Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
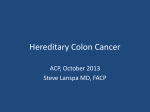
9/25/2012 Outline • Lynch syndrome/CRC overview Colon Cancer – Lynch Syndrome Tumor Testing Dana Zakalik, M.D. Beaumont Cancer Genetics Program OUWB Medical School September 19, 2012 Molecular Pathology Symposium Colorectal Cancer – Genetics of LS • Clinical characteristics/cancer risks • Management of risk • Tumor testing – MSI – IHC • Case examples Epidemiology of Colorectal Cancer • 3rd most common cancer in the U.S. – 145,000 new cases per year • 3rd most common cause of cancer-related death • Most common form of hereditary CRC is Lynch Syndrome (LS) • Stepwise progression Sporadic 60% Familial/ Multifactorial 30% – Benign mucosa polyp cancer • Effective screening prevention Rare Syndromes ~4% MUTYH Associated Polyposis (MAP) ~1% Familial Adenomatous Polyposis (FAP) ~1% Lynch Syndrome ~2-4% Cancer 1996;78:1149-67 Am J Med 1999;107:68-77 Gastroenterology 2000;119:837-53 Am J Path 2003;162:1545-8 Lynch Syndrome (formerly HNPCC: Hereditary Nonpolyposis Colorectal Cancer) KEY FEATURES: • CRC (usually dx <50 y) LYNCH SYNDROME REVIEW – Usually RT-sided, signet-ring, mucinous, poorly differentiated, Microsatellite Instability-High (MSI-H) • Endometrial cancer <50 y – Can present prior to CRC dx in women Other cancers: Ovarian, stomach, urinary tract, pancreatic, small bowel, bile duct, brain, sebaceous cysts • AD inheritance • 0 to very few polyps • GENES: MLH1, MSH2, MSH6, PMS2 “mismatch repair” genes Slides Courtesy of WBH Cancer Genetics Program 1 9/25/2012 Lynch Syndrome Colorectal cancers in LS • Amsterdam I Criteria, 1991 – Three or more relatives with CRC, which one case is a first degree relative of the other two – At least two successive generations – One or more cancers diagnosed before age 50 – FAP excluded • Distinct histologic features – Tumor infiltrating lymphocytes – “Crohn’s-like” lymphocytic infiltrate – Mucinous histology • Adenoma to carcinoma – rapid progression • Metachronous cancer risk – 16% at 10 yrs, 41% at 20 yrs • Defect in mismatch repair (MMR) system **Revised in 1999 – Amsterdam II EPCAM (TACSTD1) Mismatch Repair Genes • TACSTD1 lies upstream of MSH2 promoter – Included in LS testing schema MSH6 (10%) MSH2 (40%) MLH1 (45%) PMS2 (5%) • Deletion in the 3’ exons of TACSTD1 gene leads to hypermethylation of MSH2 promoter • Leads to silencing of MSH2 – Accounts for 25% of cases in which MSH2 absent Chr 7 Chr 3 Chr 2 • Absence of MSH2 expression on IHC can be caused by either: MSH2 mutation or EPCAM mutation (leading to methylation of MSH2) Slide courtesy of Monica Marvin, MS; CGC. MMR System and LS • DNA MMR system maintains genomic integrity by correcting DNA errors during replication • Recognizes base-pair mismatches and repairs them • Failure to repair DNA mismatches leads to genomic instability • Occurs in regions of repetitive nucleotide sequences - microsatellites 2 9/25/2012 Red Flags for Lynch Syndrome • Lynch Syndrome – Colon/ uterine cancer under age 50 – Presence of > one LS-associated cancer in same individual – Specific pathological features – 3-2-1-0 Amsterdam Criteria CLINICAL PRESENTATION • • • • 3- 3 relatives with a LS associated tumor 2- Two successive generations affected 1- At least one diagnosed under age 50 0- Polyposis syndrome ruled out * LS cancers: colorectal, endometrial, gastric, ovarian, ureter/renal pelvis, biliary tract, small bowel, pancreas, brain, sebaceous adenoma Lynch Syndrome- Cancer Risks Lynch Syndrome- Cancer Risks • Cancer Risks Avg age dx = 42-61 EC Avg age dx = 47-55 Lynch Syndrome- Cancer Risks 3 9/25/2012 Lynch Syndrome: Management Colon Cancer Surveillance Colonoscopy – every 1-2 y starting at age 20-25 y Surgery Prophylactic Colectomy Consider if: • Cancer diagnosis • Large polyp burden • Pt unwilling to undergo surveillance Endometrial /Ovarian Cancer Surveillance (no clear