillance System, 2002. Epilepsy Behav 2004; 5: 358–66. Cancer risk and anticonvulsants Sherman S, Roizen N. Foetal hydantoin syndrome and neuroblastoma. Lancet 1976; 2: 517. Shirts SB, Annegers JF, Hauser WA, Kurland LT. Cancer incidence in a cohort of patients with seizure disorder. J Natl Cancer Inst 1986; 77: 83–6. Sigler RE, Gough AW, de la Iglesia FA. Pancreatic acinar cell neoplasia in male Wistar rats following 2 years of gabapentin exposure. Toxicology 1995; 98: 73–82. Sturgill MG, August DA, Brenner DE. Hepatic enzyme induction with phenobarbital and doxorubicin metabolism and myelotoxicity in the rabbit. Cancer Invest 2000; 18: 197–205. Sugie S, Mori M, Takahashi M. Effect of in vivo exposure to liver tumor promoters Phenobarbital or DDT on the gap junctions of rat hepatocytes: a quantitative freeze-fracture analysis. Carcinogenesis 1987; 8: 45–51. Takai N, Desmond JC, Kumagai T, Gui D, Said JW, Whittaker S, Miyakawa I, Koeffler HP. Histone deacetylase inhibitors have a profound antigrowth activity in endometrial cancer cells. Clin Cancer Res 2004; 10: 1141–9. Taneja N, Jain S, Maheshwari MC, Tandon JK, Kucheria K. Induction of sister chromatid exchanges in phenytoin treated and untreated patients with epilepsy. Indian J Med Res 1992; 96: 302–5. Tang R, Faussat AM, Majdak P, Perrot JY, Chaoui D, Legrand O, Marie JP. Valproic acid inhibits proliferation and induces apoptosis in acute myeloid leukemia cells expressing P-gp and MRP1. Leukemia 2004; 18: 1246–51. Vecht CJ, Wagner GL, Wilms EB. Interactions between antiepileptic and chemotherapeutic drugs. Lancet Neurol 2003; 2: 404–9. Villikka K, Kivisto KT, Maenpaa H, Joensuu H, Neuvonen PJ. Cytochrome P450-inducing antiepileptics increase the clearance of vincristine in patients with brain tumors. Clin Pharmacol Ther 1999; 66: 589–93. Warner KA, Fernstrom MJ, Ruch RJ. Inhibition of mouse hepatocyte gap junctional intercellular communication by Phenobarbital correlates with strain-specific carcinogenesis. Toxicol Sci 2003; 71: 190–7. Watkins JR, Gough AW, McGuire EJ, Goldenthal E, de la Lglesia FA. Calcium valproate-induced uterine adenocarcinomas in Wistar rats. Toxicology 1992; 71: 35–47. Wells PG, Kim PM, Laposa RR, et al. Oxidative damage in chemical teratogenesis Mutation Res 1997; 396: 65–78. White SJ, McLean AEM, Howland C. Anticonvulsant drugs and cancer. A cohort study in patients with severe epilepsy. Lancet 1979; 2: 458–60. Whysner J, Ross PM, Williams GM. Phenobarbitone mechanistic data and risk assessment: enzyme induction, enhanced cell proliferation and tumour promotion. Pharmacol Ther 1996; 71: 153–91. Yamagi S, Sakamoto M, Ninomiya Y, Kamiya T. Decrease in L-type pyruvate kinase activity in rat liver by some promoters of hepatocarcinogenesis. J Natl Cancer Inst 1984; 73: 887–94. Yao CP, Mather GG, Stephens JR, Levy RH. Cytotoxicity induced by combination of valproic acid and tumour necrosis factor-alpha: implication for valproic acid-associated hepatotoxicity syndrome. Biochem Pharmacol 1999; 58: 455–9. Zamboni WC, Gajjar AJ, Heideman RL, Beijnen JH, Rosing H, Houghton PJ, Stewart CF. Phenytoin alters the disposition of topotecan and N-desmethyl topotecan in a patient with