evidence to support) • Transvaginal U/S • Endometrial sampling • Starting at age 30-35 y Surgery • Hysterectomy • RRSO Lynch Syndrome: Management • Gastric and Small Bowel cancer (?) – No clear evidence supporting screening but may consider: – EGD with extended duodenoscopy – Capsule endoscopy for small bowel cancer – At 2-3 y intervals starting at age 30-35 y • Uroepithelial cancer – Consider annual urinalysis starting at 25-30 y • CNS cancer – Annual physical examination staring at 25-30 y • Pancreatic cancer – No recommendation, limited data Chemoprevention of LS (Burn at al Lancet 10/12) • • • • • • • • CAPP2 Trial – largest LS intervention trial 861 pts with LS (UK) ASA 600 mg vs placebo > 4 y f/u (mean 56 mos) 63% reduction in CRC (HR 0.41, p=0.02) Also decrease in non-CRC LS cancers No protection if < 2 y of intervention No increase in ulcers, GI bleed, anemia Lynch Syndrome Evaluation • Germline Testing – Molecular genetic testing of the germline genes MLH1, MSH2, MSH6, PMS2 for a deleterious mutation • Tumor screening – Microsatellite Instability (MSI) – Immunohistochemistry (IHC) LYNCH SYNDROME TUMOR TESTING Lynch Syndrome Testing • Germline Testing – Molecular genetic testing of the germline genes MLH1, MSH2, MSH6, PMS2 for a deleterious mutation • Tumor screening – Microsatellite Instability (MSI) – Immunohistochemistry (IHC) 4 9/25/2012 Germline Testing Mismatch Repair Genes • MLH1 and MSH2 (EPCAM) ~90% • MSH6 ~7-10% • PMS2 <5% • Tumor screening (MSI/IHC) allows for targeted germline testing Lynch Syndrome Testing • Germline Testing – Molecular genetic testing of the germline genes MLH1, MSH2, MSH6, PMS2 for a deleterious mutation • Tumor screening – Microsatellite Instability (MSI) – Immunohistochemistry (IHC) Microsatellite Instability (MSI) Tumor Tests to Screen for Lynch Syndrome • Microsatellite Instability (MSI) testing – Performed on DNA extracted from tumor and normal tissue – 15% of sporadic CRC cases are MSI-H • Epigenetic silencing of MLH1 due to hypermethylation – Test is positive (MSI-H) in 77-89% of LS cases – 5-10% false negative rate • Immunohistochemistry staining – Abnormal (absence of MMR protein) in 10-15% of sporadic CRC – 5-10% false negative rate MSI testing in LS • MSI-H is associated with Lynch syndrome • MSI-stable and MSI-low is not 5 9/25/2012 Lynch Syndrome ••Revised Bethesda Guidelines, 2004 Bethesda Criteria, 2004 Tumors from individuals should be tested for MSI in the following Tumors from individuals should be tested for MSI in the following situations: situations: 1. Colorectal cancer diagnosed in a patient who is less than 50 years of age. < 50 y. 1. CRC dx 2. Presence of multiple colorectal, or other Lynch syndrome‐associated 2. Presence of synchronous or metachronous LS‐associated tumors, tumors,* regardless of age. regardless of age. 3. Colorectal cancer with the MSI‐H histology diagnosed in a patient 3. CRC with MSI‐H histology in pt < 60 y. who is less than 60 years of age. 4. CRC in pt with one or more first‐degree relatives with a LS‐related 4. Colorectal cancer diagnosed in one or more first‐degree relatives tumor, with one of the cancers < 50 y with an Lynch syndrome‐related tumor, and with one of the cancers 5. CRC dx in pt with two or more first‐ or second‐degree relatives with a being diagnosed under age 50 years. LS‐related cancers, regardless of age. 5. Colorectal cancer diagnosed in two or more first‐ or second‐degree relatives, regardless of age. * Lynch syndrome (HNPCC)-related tumors include colorectal, endometrial, stomach, ovarian, pancreas, ureter and renal pelvis, biliary tract, and brain (usually glioblastoma as seen in Turcot syndrome) tumors, sebaceous gland adenomas and keratoacanthomas in Muir–Torre syndrome, and carcinoma of the small bowel. Patient #1 Patient #2 IHC results – Interpretation Immunohistochemistry (IHC) • Normal : “staining present” or “positive staining of MMR protein” • Patient 1: Absent MLH1/PMS2 • Patient 2: Absent MSH2/MSH6 • Abnormal : “Staining absent” or “negative staining for MMR protein” www.springerimages.com Five Possible Results of IHC test: 2. Abnormal – MLH1 & PMS2 Absent 1. Normal – All 4 Stains Present • 80% of the time will get this result • May need genetics evaluation if suspect LS, patient dx <45, patient has had multiple CRC primaries (meets Amsterdam II criteria) • 80% acquired methylation of MLH1 • BRAF testing • 20% will be LS MLH1 MSH6 MSH2 PMS2 6 9/25/2012 4. Abnormal – MSH6 Absent 3. Abnormal – MSH2 & MSH6 Absent • Most likely LS due to either MSH2 or MSH6 gene mutation • Posible EPCAM mutation • Most likely LS due to an MSH6 gene mutation MLH1 MSH2 MSH6 PMS2 MLH-1 MSH-6 5. Abnormal – PMS2 Absent MLH1 MSH6 PMS-2 LS is under-recognized • Most likely LS due to an PMS2 gene mutation • Older age of cancer MSH-2 MSH2 PMS2 • Amsterdam criteria too restrictive • ~25 - 50% of individuals with LS do not meet Amsterdam or Bethesda criteria • Accuracy of family history poor • Estimated 1.2% of all individuals with LS are aware of their LS diagnosis (Hampel et al 2011) • Solution – Universal Tumor Screening for LS “The Search for Unaffected Individuals with LS: Do the Ends Justify the Means?” (Hampel ’11) • Population incidence of LS: 1 in 370 • LS: 2.8% of all newly dx CRC • Estimated 829,747 of the 307,006,550 people in U.S. could have LS • < 10,000 LS cases currently diagnosed in US • 1.2% (10,000/829,747) of all individuals with LS are aware of their diagnosis Universal Tumor Screening • Reduce the morbidity and mortality from LS-related cancer in at-risk affected and unaffected relatives • Sufficient evidence to recommend offering Lynch syndrome tumor screening to all individuals with newly diagnosed colorectal cancer – Justified from a national health care system perspective – ICER is $22,522 (anything below $50K considered cost-effective) – The Evaluation of Genomic Applications and Prevention Practice (EGAPP) Guidelines, 2009 7 9/25/2012 EGAPP Guidelines Lynch Syndrome Testing • Endorsed tumor testing of all patients with CRC (cost-effective) • Many (71%) NCI designated Cancer Centers have adopted reflex IHC/MSI to screen for LS • Community hospitals less often (15%) • LSSN – Lynch syndrome screening network – Beaumont a member The most cost effective strategy involves IHC testing first and subsequent targeted gene testing (Mvundura et al 2010) • MLH1, MSH2, MSH6, and PMS2 analysis = $4000‐4500 • MSI & IHC = $900‐1000 • IHC alone = $300‐400 • Single Gene Analysis = $1000‐1400 • Beamer et.al. JCO 4/1/12 Cost-effectiveness data • Universal tumor testing of all CRC • Preferred approach: – IHC followed by BRAF mutation testing • Incremental cost-effectiveness ratio (ICER) Universal Tumor Screening for LS: The Beaumont Experience – $36,200 per life-year gained • Requires participation of at-risk relatives (3 or more) Myundura et.al. 2010 The Beaumont Experience IHC for the four Lynch associated proteins initiated January 1, 2012 for ALL newly diagnosed colorectal cancer resections ONLY – Biopsies may not provide enough normal tissue for internal control – Infrastructure in place to handle screening results and insure communication and proper follow-up (Cancer Genetics) The Beaumont Testing Schematic IHC Normal CRC > 50 yo & no family hx no personal hx IHC Abnormal Absent Staining CRC ≤ 50 or FDR w/ CRC or multiple primaries MSH2 & MSH6, or PMS2 absent MLH1& PMS2 absent Somatic tumor testing STOP Refer to Genetics STOP 8 9/25/2012 Beaumont Data 1/1/12 – 6/1/12 Beaumont Data 1/1/12 – 6/1/12 • Reflex IHC for MMR proteins • Abnormal results: (MLH1,MSH2,MSH6,PMS2) – 22 showed absent MLH1 and PMS2 (22%) – 109 IHC performed on colorectal cancer resections – 10 currently pending • Expected 15% • 20% of those expected to have LS • 80% Sporadic etiology (somatic hypermethylation