medulloblastoma. Clin Cancer Res 1998; 4: 783–9. Zipursky A, Doyle J. Leukemia in newborn infants with Down syndrome. Leuk Res 1993; 17: 195. Downloaded from http://brain.oxfordjournals.org/ by guest on October 12, 2016 Olsen JH, Wallin H, Bioce JD Jr, Rask K, Schulgen G, Fraumeni JF. Phenobarbital, drug metabolism, and human cancer. Cancer Epidemiol Biomarkers Prev 1993; 2: 449–52. Olsen JH, Schulgen G, Boice JD, Whysner J, Travis LB, Williams GM, et al. Antiepileptic treatment and risk for hepatobiliary cancer and malignant lymphoma. Cancer Res 1995; 55: 294–7. Pendergrass TW. Foetal hydantoin syndrome and neuroblastoma. Lancet 1976; 2: 150. Peraino C, Fry RJM, Staffeldt E. Reduction and enhancement by phenobarbitone of hepatocarcinogenesis induced in the rat by 2-acetylaminoflourene. Cancer Res 1971; 31: 1506–12. Pfizer. Lyrica: Summary of Product Characteristics. Code LYR327; 2004. Ramilo J, Harris NJ. Neuroblastoma in a child with hydantoin and fetal alcohol syndrome. The radiological features. Br J Radiol 1979; 52: 993–5. Ravindranath Y. Down syndrome and acute myeloid leukemia: the paradox of increased risk for leukemia and heightened sensitivity to chemotherapy. J Clin Oncol 2003; 21: 3385–7. Regan CM. Therapeutic levels of sodium valproate inhibit mitotic indices in cells of neural origin. Brain Res 1985; 347: 394–8. Relling MV, Pui CH, Sandlund JT, Rivera GK, Hancock ML, Boyett JM, Schuetz EG, Evans WE. Adverse effect of anticonvulsants on efficacy of chemotherapy for acute lymphoblastic leukaemia. Lancet 2000; 356: 285–90. Rijlaarsden U, Scheffer E, Meijer CJ, Kruyswijk MR, Willemze R. Mycosis fungoides-like lesions associated with phenytoin and carbamazepine therapy. J Am Acad Dermatol 1991; 24: 216–20. Rogawski MA, Loscher W. The neurobiology of antiepileptic drugs for treatment of nonepileptic conditions. Nat Med 2004; 10: 685–92. Salztein SL, Ackerman LV. Lymphadenopathy-induced by anticonvulsant drugs and mimicking clinically and pathologically malignant lymphoma. Cancer 1959; 12: 164–82. Sander JW. The epidemiology of epilepsies revisited. Curr Opin Neurol 2003; 16: 165–70. Sander JW. The use of antiepileptic drugs-principles and practice. Epilepsia 2004; (45 Suppl 6): 28–34. Satge D, Sasco AJ, Little J. Antenatal therapeutic drug exposure and foetal/ neonatal tumors: review of 89 cases. Pediatr Perinat Epidemiol 1998; 12: 84–117. Schaumann BA, Winge VB, Penderson M. Genotoxicity evaluation in patients on phenobarbital monotherapy by sister chromatid exchange. J Toxicol Environ Health 1989a; 28: 277–84. Schaumann BA, Winge VB, Garry VF. Sister chromatid exchanges in adult epilepsy patients on valproate monotherapy. Epilepsy Res 1989b; 3: 182–4. Schaumann BA, Winge VB, Penderson M, Kuskowski MA. Comparative effects of phenytoin and/or Phenobarbital treatment on sister chromatid exchange. Epilepsia 1990; 31: 453–7. Selby JV, Friedman GD, Fireman BH. Screening prescription drugs for possible carcinogenicity: eleven to fifteen years of follow-up. Cancer Res 1989; 49: 5736–47. Seeler RA, Israel JN, Royal JE, Kaye CI, Rao S, Abulaban M. Ganglioneuroblastoma and foetal hydantoin-alcohol syndrome. Pediatrics 1979; 63: 524–7. Page 11 of 11