MLH1/BRAF mutation) • 75 of 99 IHCs were normal (76%) – Expected 80-85% – 2 showed absent MSH6 and MSH2 (2%) • Expected 3% • Most will likely have LS • 24 / 99 IHCs were abnormal (24%) – Expected 15-20% – 0 MSH6 or PMS2 only absent • Expected 2% IHC Results Expected Observation CASE EXAMPLES Normal MLH1/PMS2 Absent MSH2/MSH6 Absent MSH6 Absent PMS2 Absent Case Example 1 n • 21-year-old male presented with a bowel obstruction due to carcinomatosis • Found to have adenocarcinoma of the colon with liver metastases – Treatment included a left hemicolectomy and palliative chemotherapy No Info n d. 70s Ca Type Unknown 60s d. 65 80s d. 80s Lymphoma Breast dx 60 No Info 60 No CScope d. 40 Uterine dx 37 Colon dx 40 • Patient was referred to cancer genetics due to his early age of diagnosis of CRC 21 Colon dx 21 24 d. 56 d. 38 Ovarian dx 27 Ovarian dx 37 d. d.70 Lung Uterine (Smoker) dx 30s Pancreatic dx ? 49 Colon dx 37 53 Polyps? d. late 70s Lymphoma dx 60-70s 60 26 Maternal Ancestry: Polish Paternal Ancestry: Irish AJ: No 9 9/25/2012 n n No Info d. 70s Ca Type Unknown 60s n 80s d. 80s Lymphoma Breast dx 60 No Info d. 65 60 No CScope 21 Colon dx 21 d. 56 d. 40 Uterine dx 37 Colon dx 40 24 d.70 d. Uterine Lung dx 30s (Smoker) Pancreatic dx ? 49 Colon dx 37 d. 38 Ovarian dx 27 Ovarian dx 37 d. late 70s Lymphoma dx 60-70s No Info n d. 70s Ca Type Unknown 60s 60 53 Polyps? 60 No CScope 26 IHC Loss of MSH2 80s d. 80s Lymphoma Breast dx 60 No Info d. 65 d. 40 Uterine dx 37 Colon dx 40 24 d. 22 Colon dx 21 MSH2 IVS4+1G>T Maternal Ancestry: Polish Paternal Ancestry: Irish d. 56 d.70 d. Uterine Lung dx 30s (Smoker) Pancreatic dx ? 49 Colon dx 37 d. 38 Ovarian dx 27 Ovarian dx 37 d. late 70s Lymphoma dx 60-70s 60 53 Polyps? 26 Maternal Ancestry: Polish Paternal Ancestry: Irish AJ: No AJ: No Case Example 2 d. 37 • 51-year-old male presented for a routine screening colonoscopy d. 89 d. 68 d. 54 Possible Cervical – Polyp in right colon • Pathology revealed a high grade adenocarcinoma • Tumor screening performed following colon resection: d. 70s d. 86 d. 70s d. 77 CHF CScope d. 72 Bladder 2 d. 16 d. 71 3 68 61 52 48 51 No CScope 51 Colon dx 51 50 d. 52 – IHC loss of MSH6 expression – MSI-H 3/6 markers 2 Maternal Ancestry: Irish • Patient presented to cancer genetics 22 24 Paternal Ancestry: Polish AJ: No d. 37 d. 89 d. 68 d. 70s d. 54 Possible Cervical d. 86 d. 70s d. 77 CHF CScope d. 72 Bladder 2 d. 16 d. 37 d. 71 d. 89 Maternal Ancestry: Irish 61 52 48 51 No CScope 51 Colon dx 51 MSH6+ p.R1005X 50 2 d. 54 Possible Cervical d. 52 d. 16 d. 77 CHF CScope d. 72 Bladder d. 71 3 68 Maternal Ancestry: Irish 22 d. 86 Gastric Tumor dx 68 d. 70s 2 3 68 d. 68 d. 70s 24 61 52 48 51 No CScope 51 Colon dx 51 MSH6+ p.R1005X Paternal Ancestry: Polish AJ: No AJ: No d. 52 2 22 Paternal Ancestry: Polish 50 24 10 9/25/2012 Maternal ancestry: Irish / German / English Paternal ancestry: German Summary d. 80 d. “old age” Colon dx ? Prostate dx ? d. ? d. 80s Cancer Colon Type dx 60s d. 70 d. 72 Colon Stomach dx ? dx ? d. 80s d. 67 “old age” heart d. 58 No info 93 Lung dx? unknown 68 – MLH1+ Colon dx 40 / 68 61 Renal dx 64 Key: Bladder dx 59 Colon cancer Stomach cancer Other cancer Renal cancer 42 46 – polyps Colon MLH1 neg dx 34 • Lynch Syndrome is the most common inherited colorectal cancer syndrome • Intense cancer surveillance and/or prophylactic surgery decreases morbidity and mortality from LS-related cancers • Family history and testing criteria alone are insufficient in identifying individuals at risk • Tumor screening is a cost-effective approach to increasing the detection rate of Lynch Syndrome 25 - Preca Bladder cancer 9 16 21 Appendix cells Beaumont Cancer Genetics Program Dana Zakalik, MD Genetic Counselors: Lindsay Dohany, MS, CGC Heidi Dreyfuss, MS Jennifer Fulbright, MS, CGC Ashley Reeves, MS 248-551-3388 http://cancer.beaumont.edu/genetics [email protected] 11